Standard Operating Procedure (SOP) Clinical samples – WP6, WP1 and WP5 – Category: BUD Patient Collection, transport and storage of diagnostic specimens and clinical samples KNUST/Ghana Version 1 19.08.2010 1. General considerations
This document describes the standard operating procedures applied for collection, transport and storage of diagnostic specimens and clinical samples within BuruliVac work packages WP1/6, WP5/6, or WP6 only. To reduce the amount of blood drawn, different cohorts are enrolled in WP1/6 and WP5/6. Patients clinically suspected for BUD who deny to participate in one of the immunological work packages will be enrolled in WP6 (diagnostics) only.
Currently WHO recommendations for diagnostic sample collection are under revision. Therefore it may become necessary to revise this document in the near future.
▲Before any patient is enrolled in the different work packages of BuruliVac and clinical specimens are collected, ensure that informed consent of the patient or legal representative has been obtained! 2. Specimen collection 2.1 Clinical specimens for laboratory confirmation of clinical BUD suspects – WP6
According to the kind of BUD lesion standardized specimen collection procedures are applied in Ghana as indicated in table 1. Currently, there is broad consensus among BUD experts that FNA samples are to be favoured over punch biopsies. Several aspects of patient management however, may still require the collection of punch biopsies. Among indications that justify the collection of punch biopsies are:
• Strong clinical suspicion but negative FNA sample(s)
• Differential diagnosis • Paradoxical reaction
• Possible recurrence (confirmation by culture)
• Treatment failure (confirmation by culture) • Drug susceptibility testing by culture if evidence for drug resistant strains
The question as to whether punch biopsies could be replaced by FNA for mycolactone extraction has not yet been assessed and so for the research questions addressed in work package 1, currently there is no alternative for punch biopsies. WHO is in the process of issuing new guidelines on different sampling techniques to confirm Buruli Ulcer. If these guidelines are available, this document may have to be subjected to revision.
Nodule, Papule, Plaque, Edema Specimens for PCR (per lesion) 1 Tissue punch* Specimens for Microscopy and Culture (per lesion)
1 Tissue punch**
Two FNA samples are collected for PCR per lesion. *strong clinical suspicion, but negative result from FNA **required for culture as long as the debate on the sensitivity of FNA vs. punch has not been resolved
Undermined lesions Non-undermined lesions Surgical patients
specimens for PCR (per lesion) 1 Swab 1 Tissue punch alternatively Tissue surgery***
specimens for Microscopy and Culture (per lesion) 1 Swab 1 Tissue punch alternatively Tissue surgery***
Two swab samples are collected for PCR, and MIC/CUL from ulcers with undermined edges. For lesions that are not undermined FNA or punch biopsy is more appropriate than swabs (hereby FNA will be the first choice). ***Tissue from surgery will only be collected if lesions of patients on antibiotic therapy require debridement and/or skin grafting. Tissue samples however are divided for CUL, MIC & PCR by means of a sterile scalpel.
Other (Osteomyelitis) Specimens for MIC, CUL & PCR 1 Tissue surgery
Surgical samples will be most appropriate after x-rays have been taken to confirm the presence of osteomyelitis. Tissue obtained from surgery will be divided for PCR, MIC and CUL. Table 1 2.1.1 Specimen collection bags (WP1/6 and WP5/6)
Collection of diagnostic samples will apply the standardized specimen collection bags as used in previous studies conducted by KNUST and LMU. Pre-packed specimen collection bags are provided to the treatment centres by the KNUST Team. Specimen bags contain all containers filled with transport and storage media suitable to preserve specimens for all laboratory tests that are conducted within work package 6 at KCCR laboratories.
Different containers are labelled to display the diagnostic test they are subjected to. Each bag is labelled with the packing date of the bag to determine the expiry date of reagents. The specimen bags can be stored at room temperature for 6 months, after that period of time materials are replaced. Unused reagents are then discarded.
