AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
A Case Study of Chronic Metabolic Acidosis, Neuropathies and Other Injuries Due to Solvent Exposure Phillip C Cantrell ABSTRACT
A 61 year old male worker (Mr. T) previously employed on a lacquer coating line of a
custom printing and packaging manufacturer contacted WorkCover during 2009 seeking
help, as he was unable to work due to his injuries. More correctly, the pain, in
combination with the amount and type of analgesic medication (including morphine
patches, Vicodin, Gabapentin, etc) he was taking to control the pain of his injuries, made
Mr. T blamed his condition on his exposure to solvents at work, particularly methyl ethyl
ketone (MEK). This was borne out by a test carried out in September 2006. On that
occasion, Mr. T had visited his doctor after work as he was feeling very ill and near
collapse. His doctor took a urine sample to test for MEK. The results came back showing
a level of MEK nearly 450 times the biological occupational exposure limit (BOEL).
Mr T would have been exposed to other chemicals besides MEK, as the lacquers with
which he worked also contained xylene and toluene, which would have flashed off with the
MEK on the line under the electrical heating elements.
A definitive diagnosis of Mr. T’s condition was the first step in determining the extent of his
disabilities and thus compensation. However, this was difficult to obtain and highlighted
the difficulty a worker with unusual injuries has in obtaining a diagnosis.
An extensive literature review with respect to MEK elucidated a number of avenues of
exploration that eventually led to a definitive diagnosis. Some of the avenues explored
• Studies that correlated urine concentrations to atmospheric levels of MEK; • Case studies of acute metabolic acidosis attributed to MEK, alcohol and
• Case studies that showed neuropathies have been induced by MEK exposure
along with other solvents that Mr. T had been exposed to, particularly xylene.
Eventually, a dual diagnosis of chronic metabolic acidosis leading to chronic
hypocalcaemia with underlying poly and peripheral neuropathy was finally made and
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
accepted by Mr. T’s doctor and attending medical specialists, and compensation is
GLOSSARY BOEL - Biological Occupational Exposure Limit. The level that is placed on a workplace
substance or its metabolite/s encountered in biologically derived specimens,
BEI - Biological Exposure Indices, a term used by the American Conference of
Governmental Hygienists. Generally equivalent to BOELs.
ES-TWA – exposure standard – time weighted average. LC50 - a statistically derived estimate of a gas, vapour or dust expressed in parts per
million (ppm), milligrams per cubic metre (mg/m3) or some other units, that will kill
50% of an animal test group under specified conditions. Generally the time is given
LT50 - represents the time of exposure after which 50% of the animals died within 14 days MEK - methyl ethyl ketone or 2-butanone. TLV – TWA - threshold limit value - time weighted average. WCA - WorkCover Authority of NSW, now known as WorkCover NSW. INTRODUCTION
A review of WorkCover NSW cases and anecdotal evidence from doctors and workers
indicates that it is often difficult for a worker suffering chronic injuries as a result of
exposure to chemicals (particularly solvents) to get a definitive diagnosis that links the
injuries to chemical exposure . A worker with a number of concurrent illnesses from
chemical exposures will find it even more difficult to receive appropriate diagnoses, as
occurred to the subject of this case study.
Often, workers excessively exposed to chemicals with neurological sequelae are unaware
that their illnesses (injuries) are work related. This is often compounded when physicians
are ignorant of their patients’ work exposure to toxins and diagnose such illnesses without
reference to its root cause. This leaves the OH&S professional a difficult forensic task of
fitting the workers’ injuries and any available data into a suitable scenario that builds a
case aimed at determining cause and effect.
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
THE SUBJECT – MR. T
At issue is Mr T, a 61 year old cardboard sheeting coating line operator. In 2006 Mr. T
had been found to have a urinary methyl ethyl ketone (MEK or 2-butanone) level nearly
450 times the current recommended biological occupational exposure limit. The urine
analysis was undertaken according to method WCA.163 at the WorkCover Laboratories.
Neurological assessments undertaken by Mr. T were not thorough and comprised of
stimulus and response observations, percussive reflexes and Mr. T’s reported symptoms.
