Effect of continuous combined therapy with vitamin K and
vitamin D on bone mineral density and coagulofibrinolysis
Takahisa Ushiroyama *, Atushi Ikeda, Minoru Ueki
Department of Obstetrics and Gynecology, Osaka Medical College, 2-7 Daigaku-machi, Takatsuki, Osaka 569-8686, Japan
Received 28 July 2000; received in revised form 7 February 2001; accepted 14 September 2001
Abstract Objecti6es: To investigate the therapeutic effect of combined use of vitamin K and D on vertebral bone mineral
density in postmenopausal women with osteopenia and osteoporosis. Subjects and methods: We enrolled 172 womenwith vertebral bone mineral density B0.98 g/cm2 (osteopenia and osteoporosis) as measured by dual-energy X-rayabsorptiometry. In this study, we employed the criteria for diagnosis of osteopenia and osteoporosis using dual energyX-ray absorptiometry proposed by the Japan Society of Bone Metabolism in 1996. Subjects were randomized intofour groups (each having 43 subjects in vitamin K therapy group, vitamin D therapy group, vitamin K and D
combined therapy group, or a control group receiving dietary therapy alone) and treated with respective agents for2 years, with bone mineral density was measured prior to therapy and after 6, 12, 18, and 24 months of treatment. The bone metabolism markers analyzed were serum type 1 collagen carboxyterminal propeptide (P1CP), serum intactosteocalcin, and urinary pyridinoline. Tests of blood coagulation function consisted of measurement of activatedpartial thromboplastin time (APTT) and analysis of concentrations of antithrombin III (AT III), fibrinogen, andplasminogen. Results: Combined therapy with vitamin K and D for 24 months markedly increased bone mineral
density (4.92 97.89%), while vitamin K alone increased it only 0.13595.44%. The bone markers measured, revealed
stimulation of both bone formation and resorption activity. We observed an increase in coagulation and fibrinolyticactivity that was within the normal range, suggesting that balance was maintained in the fibrinolysis – coagulationsystem. Conclusions: Continuous combination therapy with vitamin K and D may be useful for increasing vertebral
bone mass in postmenopausal women. Furthermore, the increase in coagulation function observed during this therapywas within the physiological range, and no adverse reactions were observed. 2002 Elsevier Science Ireland Ltd. Allrights reserved. Keywords: Vitamin K ; Vitamin D ; Bone mineral density; Postmenopause; Coagulofibrinolysis
1. Introduction
* Corresponding author. Tel.: + 81-726-83-1221; fax: + 81-
Postmenopausal women experience accelerated
bone loss, which leads to osteoporosis and in-
0378-5122/02/$ - see front matter 2002 Elsevier Science Ireland Ltd. All rights reserved.
PII: S 0 3 7 8 - 5 1 2 2 ( 0 1 ) 0 0 2 7 5 - 4
T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
creased risk of development of fractures in the
tial to this process. Vitamin K , the human-acti-
spine (vertebral crush fractures), forearm (Colles’
vated form of vitamin K, is said to promote the
fractures) and hip. Osteoporotic fractures of the
healing of bone fractures, to have a therapeutic
spine and forearm are associated with significant
effect on osteoporosis, and to inhibit bone resorp-
morbidity, but the most serious consequences of
tion [17,18]. It may also play a role in bone
bone loss arise in patients with hip fracture, which
metabolism other than the g-carboxylation of os-
is associated with a significant increase in mortal-
teocalcin. The addition of vitamin K and acti-
ity (15 – 20%), particularly in the elderly [1]. Sev-
eral approaches are currently available to prevent
osteoblasts has been shown to promote calcifica-
and treat osteoporosis, including dietary modifica-
tion [19]. In Japan, the incidence of fractures in
tions and drugs which inhibit bone resorption.
the eastern part of the country is lower than that
There are now a variety of treatment approaches
in the west, a phenomenon that may be associated
available for the management of osteoporosis.
with differences in food culture between the two
Inhibitors of bone resorption, including calcium,
regions, specifically, in the consumption of natto
the vitamin Ds, ipriflavone, bisphosphonates, cal-
(fermented soybeans). Natto is rich in the MK-7
citonins and gonadal steroids have been variously
(menaquinone-7) form of vitamin K , which has
shown to prevent bone loss or to reduce fractures
the same effect as the MK-4 form of vitamin K ,
[2 – 4]. The effect of vitamin supplements on bone
one of the medications currently used to treat
metabolism indices in patients with osteopenia
osteoporosis. Estrogen is an agent of choice for
and osteoporosis has received scant attention in
both prevention and treatment of postmenopausal
the literature. However, some authors have re-
osteoporosis; however, once estrogen treatment is
ported that vitamin D and K may prevent bone
discontinued, bone mass density drop fairly
loss and fractures [5 – 11]. There is evidence that
quickly, and relatively high incidence of side ef-
calcium is important not only for peak bone mass
fects have been observed [6]. Long-term adherence
development but also in reducing bone loss in
to hormone replacement therapy is considered to
postmenoapusal women. It has been believed that
be low compliance. Effective alternatives for pre-
Vitamin D and calcium (and possibly vitamin K)
vention of bone loss in recently postmenopausal
are vital to prevention of bone loss and fracture.
women include vitamin K and vitamin D. Al-
Matsunaga found a synergistic effect of vitamin D
though, single therapies with these are effective in
and K in reducing bone loss in ovariectomized
inhibiting bone loss, prevention of bone loss in
rats [10]. Furthermore, it was observed that effi-
postmenopausal women is more difficult than
cacy of vitamin K was stronger in high bone
hormone replacement therapy [7,20,21], and the
resorption and high plasma vitamin D level [12].
clinical results of combined therapy have not been
Thus, in conditions of high turnover in bone
metabolism such as early postmenopausal period,
In this communication, we present the results of
it is conceivable that the clinical effect of vitamin
our study of the clinical effects of combined use of
K may increase when the plasma vitamin D level
vitamin K and D on postmenopausal osteopenia
and osteoporosis, and of its effects on bone
metabolism and the coagulofibrinolysis system.
