Pilot study on the effect of reducing dietary fodmap intake on bowel function in patients without a colon
Pilot Study on the Effect of Reducing Dietary FODMAPIntake on Bowel Function in Patients without a Colon
Catherine Croagh, MB, BS, Susan J. Shepherd, BApplSci, Melissa Berryman, BApplSci, Jane G. Muir, PhD, andPeter R. Gibson, MD
ileorectal anastomosis, diet, short-chain carbohydrates, pouch function
Background: Poorly absorbed short-chain carbohydrates (FOD- MAPs) in the diet should, by virtue of their osmotic effects, increase fecal output following colectomy and ileal pouch formation or ileorectal anastomosis (IRA). The aim was to perform a proof-of-
Ileal pouch-anal anastomosis (IPAA) surgery is curative
surgical treatment for ulcerative colitis (UC) that is medi-
concept evaluation of this hypothesis.
cally refractory or complicated by dysplasia. Colectomy with
Methods: Fifteen patients (13 pouch, 2 IRA) had dietary and
ileorectal anastomosis is also used for the treatment of in-
symptomatic evaluation before and during a low FODMAP diet.
flammatory bowel disease and familial adenomatous polyp-
Carbohydrate malabsorption was evaluated by breath tests. Pouchitis
osis. IPAA significantly improves quality of life in patients
was assessed clinically/endoscopically or by fecal lactoferrin.
with UC who require surgery.1 However, the clinical out-
Results:
come is not ideal. Even though the ileal pouch acts as a
Of 8 patients with a breath hydrogen response to lactu-
lose, 7 had fructose malabsorption, 3 with lactose malabsorption,
reservoir and continence is usually maintained, the average
and 1 had lactose malabsorption alone. Five of 7 studied retrospec-
number of stools per day is 6 – 8 and usually with overnight
tively improved stool frequency (from median 8 to 4 per day; P
stool production, and the consistency of those stools is rarely
ϭ 0.02), this being sustained over 0.5–3 years of follow-up. Five of
solid.2 A problematic functional result might be due to in-
8 patients completed a prospective arm of the study. One patient had
flammation of the pouch (pouchitis), the retained rectal cuff
sustained improvement in stool frequency and 1 had reduced wind
(cuffitis), or ileum proximal to the pouch (pre-pouch ileitis),3
production. Overall, none of 8 patients who had pouchitis improved.
but irritable pouch syndrome may also occur, being a syn-
In contrast, median daily stool frequency fell from 8 to 4 (P
drome of increased frequency of bowel movement with
ϭ 0.001) in the 7 without pouchitis. The degree of change in
change in stool consistency, abdominal pain or cramping, and
FODMAP intake also predicted response. There was a tendency for
perianal or pelvic discomfort in the absence of endoscopic
pouchitis to be associated with low baseline FODMAP intake.
and histologic inflammation.4 Similar frequent bowel actions
Conclusions: There is a high prevalence of carbohydrate malab-
and unformed consistency is also associated with ileorectal
sorption in these patients. Reduction of the intake of FODMAPs
may be efficacious in reducing stool frequency in patients without
Management of functional problems with pouches has
pouchitis, depending on dietary adherence and baseline diet.
ranged from antibiotic therapy for pouchitis to hypomotility
(Inflamm Bowel Dis 2007;13:1522–1528)
agents such as loperamide, to pouch excision in extremesituations.3 Dietary intervention has figured little in manage-
Key Words: inflammatory bowel disease, colectomy, ileal pouch,
ment recommendations, except that fiber supplementation isoften recommended. However, the evidence base for this isabsent, with only 1 crossover study that showed methylcel-
Received May 20, 2007; accepted July 14, 2007.
lulose and pectin to be ineffective.5 Supplementation with
From the Department of Gastroenterology and Monash University Depart-
inulin at a relatively high dose improved mucosal inflamma-
ment of Medicine, Box Hill Hospital, Victoria, Australia.