The standard tests that must be undertaken for a diagnosis of peripheral and/or
polyneuropathy include the review of the clinical history and which must be confirmed with
electro-diagnostic techniques, most commonly electromyography (EMG) and nerve
conduction studies. Facial nerve and blink reflex testing also are commonly undertaken.
Apparatus, such as the neurometer, vibrometer, and sensory nerve perception threshold-
testing devices can also be useful as diagnosis tools.
When Mr. T contacted WorkCover NSW in 2009 he was in severe chronic pain that could
only be eased by taking a vast number of strong analgesics. He was suffering from
cramps in his legs and arms along with ailments including bloody diarrhoea, headaches,
trembling, mood swings, loss of balance, depression, loss of hair, height, and teeth (he
had only 3 remaining teeth), breathing problems, carpal tunnel syndrome, type 2 diabetes,
calcified arteries in his legs, fatigue, etc. There was no evidence from Mr. T’s family
history of a genetic explanation for these symptoms. His previous medical history, along
with X-rays, Cat scans, MRI’s, ultrasounds, bone density scans and arterial dopplers were
all sighted by the author, along with the urine analysis for MEK.
Mr. T’s workers compensation claim was refused by the insurer because his nerve
conduction studies were not consistent with neuropathy. This was confounded by
symptoms such as calcified arteries, veins and joints which could not be attributable to the
exposures to solvents at the workplace. Other medical professionals consulted were
puzzled by the multiple symptoms and the supposedly normal nerve conduction studies
and as a result they also could not make an appropriate diagnosis.
Exposure to solvents
Many of the neurological symptoms Mr. T displays could be associated with chronic
exposure to solvents. Indeed, Mr. T stated he was able to work on the coating line for
nearly 30 years when the solvent fumes made it impossible for many others to do so. He
could have developed a degree of tolerance to solvent vapours, or even a habituation, as
he said that he “certainly missed the smell of the place and often longed for it”.
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
Mr. T reported that MEK was used to cut the viscosity of the PVC gloss coating that was
applied to printed cardboard sheeting on the coating line. Prior to the introduction of MEK,
Mr. T said that xylene and toluene has been used, and that the PVC gloss coating also
had either xylene or toluene in it. Assuming this to be correct, these solvents would also
have been liberated when the MEK was flashed off on the line under the electrical heating
Mr. T’s employer no longer uses MEK as a solvent.
Toxicology of the solvents
MEK, xylene, toluene and other solvents are absorbed into the body by breathing them as
chemical vapours or absorbing them in vapour or liquid form through the skin. There are
many factors that affect this uptake, such as temperature, sweating, skin’s vascularity,
skin thickness, exposure time, solvent concentration, etc.
Once these solvents are absorbed into the body, solvents can either pass out of the body
unchanged through breath, sweat, urine or faeces (hence, the MEK in Mr. T’s urine).
Some may be stored in body fat for a period, or will be metabolized in the body, primarily
through the liver, mainly to be excreted in urine or faeces. Whilst the body will generally
rid itself of the majority of solvents absorbed, neuropathic symptoms have been
associated with long-term occupational solvent exposure that occurs in groups such as
industrial painters, paint manufacturers, refinery workers, laboratory workers, etc (NIOSH
EVALUATION OF MR T.’S EXPOSURE TO SOLVENTS
Mr. T’s exposure to MEK level can be evaluated in terms of the Biological Occupational
Exposure Limit or BOEL. A BOEL is the level that is placed on a workplace substance or
its metabolite/s encountered in biologically derived specimens, generally blood or urine. If
a worker’s results significantly or persistently exceed the BOEL there is an increased risk
of adverse health effects. There are only about 70 recognised BOELs but, luckily, MEK is
one of them. Table 1 shows the limits for MEK, toluene and xylene, expressed as BOELs
and/or the equivalent Biological Exposure Indices (BEIs) as adopted by the American
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
Table 1: Biological Occupational Exposure Limits – Biological Exposure Indices CHEMICAL BOEL/BEI
2 mg/L (milligrams of MEK per litre of urine)
mg/100 ml (milligrams per 100 ml of blood),
0.5 mg [o-cresol]/L - urinary metabolite, and
2.5 gm (hippuric acid)/gm creatinine* - urinary metabolite
0.3 mg/100 ml(milligrams per 100 ml of blood), and
1.5 gm (methylhippuric acid)/gm creatinine - urinary
* Creatinine is used to determine the concentration of the urine and hence the
The advantage of using BOELs is that they represent the sum total of exposure from all
the possible routes of entry into the body, in this case inhalation and skin absorption.