The causes of osteoporosis have not yet been
fully elucidated, but recently published reportssuggest a possible involvement of vitamin K defi-
2. Subjects and methods
ciency [13 – 15]. It has been suggested that g-car-boxyglutamic
We enrolled 172 women with a bone mineral
(osteocalcin, BGP), a bone matrix protein, plays a
density of the lumbar spine B0.98 g/cm2, as
key role in bone metabolism [16]. The glutamic
measured by dual-energy X-ray absorptiometry
acid residues of osteocalcin are g-carboxylated by
(DEXA, Lunar DPX-L), in the present random-
the enzyme carboxylase, and vitamin K is essen-
ized study. All subjects were attending the De-
T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
partment of Obstetrics and Gynecology at Osaka
istics of 126 patients at the start of the study. The
Medical College for outpatient consultations re-
profiles for age, postmenopausal duration, per-
lated to climacteric/menopausal conditions. We
randomly assigned them to one of the following
menopause, serum calcium, serum gonadotropin
four groups by month of birth (January – March,
and estradiol values, and physique did not differ
April – June, July – September, October – Decem-
significantly among the four groups. There were
ber) after sufficient informed consent: vitamin K
no significant differences on one-way factorial
analysis of variance (ANOVA) in basal levels of
Glakay 45 mg per day), vitamin D therapy group
bone mineral density among the four groups.
(43 subjects; 1-a hydroxycholecalciferol: Onealfa 1
The patients were not given specific instructions
mg per day), vitamin K and D combined therapy
regarding adequate dietary calcium intake and did
group (43 subjects), or a control group receiving
not take part in a program of exercise. However,
dietary therapy alone (43 subjects). This study
use of daily products including milk in meals was
started with 172 subjects, with 43 patients in each
instructed when questions about calcium intake
of the four groups, while 12, 26, 38 and 46
were asked. Patients in each group were treated
patients dropped out within 6, 12, 18 and 24
for 2 years, during which periodic measurements
of bone mineral density and evaluations of bone
dropout rate 26.7%). We enrolled 126 patients
metabolism markers and coagulofibrinolysis func-
who have finished this study of 24 months and
tion were performed. Vertebral bone mineral den-
analyzed their data. Table 1 shows the character-
sity was measured at baseline and after 6, 12, 18
Mean (S.D.) plasma hormone le6elsFSH (mIU/ml)
a Body mass index expressed as weight (kg)/height (m)2. b Percent fat was measured by DPH (Lunar Hadiation, Madison, WI, USA).
FSH and LH were greater than 30 and 15 IU/ml, respectively, in all women. Figures in parenthesis indicate 1 standard deviation. P-value assessed using ANOVA. No significant differences were found in any of the parameters among the groups. T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
and 24 months of therapy by dual energy X-ray
3. Results
absorptiometry (model DPX, Lunar RadiationCorp, Madison, WI, USA) which uses a constant
There were no significant differences on one-
potential X-ray source at 12.5 fJ and a K-edge
way factorial ANOVA in basal levels of bone
filter (cecium) to achieve a congruent beam of
mineral density among the four groups consisting
stable dual energy radiation. The effective energies
of the 172 patients who started the study (P =
were 6.4 and 11.2 fJ. Bone mineral density was
0.23) and the 126 patients who continued this
assessed for the L2-4 region and expressed as the
clinical study for 2 years (P = 0.057). However,
average areal density (BMD = g/cm2). We defined
there were significant differences in this parameter
osteopenia as a BMD value below 0.98 g/cm2 and
between the combined group and vitamin K2
osteoporosis as a BMD below 0.83 g/cm2. In this
(P = 0.0101) and vitamin D (P
study, we employed the criteria for diagnosis of
for the latter 126 patients on multiple comparison
osteopenia and osteoporosis using dual energy
by ANOVA. Since 26.7% of the patients dropped
X-ray absorptiometry which was proposed by the
out over 2 years, although the present study was
Japan Society of Bone Metabolism in 1996 [24].
begun with 172 subjects and dropouts include
The in vivo and in vitro coefficients of variation
patients with relatively high BMD in the com-
were 0.73 and 0.41%, respectively. The bone
bined therapy group, basal level of BMD was
metabolism markers analyzed were serum type 1
significantly lower than those in the vitamin K or
D alone therapy group in the evaluation includ-
serum intact osteocalcin, and urinary pyridinoline.
ing only those subjects who completed the 2-year
Serum type 1 collagen carboxyterminal propeptide
study. The following appear to be biased data
(P1CP) was measured by radioimmunoassay using
given the above considerations. In the vitamin K2
a kit from Orion Diagnostica (Espoo, Finland).