Supported by grants from the International Organisation for Inflammatory
tion in patients with pouchitis without altering symptoms,6
Bowel Disease, the Vera & Les Erdi Foundation, and the CASS Foundation.
but its effect in those without inflammation has not been
Lactoferrin kits were donated by TechLabs Inc. S.J.S. was supported by a
Dora Lush Scholarship from the National Health & Medical Research
One factor that will influence the functional properties
Reprints: Prof. Peter Gibson, Department of Medicine, Box Hill Hospital,
of a pouch or rectum is the volume of liquid entering it from
Box Hill, Victoria 3128, Australia (e-mail: Peter.Gibson@med.monash.
the small bowel. This is well documented for the normal large
bowel, where diarrhea will result if the volume entering it
Copyright 2007 Crohn’s & Colitis Foundation of America, Inc.
from the small intestine overwhelms the desiccating ability of
the large bowel mucosa. An ileal pouch or rectum will have
Published online 7 September 2007 in Wiley InterScience (www.
markedly reduced desiccating ability than an intact large
Inflamm Bowel Dis ● Volume 13, Number 12, December 2007
Inflamm Bowel Dis ● Volume 13, Number 12, December 2007
bowel. Hence, it might be anticipated that the pouch/rectum
For the prospective study, patients gave written, in-
will be less able to cope with changes in small intestinal
formed consent. A medical history was taken and general
output, with such increases being readily expressed as looser
physical examination performed. A full dietary assessment
and more frequent bowel actions. Two factors that potentially
was made by an accredited practicing dietitian and a prospec-
influence small intestinal output are the small intestinal tran-
tive 7-day food diary using standard measures was performed
sit7 and the number of osmotically active molecules in the
by the patient during the screening period. The patients also
small intestinal lumen, a factor utilized by osmotic laxatives.
filled out a daily symptom diary and continued this through-
We have hypothesized that the osmotic load on the
out the study. Fecal samples were obtained prior to com-
pouch is significantly influenced by the amount of poorly
mencing the diet. Breath hydrogen tests (see below) were also
absorbed short-chain carbohydrates in the diet. Such carbo-
performed during the screening period. The patients were
hydrates have been collectively termed FODMAPs (Ferment-
then educated on the low FODMAP diet (see below) and
able Oligo-, Di-, and Mono-saccharides And Polyols) and
asked to strictly follow that diet for the next 6 weeks. The
include free fructose and lactose (if fructose and/or lactose
patient was telephoned after 3 weeks by both the dietitian and
malabsorption is/are present), fructans (oligosaccharides of
a clinician. The patient was examined and diary cards perused
fructose) that are not hydrolyzed in the small intestine, and
at the last visit. The patient was again contacted by telephone
polyols such as sorbitol, which are absorbed to a very limited
extent only.8,9 Malabsorption of fructose and other FOD-MAPs has been linked to symptoms of irritable bowel syn-
Breath Hydrogen Testing
drome including diarrhea, gas, and abdominal discomfort.9,10
Following dietary restriction of fermentable substrates for at
In addition, a moderate to high fructose/sorbitol load hastens
least 24 hours and an overnight fast, patients underwent
small intestinal transit.11 Thus, the present study aimed to
breath hydrogen tests with the ingestion of 15 g lactulose (as
explore the concept that a change in dietary FODMAPs will
positive control), 35 g fructose in 200 mL water, and 50 g
influence the frequency and quality of stool output from an
lactose in 200 mL water on separate days. Breath hydrogen
ileal pouch or a rectum following an IRA.
was measured every 15 minutes using a hand-held breathhydrogen monitor (Bedfont Gastrolyzer, Air-Met Scientific,
MATERIALS AND METHODS
Nunawading, Victoria, Australia, or SC Microlyzer, Quintron
Patients
Instrument, Milwaukee, WI). A positive test was defined as a
Two cohorts of patients were studied. The first comprised 7
rise of 10 ppm in breath hydrogen above the baseline.
patients referred for the management of a dysfunctionalpouch or poor results following colectomy and IRA. The
Evaluation of the Baseline Diet
results from investigation and dietary intervention were au-
All patients in the retrospective group had an assessment of
FODMAP intake on a qualitative basis via a dietary history
The second group was studied prospectively using a
taken by a dietitian. For the prospective study, baseline diet
defined protocol before and during dietary intervention.