Calculating atmospheric levels of MEK
Mr. T’s urinary MEK level was 896 milligrams per litre of urine (mg/L). This is 448 times
the BOEL set for MEK in urine of 2 mg/L. There is a way of roughly determining the
atmospheric concentration of MEK (ES-TWA) Mr. T would have been exposed to. This is
achieved by the knowledge that the atmospheric level of MEK directly relates to the
urinary concentration of MEK. See the following calculations:
The linear regression equations connecting MEK by Cu (urinary concentration) in
micrograms per litre (µg/L) of urine, and Ca, the air exposure concentration in parts per
million (ppm), from 2 out of 4 reported field studies (Que Hee 1993) are as follows:
By simple substitution the above equations derive
Now substituting Cu in both equations (Cu = 896,000 µg/L) we get:
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
These are incredibly high levels1, above the lower explosive level and approaching the
Distribution of MEK in the body
Another way of determining Mr. T’s possible exposure is to look at how MEK is distributed
throughout the body. MEK is nearly equally soluble in water, blood and oil. Distribution
coefficients between water/air, blood/air and oil/air are 254, 202 and 263 respectively
(Sato and Nakajima 1979), which implies that MEK distributes reasonably uniformly to the
various soft tissue compartments. This relationship was further investigated by the
American Conference of Governmental Industrial Hygienists in 1992 when the TLV – TWA
for MEK of 200 ppm was found to correspond to MEK concentrations in urine and blood
calculated to be 5.1 mg/L and 3.8 mg/L as a BEI respectively (US EPA 2003).
Hence, Mr. T’s urinary level of MEK could correspond to a blood level of 3.8 / 5.1 X 896 =
668 mg/L. However, at concentrations of urinary MEK with which Mr. T presented, such a
calculation is probably meaningless as a total saturation of the body has been achieved
and a blood/urine MEK ratio of unity has been approached.
Acute animal and human studies
The effects of MEK exposure to mammals vary from transient effects on behaviour or
neurophysiology detected after repeatedly exposing rats and baboons to concentrations
as low as 295-590 mg/m3 (100 to 200 ppm) (DiVincenzo et al 1976, WHO 1993) to an
LT50 for mice and rats exposed to 92,239 ppm 2-butanone of 3 and 0.5 hours, respectively
LC50 studies for MEK in rats suggest a LC50 of about 8,000 ppm over an 8 hour exposure
(US PHS 1992). For further comparison, the lower and upper explosive limits for MEK are
1.9% (19,000 ppm) and 10.0% (100,000 ppm) respectively (US EPA 2003). However, at
these super high concentrations the linear regression equation is probably compromised.
MEK has a low order of toxicity after single oral exposure to rodents. Estimates of the
acute oral median lethal dose in rats range from ~ 2.5 to 5.6 grams per kilogram of body
weight (gm/Kg) (Smyth et al 1962; Kimura et al 1971). For a 70 kg human, these doses
would represent 175 to 392 gm of MEK. Assuming MEK is distributed evenly throughout
the body, and that body tissue, blood and urine have a similar density (~1), then a fatal
dose of MEK in blood/urine would be in the order of 2,500 to 5,600 mg/L. Mr. T’s
exposure of 896 mg/L is significant indeed.