alone group, mean bone mineral density remained
Serum intact osteocalcin concentrations were mea-
lower than the baseline level (0.876 90.091 g/cm2)
sured by radioimmuassay using a kit from Ya-
up to 18 months after the start of treatment, but
masa Corp (Chiba, Japan). Urinary excretions of
was slightly higher (not significant) at 24 months
pyridinoline were measured by HPLC (Sumitomo
(0.888 90.112 g/cm2). In contrast in the vitamin
Metal Bioscience Lab.) according to the methods
K and D combined therapy group bone mineral
of Eyre et al. [25], and values were corrected using
density was 0.052 g/cm2 higher than the baseline
the urinary excretion of creatinine. To confirm
level (0.820 90.097 g/cm2) at 6 months (PB
effects of vitamin K, we monitored the time course
0.001, significant), and higher BMD levels were
of changes in urinary concentration of g-carboxyg-
sustained up to 24 months (Table 2). The time
lutamate (Gla)/Cr. The urinary concentration of
course of percentage changes in BMD in the 126
patients who continued this study for 24 months
(Sumitomo Metal Bioscience Lab) according to
is shown in Fig. 1. There were no significant
the methods of Kuwada and Katayama [26]and
differences from control for the subjects receiving
values were corrected using the urinary excretion
vitamin K alone therapy at 6 months (1.31 9
of creatinine. Tests of blood coagulation function
6.94%) or 12 months (0.736 96.09%), whereas the
consisted of measurement of activated partial
percentage change in BMD was significantly
thromboplastin time (APTT) and analysis of con-
higher than control at 18 months (0.278 96.55%,
centrations of antithrombin III (AT III), fibrino-
P B0.05) and 24 months (0.13595.44%, PB
gen, and plasminogen. These measurements were
0.05). On the other hand, the percentage increases
performed using standard laboratory methods.
Data were statistically analyzed by ANOVA or
therapy group were significantly higher (4.10 9
the Wilcoxon signed-rank test, and the level of
5.88% at 6 months; P B0.001, 5.8696.85% at 12
significance was set at P B0.05. Results are pre-
months; P B0.001, 5.0198.11% at 18 months;
sented as mean and standard deviation (mean 9
P B0.001, and 4.9297.89% at 24 months; PB
0.001) than those in the control group. Compared
T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
Table 2Vertebral bone mass before and during treatment
*PB0.05; **PB0.001, significance was determined using Wilcoxon’s signed-rank test, and P-values refer to differences in bone masslevels in the treated groups compared with their levels at the start of the study. Mean (S.D.) values are expressed as g/cm2.
Fig. 1. Percentage changes (mean 9S.D.) from baseline in bone mineral density in all four groups during the 24-month study. P-value assessed using Wilcoxon signed-rank test.
with the vitamin K or D alone therapy group,
P B0.001, vitamin K —combined therapy; PB
BMD was significantly increased in the combined
0.01). Furthermore, it was found that there were
therapy group from 6 to 24 months after the start
more responders to treat in the combined therapy
of treatment (vitamin D — combined therapy;
group than in the vitamin K and D alone group. T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
In the 24-month treatment, BMD increase of 5%
or higher was exhibited by 9.4 and 23.3% of the
which was used to confirm the absorption and
subjects in the vitamin K and D alone groups,
physiological activity of vitamin K , revealed that
respectively, but it was exhibited by 45.2% of the
the concentration increased significantly with
subjects in the combined therapy group (signifi-
treatment in both the vitamin K alone therapy
cantly higher than in the vitamin D alone group,
group (6 M; 53.0 938.2%, 18 M; 82.5956.3%, 24
P = 0.014). In the combined therapy group, more-
M; 56.8 938.8%, PB0.01) and the vitamin K2
over, 67.8% of responders had BMD increase of
and D combined therapy group (6 M; 43.9 9
2% or higher. Although non-responders with
43.6%, 12 M; 44.9 972.1%, 18 M; 49.9949.5%,
BMD decrease up to 22.6% were found, the per-
P B0.01). Serum intact osteocalcin and urinary
centage of such patients was significantly lower
pyridinoline levels tended to increase with dura-
than that in the vitamin D alone group (71.9%)
tion of treatment (12 and 18 months) in the
combined therapy group. Serum intact osteocalcin
There were no significant differences among
level increased significantly by 36.0 944.8% at 18
any of the groups in any of the background
months (P B0.05) in the combined therapy group.
parameters, bone parameters or coagulofibrinoly-
Urinary pyridinoline level was significantly in-
sis parameters (Table 4). Measurement of urinary
creased at 18 months (89.6 9112.3%, PB0.01)
Table 3Percentages of responders and non-responders to 24-months treatment
D3-Comb.: P = 0.014, others: n.s.
D3-Comb.: P = 0.025, others: n.s.
Table 4Baseline values of bone metabolism and coagulofibrinolysis parameters
pyridinoline/creatinine (pmol/MCM. Cr.)
Figures in parenthesis indicate 1 standard deviation. P-value assessed using ANOVA. No significant differences were found in anyof the parameters among the groups. P I CP, type I procollagen C-terminal propeptide; APTT, active partial thromboplastin time. T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
Fig. 2. Percentage changes from baseline in bone metabolism markers in all four groups during the 24-month study. Values areexpressed as mean 9S.E.M. P-value assessed using Wilcoxon signed-rank test. *: PB0.05, **: PB0.01 compared with the baseline.