was analyzed semiquantitatively using tables of known FOD-
These patients were self-referred in response to advertising
MAP content.10 The intake was described as average prob-
through the newsletter and website of the Australian Crohn’s
lematic serves per day; 1 serve represented a portion of food
and Colitis Association (ACCA). Twenty-three patients re-
that contained Ͼ0.5 g free fructose or fructans,9 Ͼ4 g lactose,
sponded to advertising. Ten were excluded since they resided
and any sorbitol. An assessment was also made of the total
interstate or overseas and 5 were not interested in participat-
fructose load (comprising the sum of free fructose, equimolar
ing. Eight, all of whom had an ileal pouch performed follow-
fructose-glucose, and sucrose intake) and was expressed as
ing colectomy for UC, were studied. The protocol for the
the average number of sittings per day that the load exceeded
prospective arm of the study was approved by the Research &
3 g.10 All evaluations were performed without knowledge of
the response to dietary intervention. Protocol Dietary Intervention
For the retrospective cohort, patients’ notes were reviewed
The low FODMAP diet was instructed via a 1-hour, one-on-
with regard to medical history, demographic data, and symp-
one session with an Accredited Practicing Dietitian (M.B. or
tomatology prior to dietary education. The dietitian’s assess-
S.J.S.). The diet aimed to reduce free fructose and fructan
ment of dietary FODMAP intake was noted, as was their
ingestion as previously outlined in detail.9 If the fructose
subsequent adherence to the dietary regimen, for which they
breath hydrogen test showed complete fructose absorption,
were educated in a single one-on-one session of Ϸ1 hour.
total fructose ingestion was limited at any 1 meal, but foods
Changes in symptoms and other clinical indices were noted
containing free fructose were permitted in moderation. If the
lactose breath hydrogen test was negative, then no dietary
Inflamm Bowel Dis ● Volume 13, Number 12, December 2007
restriction of lactose was advised. Patients who failed to
alone, 1 had lactose malabsorption alone, and 3 had both
produce hydrogen in response to lactulose were considered to
malabsorb free fructose and lactose in the construction oftheir diet. Normal dietary habits were taken into account in
Analysis of Usual Dietary Intake of FODMAPs
the design of the dietary approach. Reinforcement of the diet
In the retrospective group, 2 patients (R4 and R5) were noted
and issues that arose with its use were managed at a telephone
to consume foods with a very high FODMAP content, par-
call made 3 weeks after commencing the diet. Assessment of
ticularly of fructose, lactose, and sorbitol. One patient (R3)
adherence to the diet was made on the basis of cross-check
had a low intake of FODMAPs, although did regularly con-
sume sources of fructose with equimolar concentrations ofglucose, equating to a high fructose load. The other patients
Fecal Lactoferrin
had an intake of FODMAPs that was neither high nor low.
In the prospective group, feces were evaluated for lactoferrin
Eight patients in the prospective arm completed a 7-day
content by enzyme-linked immunosorbent assay (ELISA)
food diary and a summary of their intake of FODMAPs is
using a commercially available kit (TechLab, Blacksburg,
shown in Table 2. Overall, the patients ate few foods con-
VA). This was performed outside the protocol for the study,
taining free fructose (such as apples, pears, honey, coconut
but was approved by the Eastern Health Research & Ethics
milk/cream). The major contribution to FODMAP intake
Committee. The assay was performed according to the man-
came from fructans, mainly as wheat-containing breakfast
ufacturer’s instructions. Lactoferrin has been previously
cereals, breads, pasta, and onions. Most also avoided milk or
shown to be a good marker of inflammation associated with
used lactose-free or soy milk, but ate cheese.
the pouch (pouchitis, cuffitis, and pre-pouch ileitis).12
Adherence to the Diet Data Evaluation
All patients in the retrospective group had good apparent
Data were expressed using descriptive statistics. Changes in
understanding of the diet, but adherence, as assessed by
indices were evaluated by paired or unpaired t-tests. Propor-
dietary history, was questioned in 2. Patient R2 had only
tions were compared using a Fisher’s exact test. A P-value of
partial adherence to the diet. Patient R3 had a low FODMAP
0.05 or less was considered statistically significant.
intake prior to dietary change and changed her diet mini-mally.