Each bag contains BuruliVac laboratory data entry forms and BU01 forms for data collection.
For diagnostics (WP6) 2 different types of specimen collection bags are prepared at KCCR and provided to the BUD clinics/treatment sites for WP6:
A) Clinical specimen collection bags for WP-6 – non-ulcerative lesions B) Clinical specimen collection bags for WP-6 – ulcerative lesions ▲Per lesion one specimen collection bag is used!
2.1.1.1 Content of clinical specimen collection bags for WP-6 – non-ulcerative lesions
1 BuruliVac data entry form 1 BU01.N form (if relapse the BU01.R form is applicable) 2 needles, 21 G (gauge) for FNA
2 butterfly needles for FNA alternatively
2 syringes (5 ml, sterile) 2 FNA containers (2 x CLS, 300 µl in 2 ml screw cap tubes) For cases that justify the collection of a punch biopsy (as described under 2.1) a number of spare specimen collection bags with equipment for punch biopsies will be available.
Biopsy punch (3 mm) Container for punch biopsy (700 µl CLS in 2 ml screw cap tube)
2.1.1.2 Content of clinical specimen collection bags for WP-6 – ulcerative lesions
1 BuruliVac data entry form 1 BU01.N form (if relapse the BU01.R form is applicable) 2 swabs 2 swab containers (1x 700 µl CLS, 1 x 4 ml PANTA, swabs are taped to containers)
It can be assumed that in most cases swabs can be taken. For the rare cases with edges that are not undermined, the KNUST Team will provide a number of spare specimen collection bags with equipment for FNA and punch biopsies:
syringes (5 ml, sterile) FNA containers (300 µl CLS) Biopsy punch (3 mm) Containers for punch biopsy (4 ml PANTA, 700 µl CLS)
In cases where an item in the bag is not used, it is returned to project staff. Table 2 provides detailed information on transport conditions.
Specimen Diagnostic test Transport medium Transport container
*PANTA: Polymyxin B, Amphotericin B, Nalidixic acid, Trimethoprim, Azlocillin **CLS: Cell lysis solution (Qiagen, Gentra Systems, USA) ***FNA samples primarily for DRB-PCR, will also be used for Microscopy 2.1.2 Preparation of PANTA transport media â–˛Preparation of PANTA transport media should be carried out in the culture laboratory under sterile conditions!
Dissolve 1.5 g Dubos Broth Base in 204 ml distilled water. Add 12 ml glycerol and autoclave at 121°C for 15 minutes. Let the mixture cool down below 50 °C and add 24 ml Dubos medium albumin.
Dissolve each PANTA (Polymyxin B, Amphotericin B, Nalidixic acid, Trimethoprim, Azlocillin) vial in 3 ml sterilized distilled water under sterile conditions. The PANTA antibiotic mixture is then ready for use.
To produce the PANTA transport medium add 6 ml of PANTA antibiotic mixture to the autoclaved Dubos Broth Base/glycerol mixture under sterile conditions.
Under sterile conditions add 4 ml of PANTA transport medium into each sterile transport container tube. Label the tubes with “PANTA transport medium”.
2.2 Clinical samples for immunological research - WP1, WP5
The following table indicates clinical samples collected from study participants enrolled in WP1 and WP5.
Work package Heparinized blood Punch biopsy â–˛Only children over the age of 5 years are eligible for participation in WP1 or WP5! 2.2.1 Clinical specimens for WP1 patients
For collection of immunological specimens the following items will be needed:
1 Sodium heparin tube (green top, 10ml) 1 vacutainer adaptor 2 vacutainer needles one 21 G (for adults) & one 23 G (for children) 2 alcohol swabs 1 urine bottle 1 urine collection bag 1 punch biopsy needle (3mm)
These items will be prepared at KCCR and provided to the BUD clinics.