and 24 months (53.4 955.7%, PB0.05) in the
change and changes in serum P1CP levels at 12
vitamin K alone therapy group. In the combined
months in the vitamin K treatment group (P =
therapy group, urinary pyridinoline level was sig-
0.0012). A significant positive correlations were
nificantly increased at 6 (17.5 936.4%, PB0.05),
also observed between BMD change and changes
12 (27.5 918.7%, PB0.05), 18 months (29.49
in serum P1CP level (P = 0.034) and intact os-
31.7%, P B0.05) and 24 months (84.5951.9%,
teocalcin level (P = 0.035) after 12 months of
combined therapy. At 24 months of combined
Serum P1CP was approximately 20% higher at
therapy, we also observed a positive correlation
6 months (19.8 927.5%, PB0.05) and 12 months
between BMD change and intact osteocalcin level
(18.7 937.2%, PB0.05) in the vitamin K alone
(P = 0.002). On the other hand, we observed a
therapy group and returned to baseline levels at
significant negative correlation between BMD
24 months. In contrast, in the combined therapy
change and change in urine pyridinolin level at 12
group baseline levels were more or less main-
(P = 0.001) and 24 months (0.004) of combined
tained up to 12 months, but increases of 21.8
( 922.5)% and 24.2 (923.1)% were then recorded
Tests of coagulation function revealed a grad-
at 18 months (P B0.05) and 24 months (PB
ual decline in APTT in both the vitamin K alone
0.01), respectively (Fig. 2). Table 5 shows the
group and combined therapy with vitamin D3
group, which fell significantly to 15.0 98.4 and
metabolic marker changes during treatment with
14.2 911.5% below baseline at 6 months (PB
vitamin K or combined therapy. There was a
0.01) and 18 months (P B0.05), respectively, in
significant positive correlation between BMD
T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
cantly to 19.1 910.4 and 15.299.5% below base-
4. Discussion
line at 18 months (P B0.01) and 24 months (PB0.05) in the combined therapy with vitamin D
Vitamin K occurs naturally in two forms, K
group. Serum AT III activity gradually increased
and K . The K congener, menaquinone-4, which
over time, and increased significantly to 8.2 96.4
has the most potent g-carboxylation activity, re-
and 8.3 97.5% above baseline at 18 months (PB
portedly improves bone mass in patients with
0.05) and 24 months (P B0.05), respectively, in
involutional osteoporosis [17]. In the present
the vitamin K alone therapy, and increased sig-
study, we attempted to determine whether combi-
nificantly to 11.1 97.4 and 15.297.5% above
nation therapy with vitamin K and D yields a
baseline at 18 months (P B0.01) and 24 months
synergistic effect in maintaining or increasing
(P B0.01), in the combined therapy with vitamin
bone mineral density due to promotion of calcifi-
D group. Serum fibrinogen and plasminogen lev-
cation in postmenopausal women with decreased
els also tended to increase gradually over time.
bone mass. Treatment with menaquinone-4 alone
Significant increases in serum fibrinogen levels
for 24 months produced an increase of 0.135 95.44% in BMD, confirming a maintenance effect
were observed at 6 months (26.0 941.5%, PB
on BMD. For combination therapy consisting of
0.05) from baseline in the vitamin K alone ther-
vitamin K and D , however, marked increases in
BMD of 5.86 96.85 and 4.9297.89% were ob-
(28.1 935.5%, PB0.05) and 24 months (30.29
served at 12 and 24 months, respectively. Com-
33.5%, P B0.05) from baseline in the combined
bined therapy appears to have an effect on
therapy group. Significant increases in serum plas-
vertebral BMD in the first 6 – 12 months, while
minogen levels were observed at 18 months
thereafter mean rate of increase in BMD decline.
(14.2 912.2%, PB0.05 and 11.998.5%, PB
The rate of increase appeared to decrease slightly
0.01) and 24 months (19.6 912.6%, PB0.01 and
because the bone metabolic profile was almost
19.2 913.5%, PB0.05) from baseline in both the
stabilized by sufficient supplementation of vitamin
vitamin K alone therapy group and combined
effects of physiological aging. However, since the
Table 5Correlations between percent changes in vertebral BMD and bone markers
Vitamin K alone 12 months therapyVitamin K alone 24 months therapyCombined therapy with 6itamin K and D 12 monthsCombined therapy with 6itamin K and D 24 monthsT. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
Fig. 3. Percentage changes from baseline in coagulation function in all four groups during the 24-month study. Values are expressedas mean 9S.E.M. P-value assessed using Wilcoxon signed-rank test. *: PB0.05, **: PB0.01 compared with the baseline.
rate of decrease was smaller than the 1.9% per
osteoporosis, there is negative imbalance between
year exhibited by the control group, it appeared
bone resorption and bone formation, resulting in
that decrease in BMD could be suppressed by
bone loss. We observed significant BMD change
combined therapy with vitamin K and D for a
at 6 months of combined therapy, while mean
period from several years to more than 10 years
levels of bone formation markers did not increase
after menopause, leading to prevention of bone
and bone resorption marker increased signifi-
fracture. Koshihara and colleagues described a
cantly. Although clear explanation of this contra-
synergistic effect in an in vitro system containing
diction is difficult, there appeared to be more
cultured osteoblasts, in which this process of cal-
cases in which osteogenesis became dominant in
cification was greatly promoted by the presence of
the balance of formation and resorption in bone
metabolism, since there were many responders in
vitamin K suppressed decrease in spinal BMD,
the combined therapy group. Moreover, the mean
compared with vitamin D treatment [28]. In an-
values of bone resorption markers did not de-
other recent study, vitamin K partially prevented
crease compared with the previous value due to
bone loss caused by estrogen deficiency, when
menopausal period, but the change in such mark-
There was a tendency toward higher concentra-
ers was sufficient to suppress bone resorption. The
tions of intact osteocalcin at times up to 18
significant positive correlation between individual
months of treatment in the groups receiving vita-
BMD change and serum P1CP level in the 24-
min K alone and combined therapy, reflecting
month vitamin K alone therapy and the signifi-
the fact that bone turnover had increased. In
cant positive correlation between individual BMD
T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
change and serum P1CP level and intact osteocal-
raishi for her skillful assistance, and are grateful
cin level in the group with combined therapy with
to Eizai Pharmaceutical Co Ltd for financial
vitamin D suggested that vitamin K can acceler-
ate bone formation, and that this formation canbe potentiated by combination with vitamin D .