In the prospective group, 5 of the 8 patients completed
6 weeks on the diet together with week-6 food diaries (Table
Patient Characteristics
2). In 3 there was excellent adherence to the diet and 1 patient
The characteristics of the 7 patients in the retrospectively
(P2) markedly reduced FODMAP intake, although did con-
studied group are shown in Table 1. Five had an ileal pouch
sume some free fructose. One patient (P5) inadvertently con-
performed because of UC at a median of 6 (range 5–17) years
sumed foods high in FODMAPs, such as onion in tinned
previously, while an ileorectal anastomosis was formed in 2
soups and sauces and wheat-containing foods at a celebratory
after colectomy for chronic constipation (2 years previously)
and Crohn’s disease (20 years previously). All had problem-
Three patients did not complete the diet. One (P8) was
atic increased frequency of and/or nocturnal bowel actions.
lost to follow-up before receiving dietary instruction, 1 (P6)
Two were associated with chronic pouchitis, both of whom
abandoned the diet on development of acute chronic pouchitis
responded to antibiotic therapy (metronidazole or ciprofloxa-
shortly after commencing the diet, and the third (P7) reported
cin) either previously or subsequent to the study. The other 3
practical difficulty adhering to the changes required by the
patients with an ileal pouch had no evidence of pouchitis on
diet and abandoned it within 1 week.
clinical grounds or on recent endoscopic examination.
All patients in the prospectively studied group had
J-pouch surgery for UC with formation of the pouch a median
Effect of Diet on Symptoms
of 7 (range 3–10) years previously. In the majority, no sig-
Retrospective Study
nificant comorbidities were present, but 5 patients had been
Five of the 7 patients had substantial improvement in stool
treated for pouchitis on 1 or more occasions in the past,
frequency and consistency as shown by patient self-reporting.
including 1 who had chronic pouchitis.
The median number of stools per day fell from 8 to 4 (Pϭ 0.02; paired t-test). Benefits were sustained over longer-
Prevalence of Fructose and Lactose Malabsorption
term follow-up of 2 (0.5–3) years. Furthermore, patients
As shown in Table 1, 7 of the 15 patients had no breath
uniformly reported that reintroduction of prohibited foods
hydrogen response to lactulose (“nonhydrogen-producers”).
worsened their symptoms. The results of breath testing, while
Of the other 8, 4 had evidence of fructose malabsorption
influencing the nature of the dietary intervention, did not
Inflamm Bowel Dis ● Volume 13, Number 12, December 2007
Inflamm Bowel Dis ● Volume 13, Number 12, December 2007
TABLE 2. Quantification of FODMAP Intake According to Prospectively Completed 7-Day Food Diaries
Before Dietary Intervention (Numbers of Serves per Day)
During Dietary Intervention (Numbers of Serves per Day)
Noncompliant with or did not commence diet
Results are shown as averaged daily intake of problematic serves. The serve sizes are free fructose 0.5 g, fructans 0.5 g, lactose Ͼ4 g, sorbitol any, and totalfructose load (free fructose plus sucrose) Ͼ3 g.
appear to influence the response to the diet. Both patients who
At follow-up by telephone call 6 weeks after cessation
had no response to dietary change had chronic pouchitis,
of the study treatment period, the 2 patients who reported
benefit had continued dietary change. Patient P2 adhered tothe diet most of the time and had continued improvement in
Prospective Study
stool output and consistency. Patient P4 continued with par-
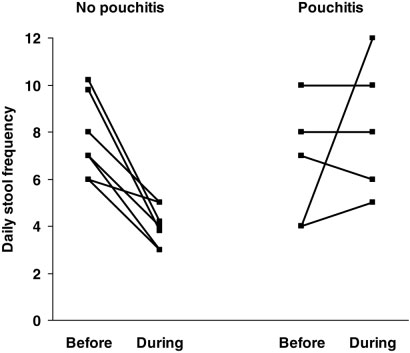
Only 5 patients were evaluable for the effect of diet on stool
tial adherence to the diet via the avoidance of apples, pears,
frequency (Fig. 1), with no change seen (median 6 to 5 per
and apricots, as well as lactose-containing foods. The im-
day; P ϭ ns). One patient had considerable worsening of
provement was not in stool frequency but wind production
stool frequency and this proved to be due to acute pouchitis.
had reduced. One of the patients (P1) who initially did not
As outlined in Table 1, the 3 patients who symptomatically
improve had incorporated some aspects of the dietary advice
did not improve had inflammation associated with the pouch
into his eating habits, such as avoiding free fructose con-
on fecal lactoferrin and clinical criteria, while the 2 who
tained in honey and apples, presumably related to symptom-
atic benefit. Two unresponsive patients (P3 and P5) did notcontinue the diet. Patient P6 who withdrew due to poorlycontrolled chronic pouchitis responded to ciprofloxacin ther-apy, and subsequent reintroduction of the diet led to signifi-cant improvement in symptoms, especially stool consistency. Predictors of Response Examining the 2 cohorts together, the presence or absence of evidence for pouchitis predicted the effect of dietary inter- vention on stool frequency. As shown in Figure 1, for the 7 patients without pouchitis median daily stool frequency fell from 8 to 4 (P ϭ 0.001) compared with the 5 patients with pouchitis, where the daily stool frequency rose from 7 to 8 (P ϭ ns). This represents a statistically significant median fall of 3 stools per day compared with no change in those with pouchitis (P ϭ 0.007; t-test).