â–˛No punch biopsy for children under the age of 10 years for WP1!Follow-up punch biopsies will only be collected if the lesion is not closed yet. The following samples are collected for WP1 from adults and children over the age of 10 years:
Before start of treatment, at the same time as the collection of diagnostic samples for WP6, the following specimens will be obtained from each patient: 10 ml venous blood, 10 ml urine, 1 punch biopsy (3 mm)
During and after treatment, the following additional samples will be collected at week 6, 12 and 48 after start of treatment: 10 ml venous blood, 10 ml urine; 1 punch biopsy (3mm, only if the lesion is not yet closed) The following samples are collected for WP1 from children aged 5-10 years: Before start of treatment, at the same time as the collection of diagnostic samples, the following specimens will be obtained from each patient: 6 ml venous blood, 10 ml urine
During and after treatment, the following additional samples will be collected at week 6, 12 and 48 after start of treatment: 6 ml venous blood, and 10 ml urine 2.2.2 Clinical specimens for WP5 patients
For collection of immunological specimens the following items will be needed:
1 Sodium heparin tube (green top, 10ml) 1 Serum tube (red top, 3ml) 1 vacutainer adaptor 2 vacutainer needles one 21 G (for adults) & one 23 G (for children) 2 alcohol swabs
These items will be prepared at KCCR and provided to the BUD clinics.
The following blood samples are collected for WP5 from adults and children over the age of 10 years:
Before start of treatment, at the same time as the collection of diagnostic samples, the following specimens will be obtained from each patient: 2 tubes of venous blood (10 ml, 3 ml – a total of 13 ml blood) During and after treatment, the following additional samples will be collected at week 6, 12 and48 after start of treatment: 2 tubes of venous blood (10 ml, 3 ml – a total of 13 ml of blood) The following blood samples are collected for WP5 from children aged 5-10 years:
Before start of treatment, at the same time as the collection of diagnostic samples, the following specimens will be obtained from each patient: 2 tubes of venous blood (6 ml and 2 ml – a total of 8 ml of blood) During and after treatment, the following additional samples will be collected at week 6, 12 and 48 after start of treatment: 2 tubes of venous blood (6 ml and 2 ml – a total of 8 ml of blood) 2.3 Procedure of sampling ▲In Ghana, diagnostic BUD samples will be collected by resident physicians and/or trained BUD study nurses under supervision of the resident physicians only! 2.3.1 Diagnostic samples for laboratory diagnosis of BUD – WP6 ▲Prior to specimen collection the longitudinal and transversal diameters of the lesion are determined (in mm) and registered on the laboratory data entry form.
To obtain a swab specimen first explain the procedure to the patients. Swab underneath the undermined edge twirling the sterile swab on an applicator and circling the entire undermined edge of ulcers as indicated in Fig.1.
Fig. 1. Specimen collection for diagnostic swabs from ulcerative lesions with undermined edge u.e.: underminded edge of ulcer. The swab is placed into the respective container and labelled. Samples for culture and microscopy will be placed in 4 ml transport buffer (PANTA), samples for PCR are placed in 2 ml screw cap tubes containing 700 µl CLS.
The procedure of FNA collection is described according to current WHO recommendations:
1. The lesion is carefully inspected and palpated 2. The site of the lesion for doing the aspiration is determined and disinfected using an
alcohol soaked swab. It is advisable to obtain the FNA from the centre of the lesion or to identify weak areas in the case of non ulcerated oedematous lesions
3. The syringe and needle (sterile 21 G needle or preferably a butterfly needle, 2ml or
4. For nodules and small plaques, the lesion is grasped with one hand and hold in a fixed
5. Using the other hand, the needle is inserted into the estimated centre of the lesion and
move back and forth (about 3 times) within the subcutaneous adipose tissue in different directions without withdrawing through the skin and suction is applied each time the needle is moved forth
6. Finally, the needle is withdrawn. To prevent ulceration, the respective needle must not
FNA is suitable for microscopy and PCR. For PCR needle tips are inserted into the respective transport medium (CLS) and flushed to wash the aspirate into the container (note that the aspirate may not be visible) and the tube is labelled. The procedure is repeated twice. The same fluid may be used for microscopy.