In recent in vitro studies, menaquinone-4 modu-lated proliferation and function of mouse cultured
References
In the coagulation system, plasma concentra-
[1] Kanis JA. Risk factors in osteoporosis. Maturitas
tions of the vitamin K-dependent and contact
[2] Ushiroyama T, Okamura S, Ikeda A, Ueki M. Efficacy of
factors have important effects. Coagulation dis-
ipriflavone and 1a vitamin D therapy for the cessation of
vertebral bone loss. Int J Gynecol Obstet 1995;48:283 – 8.
metabolism, defective synthesis of coagulation
[3] Netelenbos C. Osteoporosis: intervention options. Matu-
factors and regulatory proteins, impaired clear-
ance of activated coagulation factors and in-
[4] Watts NB, Becker P. Alendronate increases spine and hip
bone mineral density in women with postmenopausal
creased fibrinolysis [31,32]. It has been shown that
osteoporosis who failed to respond to intermittent cyclical
vitamin K (menaquinone-4) improves fibrinoly-
sis. Coagulation function was evidently promoted
[5] Rozenberg S, Vandromme J, Ayata NB, Filippidis M,
by continuous, long-term administration given the
Kroll M. Osteoporosis management. Int J Fertil Womens
observation of increased concentrations of AT III
[6] Watts NB. Postmenipausal osteoporosis. Obstet Gynecol
and fibrinogen. However, these changes, which
occurred in response to the promotion of coagula-
[7] Celotti F, Bignamini A. Dietary calcium and mineral/vita-
tion function, remained within the normal range,
min supplementation: a controversial problem. J Int Med
whereas plasminogen values tended to increase
gradually. Thus, promotion of fibrinolytic func-
[8] New SA. Bone health: the role of micronutrients. Br Med
tion was also observed, suggesting that coagulofi-
[9] Meunier PJ. Calcium, vitamin D and vitamin K in the
brinolytic balance may have been maintained in
prevention of fractures due to osteoporosis. Osteoporosis
the physiological fibrinolytic system. Ronden et
al. reported that very high doses of vitamin K
[10] Matsunaga S, Ito H, Sakou T. The effect of vitamin K
affected neither blood coagulation characteristics
and D supplementation on ovariectomy-induced boneloss. Calcif Tissue Int 1999;65:285 – 9.
nor the blood platelet aggregation rate [33].
[11] Shearer MJ. The roles of vitamins D and K in bone
In conclusion, the results of this in vivo study
health and osteoporosis prevention. Proc Nutr Soc
involving patients with postmenopausal decreased
bone mass suggest that combined therapy with
[12] Orimo H, Fujita T, Onomura T, Inoue T, Kushida K,
vitamin K and D increases bone turnover and
Shiraki M. Clinical evaluation of Ea-0167 (Menate-
trenone) in the treatment of osteoporosis. Clin Eval (In
promotes bone formation and calcification, result-
ing in marked increases in bone mineral density
[13] Sato Y, Honda Y, Kuno H, Oizumi K. Menatetrenone
and improvement in bone quality. Given that the
ameliorates osteopenia in disuse-affected limbs of vitamin
increases in coagulation function observed were
D- and K-deficient stroke patients. Bone 1998;23:291 – 6.
variations within the physiological range, and no
[14] Feskanich D, Weber P, Willett WC, Rockett H, Booth
SL, Colditz GA. Vitamin K intake and hip fractures in
adverse drug reactions were observed, this mode
women: a prospective study. Am J Clin Nutr 1999;69:74 –
of combined therapy may be very effective in
preventing postmenopausal bone fracture.
[15] Sato Y, Tsuru T, Oizumi K, Kaji M. Vitamin K defi-
ciency and osteopenia in disuse-affected limbs of vitaminD-deficient elderly stroke patients. Am J Physiol MedRehabil 1999;78:317 – 22. Acknowledgements
[16] Lian JB, Gundberg CM. Osteocalcin — biochemical con-
siderations and clinical applications. Chin Orthopaed
The authors would like to thank Kyoko Shi-
T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
[17] Orishige H. Clinical evaluation of menaquinone versus
changes in the content of mature hydroxypyridinium
alfacalcidol in the treatment of osteoporosis: a double-
residues. Biochem J 1988;252:495 – 500.
blind, controlled Phase III clinical trial. Clin Eval
[26] Kuwada M, Katayama K. A high-performance liquid
chromatographic method for the simultaneous determina-
[18] Akiyama Y. Research on the mechanism of inhibitory
tion of g-carboxyglutamic acid and glutamic acid in
action of vitamin K on bone resorption in cultured organ
proteins, bone, and urine. Anal Biochem 1981;117:259 –
culture. J Jpn Soc Bone Min Metab 1991;9:239.
[19] Koshihara Y. Establishment of human osteoblastic cells
[27] Koshihara Y. Current topics in vitamin K research: pro-
derived from periosteum in culture. In Vitro Cell Dev
motion of bone formation. Vitamin 1998;72:641 – 4.
[28] Iwamoto I, Kosha S, Noguchi S, Murakami M, Fujino T,
[20] Anderson JJ, Rondano P, Holmes A. Roles of diet and
Douchi T, Nagata Y. A longitudinal study of the effect of
physical activity in the prevention of osteoporosis. Scand
vitamin K on bone mineral density in postmenopausal
J Rheumatol Suppl 1996;103:65 – 74.
women: a comparative study with vitamin D and estro-
[21] Feskanich D, Weber P, Willett WC, Rockett H, Booth
gen – progestin therapy. Maturitas 1999;31:161 – 4.