Qualitative data in the retrospective group suggested
that the degree of reduction in FODMAP intake might predictsymptomatic improvement. Response to dietary change wasseen in both patients (R4 and R5) who had a high baseline
FIGURE 1. Daily stool frequency before and during the low
intake of FODMAPs with strict adherence to the diet. One
FODMAP diet according the presence or absence of evidence of
patient (R2) had a low baseline FODMAP intake, made few
pouchitis. Changes in those without pouchitis were statisticallysignificant (P ϭ 0.001; paired t-test).
dietary changes, and did not respond. Semiquantitative as-
Inflamm Bowel Dis ● Volume 13, Number 12, December 2007
sessment in the prospective group showed that clear symp-
(50%). These observations are of great importance since they
tomatic improvement was observed in Patient P2, who re-
offer an opportunity to reduce the osmotic load to the pouch
duced FODMAP intake by 10 serves per day and partial
or rectum via dietary modification. If attention is also paid to
symptomatic benefit was reported by P4, who reduced by 9
minimizing intake of poorly absorbed oligosaccharides, most
serves per day. No improvement was seen in P5, who reduced
importantly fructans, and of polyols, particularly sorbitol,
by 7 serves per day and P3, who developed acute pouchitis
perhaps the fluid load on the pouch might be significantly
during the study but was strictly adherent and reduced intake
altered. Indeed, semiquantitative assessment of dietary FOD-
by 9 serves per day. Thus, these data suggest that the degree
MAP intake showed a generally modest intake of free fruc-
of reduction in FODMAP intake may be another factor in
tose, with most of the FODMAP intake deriving from fruc-
tans contained in onions and wheat products.
Of the 5 patients who were found to consume a diet low
The main outcome measure was the daily stool fre-
in FODMAPs, 4 had evidence of pouchitis. In contrast, of the
quency. In the retrospective group, this was significantly
9 patients who consumed a diet that contained moderate to
reduced by dietary change, but such a finding was not con-
high amounts of FODMAPs, only 2 had evidence of pouchi-
firmed in the prospective study. However, it was apparent that
tis. This difference was not, however, statistically significant
the responders and nonresponders differed in a clear way.
(P ϭ 0.068, Fisher’s exact test).
The presence of inflammation in the gastrointestinal tract, asdemonstrated by endoscopic examination of the pouch or by
DISCUSSION
the measurement of fecal lactoferrin,12 was strongly associ-
Managing frequency and nocturnal bowel actions is challeng-
ated with failure to change daily stool frequency on the
ing in patients following colectomy and ileoanal pouch anas-
low-FODMAP diet. In contrast, a highly significant reduction
tomosis or IRA. Diet has figured poorly as a therapeutic tool
in daily stool frequency was observed in patients where no
due to inefficacy. Limiting dietary intake of FODMAPs as
evidence of pouchitis was found. Reasons for the lack of
outlined in the present study represents the first dietary ther-
response in patients with inflammation are not clear. There
apy that may reduce stool frequency, at least in the absence of
may be a significant secretory element to diarrhea in associ-
pouchitis or other causes of pouch-associated inflammation.
ation with inflammation. Intestinal transit might also be ac-
The present study was designed to be a ‘proof-of-
celerated in response to inflammation, although studies ex-
concept’ study in that there was no blinding or randomiza-
amining pouch dysfunction have not linked pouchitis with the
tion. It was limited by the fact that several patients were
rapidity of transit.11 Both of these factors, however, would
studied retrospectively, where less precise documentation of
render pouch output and function less responsive to changes
stool frequency is almost certain to occur. Furthermore, the
in the osmotic load. Additionally, it is likely that increased
prospective arm was limited in the selection of patients,
irritability of the pouch in pouchitis may have contributed to
where volunteers responded to advertisements to participate.
stool frequency independently of the volume in the pouch.