1 The Australian exposure standard (TWA) for MEK is 150 ppm (NOHSC 1995).
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
There are no reports of human fatalities due to exposure to MEK alone, either by
inhalation or ingestion. The only documented case of a person orally exposed to MEK
alone was documented by Kopelman and Kalfayan (1983), who describe non-
occupational, acute toxicity from ingestion of MEK. A 47 year old woman who
inadvertently ingested an unknown amount of MEK was unconscious, hyperventilating
and suffering from severe metabolic acidosis upon hospital admission. Her plasma
concentration of MEK was 950 mg/L. After an uneventful recovery, she was discharged
from the hospital. This is an important case as the woman’s plasma level was just above
Mr. T’s urine level. Considering the even equilibrium postulated for MEK in
blood/plasma/urine/soft tissue, at the time his urine was taken, Mr. T would have been
very close to this woman’s condition, the only difference being that Mr. T had spent
decades exposed to MEK on a daily basis. The acute severe metabolic acidosis the
woman suffered might give a clue to Mr. T’s other symptoms.
(Chronic) Metabolic Acidosis
Mr. T’s symptoms, including the loss of teeth, hair and height, calcified arteries and
rheumatic symptoms in his hands and wrists (carpel tunnel), might be explained by
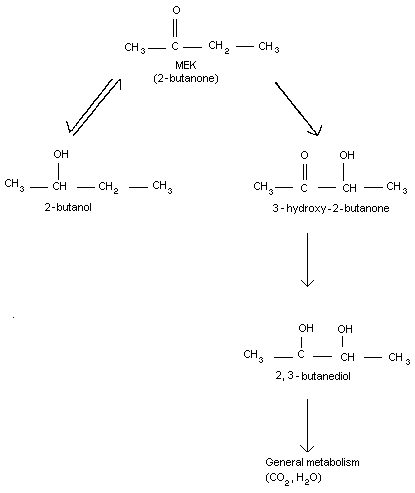
chronic metabolic acidosis, as suggested by the case study mentioned above. Chronic
metabolic acidosis comes about by the metabolism of solvents, MEK in particular, into
carbon dioxide and water. See Figure 1 below.
Figure 1 Metabolic pathway of methyl ethyl ketone in mammals
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
Carbon dioxide is a weak acid and chronic acidosis interferes with the body’s normal
calcium metabolism, as well as a host of other biological equilibrium mechanisms in the
body, due to the lower blood/plasma pH. There is ample evidence to support this
scenario in the medical and OH&S literature.
Chronic Hypocalcaemia Caused by Chronic Severe Metabolic Acidosis
Total body levels of calcium are controlled by a complex feedback system. Parathyroid
hormone (PTH) directly targets the bone and kidneys to increase serum calcium levels.
Indirectly through vitamin D, it causes intestinal calcium absorption. Vitamin D directly
targets gastrointestinal absorption of calcium to increase calcium levels. Calcitonin lowers
calcium by targeting bone, renal and gastrointestinal losses. Calcium is also affected by
Metabolic acidosis decreases renal calcium reabsorption. Several mechanisms have
been implicated, including an increase in ionised serum calcium levels with suppression of
parathyroid hormone release. However, experiments with parathyroidectomised animals
have clearly demonstrated that acidosis per se blocks the reabsorption of calcium
independently of the level of parathyroid hormone. This blocking of calcium reabsorption
leads to a condition known as hypocalcaemia (Boden and Kaplan 1990).
According to Bourke and Delaney (1993), the degree of muscle spasm reflects the
patient's serum calcium level, stating that, initially, hypocalcaemia will produce
paresthesia in the fingers, toes and around the lips, progressing to muscle tension and
carpopedal spasms. Other symptoms may include muscle weakness, twitching or
cramps, fatigue, palpitations, hyperactive deep tendon reflexes and choreiform
movements. They cited symptoms of chronic hypocalcaemia including changes of mental
status, double vision, difficulty swallowing, abdominal cramps, dry, scaly skin, alopecia,
brittle nails and thin, patchy scalp and eyebrow hair. Mr. T exhibited all these symptoms.
Rose and Post (2001) cite chest pain, palpitations, headache, altered mental status,
decreased visual acuity, nausea, vomiting, abdominal pain, altered appetite (either loss of
or increased) and weight loss (longer term), muscle weakness and bone pains as
symptoms of metabolic acidosis, all symptoms Mr. T has previously complained of.