SL, Colditz GA. Vitamin K intake and hip fractures in
[29] Somekawa Y, Chigugi M, Harada M, Ishibashi T. Use of
women: a prospective study. Am J Clin Nutr 1999;69:74 –
vitamin K (menatetrenone) and 1,25-dihydroxyvitamin
D in the prevention of bone loss induced by leuprolide.
[22] Kamezawa K. Inhibitory effects of combined treatment
J Clin Endocrinol Metab 1999;84:2700 – 4.
with vitamin K and D on bone loss of ovariectomized
[30] Akedo Y, Hosoi T, Inoue S. Vitamin K
rats: a microradiographic study. Fukuoka Igaku Zasshi
proliferation and function of osteoblastic cells in vitro.
[23] Douglas AS, Robins SP, Hutchinson JD, Porter RW,
Biochem Biophys Res Commun 1992;187:814 – 20.
Stewart A, Reid DM. Carboxylation of osteocalcin in
[31] Mehta AB, Mclntyre N. Haematological disorders in liver
postmenopausal osteoporotic women following vitamin K
disease. Forum Genova 1998;8:8 – 25.
and D supplementation. Bone 1995;17:15 – 20.
[32] Andrew M. The relevance of developmental hemostasis to
[24] Orimo H, Sugioka Y, Fukunaga M, Muto Y, Hokoke-
hemorrhagic disorders of newborns. Semin Perinatol
buchi T, Gorai I, Nakamura T, Kushida K, Tanaka H,
Ikai T, Oh-hashi Y. Diagnostic criteria of primary os-
[33] Ronden JE, Groenen van Dooren MM, Hornstra G,
teoporosis. J Bone Miner Metab 1998;16:139 – 50.
Vermeer C. Modulation of arterial thrombosis tendency
[25] Eyre DR, Dickson IR, Van Ness KP. Collagen cross-link-
in rats by vitamin K and its side chains. Atherosclerosis
ing in human bone and articular cartilage. Age-related
CONTENTS Vehicle ScrutinyEnclosuresDeclarationEntry Form "6TH KAVIGURU RALLY" Kolkata Ð Santiniketan May 31, 2003 Supplementary Regulations & Rules, Official Programme and Entry Form The “Sixth Kaviguru Rally ” is being organised by the Bengal Motor Sports Club (Promoter) and held under the International SportingCodes of the Federation International