This method of recruitment attracted those with problematic
A second possible predictive factor was the degree of
pouches in that at least 5 of the 8 patients had pouchitis, or
reduction in FODMAP intake. Those with high baseline
other cause for inflammation such as cuffitis or pre-pouch
intake of dietary FODMAPs and with good adherence to the
ileitis, as shown by elevated fecal lactoferrin concentrations,
diet responded, while those with a low baseline intake and/or
compared with only 2 of 7 in the retrospective study, who
partial adherence did not. These observations would be an-
were offered the dietary therapy when seen in routine clinical
ticipated from the postulated mechanism for dietary efficacy
practice. Nevertheless, this study did permit important obser-
and, in that way, they support the hypothesis.
A limiting factor of the efficacy of any dietary change
Nearly 50% of patients failed to produce hydrogen in
for a chronic problem is the ability of patients to follow
response to a load of lactulose compared with less than 10%
dietary instruction and to maintain adherence in the long
across healthy populations and patients with functional gut
term. We have previously found that long-term adherence can
disorders.8 This was similar to the observations of Santa-
be achieved in at least 3 out of 4 patients with functional gut
verta,13 where 32% of subjects had no hydrogen response to
disorders.10 Patients who had responded to the diet in the
lactulose in the only previous study describing hydrogen
retrospective group did, on self reporting, adhere to the di-
production in patients with an ileal pouch. It may well relate
etary guidelines in the longer term. Reasons for such success
to the length of time the lactulose is in contact with bacteria
include the perception of continuing efficacy and the inter-
or to the type of bacteria present in the pouch or rectum. It did
mittent reinforcement associated with a relapse of symptoms
not correlate with the presence of inflammation. In those who
when excluded foods were again consumed. The fact that the
did produce detectable hydrogen, fructose malabsorption was
majority of patients remain adherent to the diet most of the
common, being seen in 7/8 (88%) patients with a J pouch or
time is in itself a testament to the diet’s efficacy. Long-term
IRA. Likewise, lactose malabsorption was found in 4 patients
follow-up in the prospective group was not possible, but it
Inflamm Bowel Dis ● Volume 13, Number 12, December 2007
was interesting that 6 weeks after the completion of the
positive impact on the quality of pouch function in such
formal treatment part of the study the patient with excellent
patients. Further prospective evaluation of this approach in a
improvement of symptoms continued on the diet and that 2
larger population of patients without pouchitis, in whom
patients who had some or little efficacy reported during the
baseline dietary intake is evaluated, is needed to determine
treatment period had continued with some of the dietary
whether the diet indeed has an important role in improving
restrictions, presumably since they had now recognized and
experienced direct precipitation of increased or more frequentpouch output in response to specific FODMAP-rich foods. REFERENCES
There may be potential risks of reducing dietary intake
1. Lichtenstein GR, Cohen R, Yamashita B, et al. Quality of life after
of FODMAPs. The prebiotic effect of fructose and fructans is
proctocolectomy with ileoanal anastomosis for patients with ulcerative
well demonstrated.14 One study has provided evidence that
colitis. J Clin Gastroenterol. 2006;40:669 – 677.
2. Michelassi F, Lee J, Rubin M, et al. Long-term functional results after
dietary supplementation with a large dose of inulin (24 g/day)
ileal pouch anal restorative proctocolectomy for ulcerative colitis: a
reduced pouch inflammation in patients with pouchitis.6 In-
prospective observational study. Ann Surg. 2003;238:433– 441.
ulin is a long-chain fructan and is different in this respect to
3. Pardi DS, Sandborn WJ. Systematic review: the management of pou-
chitis. Aliment Pharmacol Ther. 2006;23:1087–1096.
the short-chain (oligosaccharide) fructans that make up the
4. Shen B, Achkar JP, Lashner BA, et al. Irritable pouch syndrome: a new
majority of dietary fructans. However, it does exhibit similar
category of diagnosis for symptomatic patients with ileal pouch-anal
prebiotic effects to fructose and fructo-oligosaccharides.13
anastomosis. Am J Gastroenterol. 2002;97:972–977.