In addition, due to an assumed higher sensitivity one slide is prepared on site by flushing the needle content onto a slide with frosted ends for microscopy. The slide is labelled and stored in the respective specimen collection bag for KCCR laboratories.
Punch biopsy
Diagnostic tissue specimens from pre-ulcerative lesions are collected from the centre of the lesion (Fig. 2) or, in case of ulcers without undermined edges, from the necrotic margin of ulcers bordering healthy (viable) tissue (Fig. 3) using a 3 mm biopsy punch. By determining the location of specimen collection, special attention must be paid to anatomically underlying neuro-vascular structures in the area of the defined biopsy site. The area of specimen collection must be draped. Local anaesthesia with 1 % lidocaine is administered. The skin must be stretched perpendicular to skin tension lines, then the biopsy punch is rotated into the dermis and fully into the subcutaneous adipose tissue. For diagnostic purposes it is mandatory that tissue specimens contain the subcutaneous adipose tissue as mycobacteriaare present in that layer. The punch biopsy must be elevated above the incision level, if necessary by using sterile forceps, and excised using a sterile scalpel. The specimens are placed into the respective transport container. The punch biopsies for mycolactone detection (WP1) will be snap frozen in liquid nitrogen. The wound closes in most cases by itself and adequate wound dressing is sufficient. Sometimes it may be necessary to apply 1-2 stitches (these are usually removed after 7-10 days).
Fig. 2. Punch biopsy, non-ulcerative lesion (e.g. nodule, plaque)
The black dots indicate 3 possible locations for collection of a punch biopsy
Fig. 3. Punch biopsy, ulcerative lesion without undermined edge
The black dots indicate 3 possible locations for collection of a punch biopsy
Surgical tissue samples
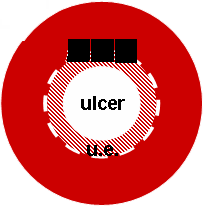
Surgically excised tissue specimens are collected at the time of surgery (if conducted for individual patients). Diagnostic tissue specimens from ulcerative lesions are collected from the edge of the lesion below the end of the undermined edge of the ulcer and must contain necrotic tissue. Surgically excised tissue from pre-ulcerative lesions, such as nodules and plaques, must contain material from the centre of the lesion. (Fig. 4) A new pair of sterile gloves is used to prepare sterile forceps and sterile scalpel. The excised tissue is spread on sterile gauze. For diagnostic purposes it is mandatory that tissue specimens contain the subcutaneous adipose tissue as Mycobacterium ulcerans is found in that layer. Tissue from non-ulcerative lesions is cut longitudinally and horizontally in four equal segments, each of those must comprise a part from the centre of the lesion. Pieces of a
maximum size of 1 cm x 1 cm are then transferred to the respective specimen collection containers containing transport medium (4 ml PANTA) for microscopy and culture and 700 µl CLS for PCR.
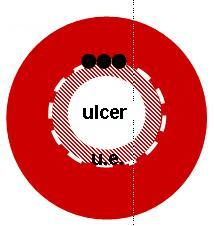
left: ulcerative lesion; right: pre-ulcerative lesion
Black squares indicate the location for collection. u.e.: underminded edge of ulcer.
Venous blood samples
Blood samples will be collected by trained study nurses after explaining the procedure to the patient (under supervision of the study physician, Dr. Fred Stephen Sarfo). A tray containing a sterile alcohol swab, tourniquet, vacutainer tube, adaptor and needle (Please note: 23 G for children aged 5-10 years, and 21 G for all others) will be available. A tourniquet is wrapped around the upper arm proximal to the site where the needle is pierced into the vein. The area where the needle pierces the skin is disinfected. Whole blood is drawn from a vein, usually the medial cubital vein at the elbow after insertion of the needle into the vein. After the collection tubes are filled the tourniquet is loosened, the needle withdrawn and a pad is pressed for some minutes to stop bleeding. Heparin tubes are gently turned upside down once, labelled and placed in stable racks. Serum tubes are placed directly into the stable racks. Urine
The patient will be asked to void urine (note: midstream is not necessary) in a sterile urine container. This container is labelled and placed into urine collection bags.