The HAVACS (HIV Atlanta VA Cohort Study) was initiated in 1982 to clinically care for and study all HIV+ veterans seeking care at the Atlanta VA Medical Center. To date, over 3,000 patients have been entered into this cohort and database. The prospective collection of data was begun in 1982 and includes the full HIV history of patients including any care they received for their HIV disease b
 Effect of continuous combined therapy with vitamin K and
vitamin D on bone mineral density and coagulofibrinolysis
Takahisa Ushiroyama *, Atushi Ikeda, Minoru Ueki
Department of Obstetrics and Gynecology, Osaka Medical College, 2-7 Daigaku-machi, Takatsuki, Osaka 569-8686, Japan
Received 28 July 2000; received in revised form 7 February 2001; accepted 14 September 2001
Abstract
Effect of continuous combined therapy with vitamin K and
vitamin D on bone mineral density and coagulofibrinolysis
Takahisa Ushiroyama *, Atushi Ikeda, Minoru Ueki
Department of Obstetrics and Gynecology, Osaka Medical College, 2-7 Daigaku-machi, Takatsuki, Osaka 569-8686, Japan
Received 28 July 2000; received in revised form 7 February 2001; accepted 14 September 2001
Abstract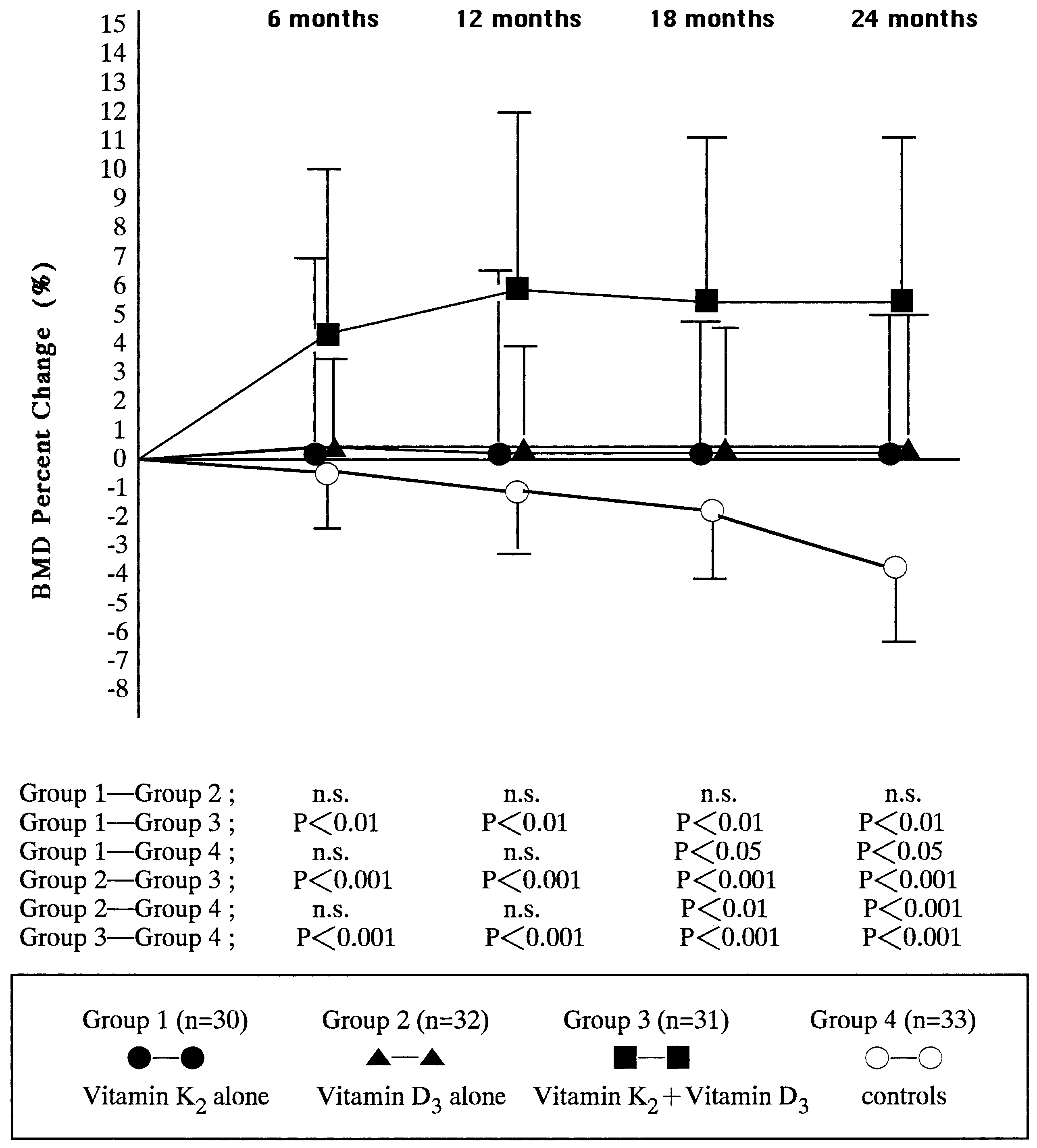 T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
Table 2Vertebral bone mass before and during treatment
*PB0.05; **PB0.001, significance was determined using Wilcoxon’s signed-rank test, and P-values refer to differences in bone masslevels in the treated groups compared with their levels at the start of the study. Mean (S.D.) values are expressed as g/cm2.
T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
Table 2Vertebral bone mass before and during treatment
*PB0.05; **PB0.001, significance was determined using Wilcoxon’s signed-rank test, and P-values refer to differences in bone masslevels in the treated groups compared with their levels at the start of the study. Mean (S.D.) values are expressed as g/cm2.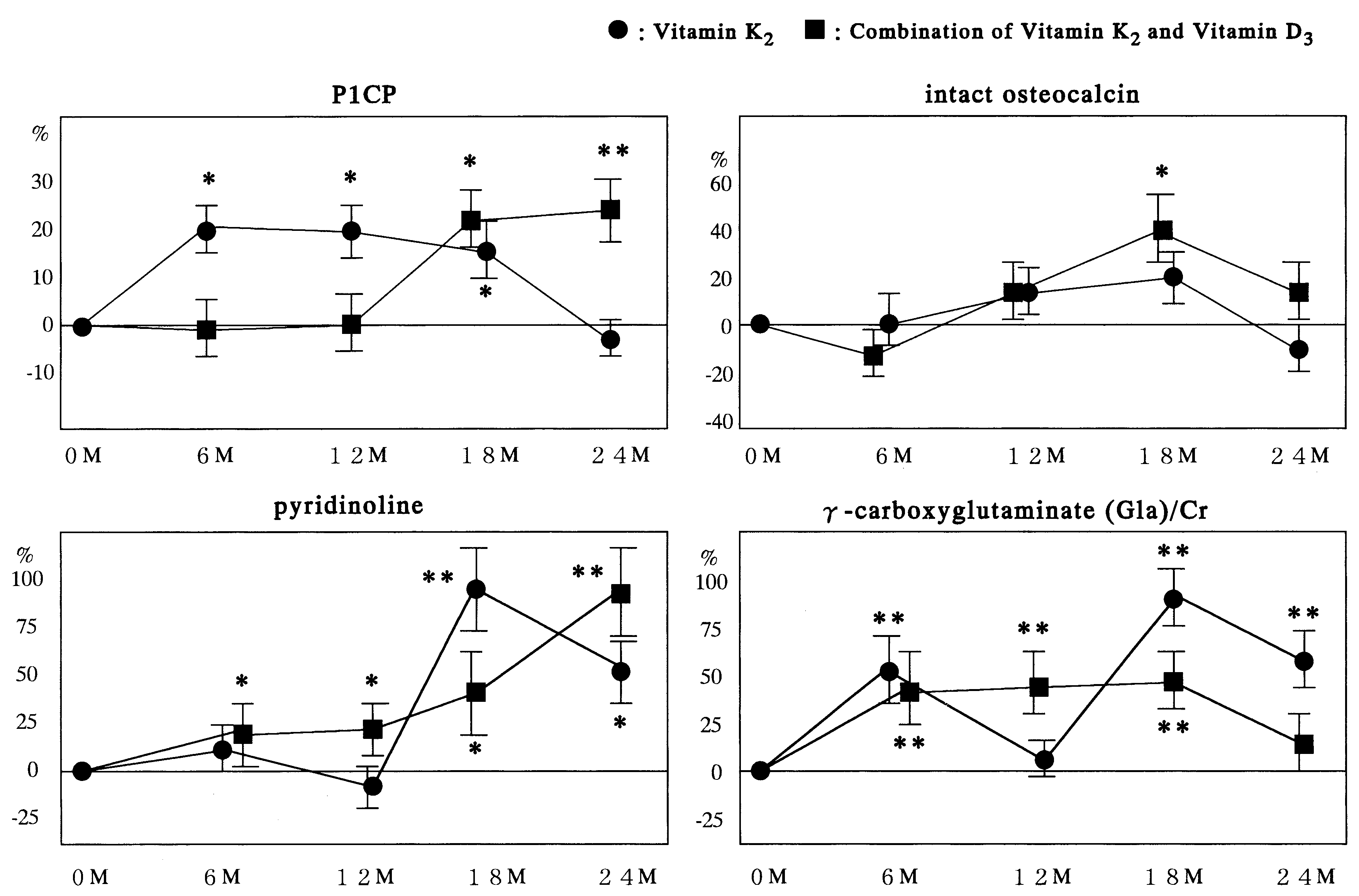 T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
Fig. 2. Percentage changes from baseline in bone metabolism markers in all four groups during the 24-month study. Values areexpressed as mean 9S.E.M. P-value assessed using Wilcoxon signed-rank test. *: PB0.05, **: PB0.01 compared with the baseline.