5. Thirlby RC, Kelly R. Pectin and methyl cellulose do not affect intestinal
This raises the possibility that reduction in dietary fructans as
function in patients after ileal pouch-anal anastomosis. Am J Gastroen-
well as fructose might lead to a less favorable spectrum of
bacteria in the pouch. Indeed, 1 patient in the study had
6. Welters CF, Heineman E, Thunnissen FB, et al. Effect of dietary inulin
supplementation on inflammation of pouch mucosa in patients with an
worsening symptoms on the low FODMAP diet, although
ileal pouch-anal anastomosis. Dis Colon Rectum. 2002;45:621– 627.
fecal lactoferrin level was elevated prior to commencing the
7. Tomita R, Fujisaki S, Tanjoh K. Relationship between gastrointestinal
diet. There was also a tendency for patients with pouchitis to
transit time and daily stool frequency in patients after Ileal J pouch-analanastomosis for ulcerative colitis. Am J Surg. 2004;187:76 – 82.
consume a low amount of FODMAPs in their usual diet.
8. Gibson PR, Shepherd SJ. Food for thought: Western lifestyle and sus-
Further studies are required to determine whether the associ-
ceptibility to Crohn’s disease: the FODMAP hypothesis. Aliment Phar-
ation of low FODMAP intake with pouchitis is indeed real. macol Ther. 2005; 21: 1399 –1409.
9. Gibson PR, Newnham E, Barrett JS, et al. Systematic review: fructose
In conclusion, the present study suggests that reduction
malabsorption and the bigger picture. Aliment Pharmacol Ther. 2007;
of dietary FODMAPs in patients with ileal pouch or IRA may
be efficacious in reducing stool frequency in patients who do
10. Shepherd SJ, Gibson PR. Fructose malabsorption and symptoms of
irritable bowel syndrome: guidelines for effective dietary management.
not have active pouchitis or other inflammation associated
J Am Diet Assoc. 2006;106:1631–1639.
with the pouch, especially in those who consume at least
11. Madsen JL, Linnet J, Rumessen JJ. Effect of nonabsorbed amounts of a
modest quantities of FODMAPs in their usual diet. The high
fructose-sorbitol mixture on small intestinal transit in healthy volunteers. Dig Dis Sci. 2006;51:147–153.
prevalence of fructose and lactose malabsorption indicates
12. Parsi MA, Shen B, Achkar JP, et al. Fecal lactoferrin for diagnosis of
that reduction of the intake of free fructose and lactose should
symptomatic patients with ileal pouch-anal anastomosis. Gastroenterol-
be integral to the dietary approach. Taken together with the
13. Santavirta J. Lactulose hydrogen and [14C]xylose breath tests in patients
observation that 1 in 2 patients are nonhydrogen producers,
with ileoanal anastomosis. Int J Colorectal Dis. 1991;6:208 –211.
the performance of breath hydrogen tests probably contrib-
14. Hopkins MJ, Cummings JH, Macfarlane GT. Inter-species differences in
utes little to dietary design. The application of the FODMAP
maximum specific growth rates and cell yields of bifidobacteria culturedon oligosaccharides and other simple carbohydrate sources. Selective
approach to reducing the osmotic load on the ileal pouch or
stimulation of bifidobacteria in the human colon by oligofructose and
rectum represents the first dietary strategy likely to have a
inulin. J Appl Microbiol. 1998;85:381–386.
New York State Chiropractic AssociationBoard of Directors and House of Delegates Meeting Fort William Henry Hotel & Convention CenterA. Budget B. Accountant’s Report C. Expenditures D. Legal Expenses E. NYCPAC Contribution Report ( Oliver ) F. Controller’s Report to the District Treasurer’s, Re: District Bank Accounts VI. Chiropractic Education Foundation of New York (CEFNY)VII. Chi
For the many families and teachers of school-aged children, head lice continue tocreate some concerns and cause minor frustration. Curtis School intends to outlineroles, responsibilities, and expectations of the school community to assist with treatingand controlling head lice in a consistent and coordinated manner. While parents havethe primary responsibility for the detection and treatm
 Inflamm Bowel Dis ● Volume 13, Number 12, December 2007
TABLE 2. Quantification of FODMAP Intake According to Prospectively Completed 7-Day Food Diaries
Inflamm Bowel Dis ● Volume 13, Number 12, December 2007
TABLE 2. Quantification of FODMAP Intake According to Prospectively Completed 7-Day Food Diaries