Neurotoxicology
Other symptoms that Mr. T suffers from mostly appear to be neurological in nature.
Although MEK does not appear to be highly neurotoxic itself, the US EPA (2003) has
reported three case studies of long-term human exposures to MEK that indicate severe
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
neurological damage to the individuals concerned, although, as was the case with Mr. T,
nerve conduction studies were normal in one case.
However, Mr. T was also exposed to other solvents such as xylene, toluene and napthas
over his 30 years work history. These other solvents, particularly n-hexane or methyl
butyl ketone, could have contributed to Mr. T’s neuropathies.
Mr. T’s exposure to xylene must have been significant, particularly as xylene was used as
a dilutant to cut the viscosity of the gloss lacquers for a number of years prior to the
introduction of MEK. Even then, xylene was still part of the lacquer and would have been
liberated into Mr T’s breathing zone as the solvents flashed off under the electric line
Xylene has shown positive associations between exposure and peripheral nervous
system dysfunction in 11 epidemiological studies of painters or other subjects with xylene
exposure (Rutchik 2009). One study in particular stands out where seven men aged 17-
22 who worked on a lacquer coating line “developed severe distal symmetrical
polyneuropathy after repeatedly inhaling … lacquer thinner that was composed
predominantly of xylene. All 7 were disabled permanently with motor weakness. One man
died, 3 remained wheelchair bound, and 3 could walk but demonstrated varying degrees
of weakness. Pathologic specimens revealed evidence of peripheral neuropathy.”
Mr. T’s exposure to toluene would also have been significant, as it was an integral part of
Chronic toluene abuse in humans has been associated with neurotoxic symptoms,
narcosis and death. Various cases of chronic abuse documented by the US Department
of Health and Human Services (US DHHS 2000) indicate that prolonged exposure to
toluene results in permanent damage to the human central nervous system, including
reduced ability in tests of cognitive and neuromuscular function amongst people whose
occupations exposed them to average concentrations as low as 80–150 ppm.
Abnormalities in MRI and brainstem auditory evoked response results were still present in
chronic abusers who had refrained from toluene exposure for two to nine months. Other
studies indicated apparent neurological damage to hearing and colour vision caused by
chronic exposure to toluene from average concentrations as low as 30–130 ppm
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
DISCUSSION: KNOWN HEALTH IMPACTS AND RESULTS AND COMPARISON TO THE TOXICOLOGY OF THE SOLVENTS
Mention has been made of the difficulty a chronically injured worker might face in getting
compensation when his injuries are confusing and his workplace or work regimen no
longer includes the agent that elicited the injury. Mr. T is a case in point, having two
distinct occupational diseases stemming from his solvent exposure:
1. the solvent induced nerve damage that led to peripheral and polyneuropathies and
2. the hypocalcaemia also caused by Mr. T’s massive solvent exposure.
Together, these conditions apparently confused the medical practitioners he saw.
Unfortunately, Mr. T’s neuropathies have showed no sign of abating and laser cutting of
some of his nerves has been considered to provide longer term analgesia. The prognosis
of Mr. T’s neuropathies is not good. However, some of the hypocalcaemia symptoms
have subsided, such as the carpopedal spasms, which initially was mistakenly diagnosed
as carpel tunnel syndrome. Other symptoms have improved, for example his finger and
toenails have lost their malformed and brittle appearance, the cramps in his feet have
subsided, as one would expect with the cause of the carpopedal spasms removed. Mr.
T’s type 2 diabetes has also improved to such an extent that medication is no longer
required (this is not altogether unexpected, as calcium plays a part in normal glucose
homeostasis). Other muscular cramps have also abated in all his extremities.