T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
Fig. 2. Percentage changes from baseline in bone metabolism markers in all four groups during the 24-month study. Values areexpressed as mean 9S.E.M. P-value assessed using Wilcoxon signed-rank test. *: PB0.05, **: PB0.01 compared with the baseline.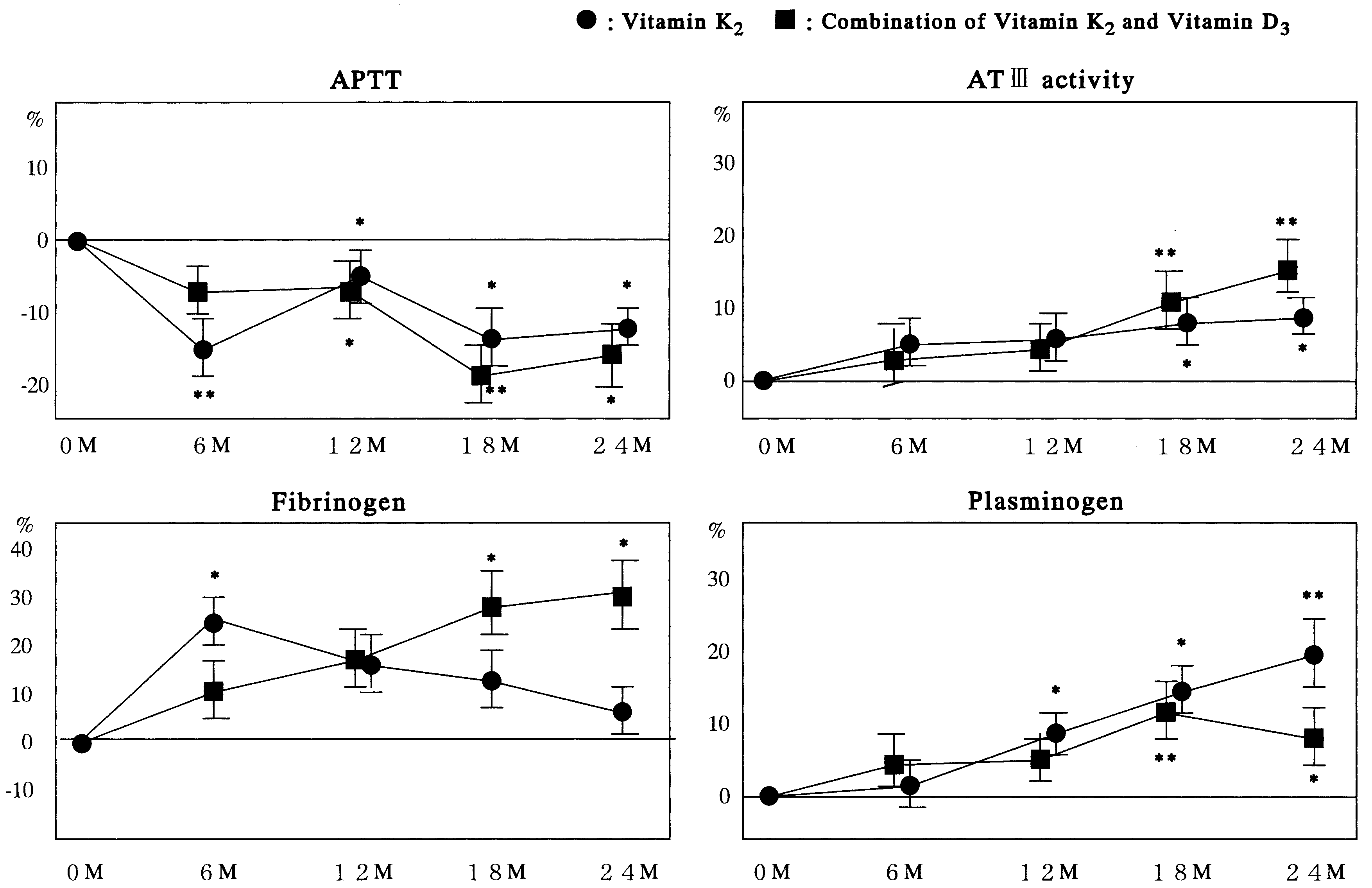 T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
Fig. 3. Percentage changes from baseline in coagulation function in all four groups during the 24-month study. Values are expressedas mean 9S.E.M. P-value assessed using Wilcoxon signed-rank test. *: PB0.05, **: PB0.01 compared with the baseline.
T. Ushiroyama et al. / Maturitas 41 (2002) 211 – 221
Fig. 3. Percentage changes from baseline in coagulation function in all four groups during the 24-month study. Values are expressedas mean 9S.E.M. P-value assessed using Wilcoxon signed-rank test. *: PB0.05, **: PB0.01 compared with the baseline.