3. Transport of clinical samples
Diagnostic samples are transported in the respective collection bag with enclosed laboratory data entry forms and BU01 forms by the KNUST study team to KCCR laboratory by means of a study vehicle. Heparinised whole blood and serum collected will be kept in stable racks after labelling to reduce agitation and hemolysis. Punch biopsy tissue obtained for mycolactone research will be snap frozen in liquid nitrogen and transported using a dry shipper. Urine specimen will be kept in urine specimen collection bags. Specimen collected will be transported to the KCCR laboratories for processing by means of a study vehicle.
Blood samples and urine for the immunology work packages (WP1, WP5) are transported under the following precautions: Transport condition max. time of transport envisaged
Urine sample will be kept in a cooling box
3 mm punch biopsy Snap frozen in liquid nitrogen
4. Storage of diagnostic specimens and immunology samples 4.1. Storage of diagnostic specimens
Upon arrival at KCCR laboratories, all diagnostic samples are stored in 4 ml PANTA medium or 700 µl CLS at 2-8°C until further processing. For long term storage DNA extracts are kept at -20° C. 4.2. Storage of immunology samples (WP1, WP5) Immunological samples will also be transported to the KCCR laboratories and processed immediately. Heparinized blood samples will be processed immediately. Serum, punch biopsy and urine will be stored at –80oC.
Expert health and behavior advice from the feline care professionals at Paws, Whiskers & Claws The Feline Hospital Your cat’s kidneys are essential to her health. Their main functions are to filter protein waste from the blood, regulate the level of essential nutrients such as potassium and phosphorus, maintain hydration, and produce urine. They also help to regulate the catâ€
Clear Cell Line containing Benzoyl Peroxide by Marc A. Ronert MD PhD, Clinical Director Image Skincare Image Skincare offers products with many active, scientifically proven and researched key ingredients to achieve a certain result on the skin. In order to achieve the maximum benefit, not only one key ingredient, but an array of synergistically working ingredients, to target specific s
 Standard Operating Procedure (SOP)
Standard Operating Procedure (SOP) 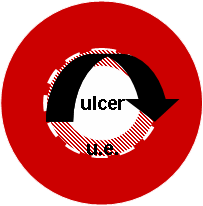 2.3 Procedure of sampling
2.3 Procedure of sampling 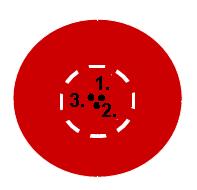
 In addition, due to an assumed higher sensitivity one slide is prepared on site by flushing the needle content onto a slide with frosted ends for microscopy. The slide is labelled and stored in the respective specimen collection bag for KCCR laboratories.
Punch biopsy
In addition, due to an assumed higher sensitivity one slide is prepared on site by flushing the needle content onto a slide with frosted ends for microscopy. The slide is labelled and stored in the respective specimen collection bag for KCCR laboratories.
Punch biopsy 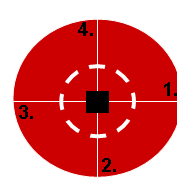
 maximum size of 1 cm x 1 cm are then transferred to the respective specimen collection containers containing transport medium (4 ml PANTA) for microscopy and culture and 700 µl CLS for PCR.
left: ulcerative lesion; right: pre-ulcerative lesion
Black squares indicate the location for collection. u.e.: underminded edge of ulcer.
maximum size of 1 cm x 1 cm are then transferred to the respective specimen collection containers containing transport medium (4 ml PANTA) for microscopy and culture and 700 µl CLS for PCR.
left: ulcerative lesion; right: pre-ulcerative lesion
Black squares indicate the location for collection. u.e.: underminded edge of ulcer.