It is interesting to note that a review of the literature shows no mention of occupationally
acquired chronic hypocalcaemia from chronic exposure to MEK or any other solvent. A
simple Google search will easily indicate the connection between acidosis and solvent
abusers and alcoholics, but they are notoriously difficult groups to study, generally having
a plethora of other complicating lifestyle factors such as malnutrition, disease and other
drug abuses. Unlike Mr. T, solvent abusers and alcoholics generally don’t spend 60 hours
a week constantly imbibing their pleasure at work, combined with good nutrition and a
family life. Complicating factors such as alcohol did not play any part in Mr. T’s case as
Mr. T’s initial medical assessments indicated the employment of inadequate neurological
determination techniques, with some physicians appearing to display a lack of even basic
understanding of occupational toxicology with respect to solvent exposure. There would
seem to be a dearth of physicians with toxicology skills available to the Workers
Compensation system and hence someone like Mr. T could easily fall through the cracks.
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
There are probably more workers suffering from chronic solvent induced neuropathies or
other chronic sequelae that have not been detected by the system and are missing out on
inadequate medical investigations leading to an incorrect or no diagnosis
workers often being unaware that their injuries are work-related
workers’ health being severely compromised by the time their illness is diagnosed
workers lacking the strength and/or having insufficient funds to mount a legal case
inadequate occupational evaluations being carried out at workplaces to support any
workers blaming themselves for their predicament
Unfortunately, as an occupational health and safety professional, I have seen many
CONCLUSION
The main conclusion that this case study reaches is that Mr. T was suffering from two
occupational diseases caused by the same massive solvent exposure. These diseases
were chronic hypocalcaemia and peripheral and poly neuropathy.
Chronic hypocalcaemia brought about by solvent-induced chronic metabolic acidosis has
not been described in the occupational medical literature and could definitely form the
basis for further solvent studies, particularly of spray painters and printers who have high
solvent exposures, to see if they are suffering from any of the symptoms Mr. T
Mr. T’s case study is interesting considering his tenacious desire to carry out his job in the
face of solvent levels other workers could not bear. A habituation to the solvent could
explain this phenomena: as with other addictions, addicts can be blind to the life-
threatening side-effects so obvious to others.
It also became evident that there was not enough medical toxicological knowledge
available to achieve the quick diagnosis of a chronically injured worker with multiple
sequelae attributable to solvent exposure. The delays, mistakes and oversights made
with Mr. T should be investigated and neurological assessments expanded to achieve
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
RECOMMENDATIONS
This case study has shown an area of chronic solvent exposure that has not been
explored ie. chronic hypocalcaemia. It is well known that toluene, xylene, ethanol,
acetone and MEK, the solvents used in many paints and thinners, can cause acidosis.
However, what is not known is to the extent to which they may affect exposed workers
calcium metabolism. It might be assumed that the blood’s natural pH buffering
mechanism might ward off the worst consequences, but when lifestyle factors such as
alcohol consumption, poor diet, etc impinge, they could over-ride the bodies blood
buffering system. The assessment of solvent exposed workers for any signs of possible
hypocalcaemia may be a fertile area of enquiry.
Such investigations most likely would require biological monitoring and a worker
questionnaire with respect to dental health, diet, alcohol consumption, pains and cramps,
general well being, etc. Most importantly neuropathies need to be evaluated in a much
more scientific way to achieve appropriate diagnosis. The majority of physicians do not
have the required electro-diagnostic apparatus to do a definitive diagnosis.
REFERENCES
Boden, SD, Kaplan, FS 1990, ‘Calcium homeostasis’. Orthop Clin North Am. Jan
Bourke E, Delaney, V 1993, ‘Assessment of hypocalcaemia and hypocalcaemia’, Clin Lab
DiVincenzo GD, Kaplan CJ, & Dedinas J 1976 ‘Characterization of the metabolites of
methyl-N-butyl ketone, methyl iso-butyl ketone, and methyl ethyl ketone in guinea-pig serum and their clearance’, Toxicology and Applied Pharmacology, 36 pp. 511-522.
Hayes, AW (Ed) 2007, Principles and methods of toxicology, Informa Healthcare, New
Kimura, E, Ebert, D, Dodge, P 1971, ‘Acute toxicity and limits of solvent residue for
sixteen organic, solvents’, Toxicology and Applied Pharmacology 19 pp. 699-704.
Klimisch, H 1988, ‘The inhalation hazard test; principle and method’, Archives of Toxicology 61 pp. 411-416, Springer-Verlag.
Kopelman, P, Kalfayan, P 1983, ‘Severe metabolic acidosis after ingestion of butanone’,
British Medical Journal 286 pp. 21-22.
NIOSH (National Institute for Occupational Safety and Health) 1987, Current Intelligence Bulletin #48: Organic Solvent Neurotoxicity, viewed 26 July 2009, <http://www.cdc.gov/mmwr/preview/mmwrhtml/00000918.htm>
NOHSC (National Occupational Health & Safety Commission) 1995, Adopted National Exposure Standards for Atmospheric Contaminants in the Occupational Environment [NOHSC:1003(1995)]
Que Hee, SS 1993, Biological Monitoring: An Introduction, Van Nostrand Reinhold, New
Rose, BD, Post, TW 2001, Clinical Physiology of Acid-Base and Electrolyte Disorders,
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
Rutchik, JS 2009, Toxic Neuropathy, viewed 26 July 2009,
<http://emedicine.medscape.com/article/1175276-overview>.
Sato, A, Nakajima, T 1979, ‘Partition coefficients of some aromatic hydrocarbons and
ketones in water, blood and oil’, British Journal of Industrial Medicine 36 pp. 231-234.
Smyth, HF, Carpenter, CP, Weil, CS, Pozzani, UC, & Striegel, JA 1962, ‘Range-finding
toxicity data: List VI’, American Industrial Hygiene Association Journal 23 pp. 95-107.
US DHHS (Department of Health and Human Services, Agency for Toxic Substances and
Disease Registry) 2000, Toxicological Profile for Toluene, p. 57, viewed 28 July 2009, <http://www.atsdr.cdc.gov/toxprofiles/tp56.pdf>.
US EPA (Environmental Protection Agency) 2003, Toxicological Review of Methyl Ethyl Ketone (EPA 635/R-03/009) pp. 19-20, viewed 4 August 2009 <http://www.epa.gov/iris/toxreviews/0071-tr.pdf>.
US PHS (US Public Health Service - Agency for Toxic Substances and Disease Registry)
1992, Toxicological Profile for 2-Butanone.
WHO (World Health Organisation) 1993, ‘Methyl Ethyl Ketone’, Environmental Health Criteria 143, Geneva, viewed 2 August 2009, <http://www.inchem.org/documents/ehc/ehc/ehc143.htm>.
The Adverse Effects of Chemical Treatment of Depression in Children The intent of this article is to present to the field doctor the story of growing usage and adverse effects of newer types of antidepressants (selective serotonin reuptake inhibitors, or SSRIs) among children and adults. This is not an attempt to discourage entirely the use of antidepressants by children, but rather, to prov
A randomized controlled trial of the efficacy of rosiglitazone and clomiphene citrate versus metformin and clomiphene citrate in women with clomiphene citrate–resistant polycystic ovary syndrome Abdulrahim A. Rouzi, FRCSC, a and Mohammed Salleh M. Ardawi, Ph.D., F.R.C.Path. ba Department of Obstetrics and Gynecology, and b Clinical Biochemistry, Faculty of Medicine, King Abdulaziz Universi
 AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
There are no reports of human fatalities due to exposure to MEK alone, either by
inhalation or ingestion. The only documented case of a person orally exposed to MEK
alone was documented by Kopelman and Kalfayan (1983), who describe non-
occupational, acute toxicity from ingestion of MEK. A 47 year old woman who
inadvertently ingested an unknown amount of MEK was unconscious, hyperventilating
and suffering from severe metabolic acidosis upon hospital admission. Her plasma
AIOH2009 Conference, 5 – 9 December 2009, Canberra, ACT, Australia
There are no reports of human fatalities due to exposure to MEK alone, either by
inhalation or ingestion. The only documented case of a person orally exposed to MEK
alone was documented by Kopelman and Kalfayan (1983), who describe non-
occupational, acute toxicity from ingestion of MEK. A 47 year old woman who
inadvertently ingested an unknown amount of MEK was unconscious, hyperventilating
and suffering from severe metabolic acidosis upon hospital admission. Her plasma