House dust mite avoidance for children with asthma in homes of low-income families Gail G. Shapiro, MD,a Timothy G. Wighton, PhD,a Tamara Chinn, RN,a Jon Zuckerman, BA,a A. Heather Eliassen, BA,a Joseph F. Picciano, BA,a and Thomas A. E. Platts-Mills, MD, PhDb Seattle, Wash, and Charlottesville, Va Background: Home exposure to high levels of house dust mite allergen has been shown to aggravate airways reactivity and Objective: The purpose of this study was to determine whether specific house dust mite control measures could reduce expo- sure levels and asthma severity.
ways inflammation and clinical disease.5-9 Secondary
Methods: This double-blinded, randomized trial compared
variables included assessment of symptoms, quality of
asthma progression over 1 year in children whose homes
life, spirometry, urgent care, and hospital visits, as well
received standard environmental control intervention with
as prednisone courses for acute exacerbations. those whose homes received aggressive intervention for dust mite elimination. The primary end point was doubling in PD20 methacholine. Patient selection and clinical measures Results: Symptom scores and quality-of-life scores were simi- lar for the standard and aggressive intervention groups. PD20
This study represents a double-blinded, randomized clinical
methacholine doubling occurred in 9 members of the aggres-
trial; only the home dust collector was unblinded, and he did not
sive intervention group vs 4 control patients (P < .05). Dust
communicate home information to others. Children aged 6 to 16
mite levels decreased in the aggressive intervention homes
years with asthma were recruited from clinics that serve lower
compared with the standard intervention homes (P < .05).
socioeconomic neighborhoods. The children had been diagnosed by
Conclusion: Aggressive dust mite intervention decreased dust
a physician as having asthma and satisfied the definition of having
mite levels and improved bronchial hyperresponsiveness. (J
mild-to-moderate persistent disease according to criteria set forth in
Allergy Clin Immunol 1999;103:1069-74.)
the National Heart, Lung, and Blood Institute guidelines.10 Thesecriteria included 1 or more of the following: cough or wheeze more
Key words: Asthma, dust mite, bronchial hyperresponsiveness,
than once a week, nocturnal symptoms, documentation of peak
expiratory flow rate (PEFR) at 60% to 80% of predicted level, andcurrent asthma symptoms causing some impairment to normal
There is growing concern in the medical and lay com-
activity, including school performance. In addition, patients had to
munities that asthma should be treated more aggressive-
meet all of the following inclusion criteria: (1) at least 1 urgent care
ly from both an environmental and pharmacotherapeutic
visit caused by asthma in the previous 6 months; (2) history of
point of view. Continuous exposure to high levels of
required albuterol at least 5 times per month; (3) positive metha-
environmental allergens, in particular house dust mites,
choline challenge response at a concentration of 10 mg/mL or less;
has been shown to aggravate airways reactivity and may
and (4) positive skin prick test response to Dermatophagoides
be a critical factor in the development and perpetuation
pteryonyssinus, Dermatophagoides farinae, or both (ie, wheal
diameter at least 3 mm greater than that produced by the saline con-
The goal of this study was to determine whether spe-
trol). Patients were excluded if their families were already carryingout environmental control measures in the home as reported by the
cific house dust mite control measures could reduce
field staff on the first home visit.
exposure levels to this allergen and, subsequently, reduce
Parents and older children consented (and younger children
the severity of asthma in children. The primary end point
assented) to be randomized to either a standard or aggressive envi-
was change in airways reactivity to methacholine
ronmental control program. The trial was approved by the Investi-
because this response can be roughly correlated with air-
gational Review Board of Children’s Hospital and Regional Med-ical Center, Seattle, Washington.
At the initial visit, all patients provided a history and underwent
physical examination, quality-of-life assessment, and skin prick
From aA.S.T.H.M.A., Inc, Seattle; and bthe Division of Allergy, University of
tests to dust mites, cat, cockroach, and regional pollens. Spirometry
Virginia Medical Center, Charlottesville.
was performed, with short-acting β-agonists having been withheld
Supported by National Institute of Allergy and Infectious Diseases grant #1
for at least 4 hours. Patients were instructed on peak flow tech-
UO1 AI34578-01, AI/ES-34607, and AI-20565.
niques and charting of peak flow and symptoms, which was to be
Received for publication Oct 29, 1998; revised Mar 2, 1999; accepted for
done morning and night. Patients received cromolyn, nedocromil, or
triamcinolone metered-dose inhalers at the discretion of the investi-
Reprint requests: Gail G. Shapiro, MD, A.S.T.H.M.A., Inc, 4540 Sand Point
gator, with the inhaled steroid (ie, triamcinolone) being reserved for
those with more severe disease, as determined by history of
1/1/98647
albuterol use and pulmonary function. 1070 Shapiro et al TABLE I. Baseline characteristics of the study population TABLE II. Doubling PD20 methacholine Standard Aggressive
es), change in FEV1 levels (classified as mild, moderate, or severe),
and changes in household dust mite concentration (classified as low,
moderate, or high). In each of these analyses, P values of less than
.05 were considered indicative of statistically significant group dif-
Four weeks later, patients returned for methacholine challenge,
and diaries were reviewed. A home visit occurred soon after this at
Patient sample
which patients were randomized to the standard or aggressive envi-ronmental intervention arms. Patients were again seen in the clinic
Forty-four patients were randomized, and 36 complet-
after 6 and 12 months for history, physical examination, quality-of-
ed the evaluation. Five patients (3 in the standard and 2
life assessment, spirometry, and methacholine challenge. Peak flow
in the aggressive intervention groups) failed to complete
and symptom diaries were collected, and families were questioned
the trial because of noncompliance with medications and
regarding their children’s asthma severity in this interval compared
visits. Three (2 in the standard and 1 in the aggressive
with baseline values. Sequential pulmonary function and metha-
intervention groups) failed to complete the study because
choline challenges were done at approximately the same time of
of worsening asthma: 1 patient withdrew on the advice of
day and at least 30 days after steroid bursts.
his primary care doctor, and 2 were withdrawn when
Home intervention and analysis
FEV1 values were too low to allow methacholine chal-
Standard intervention included a general discussion of the need
to dust and vacuum the house weekly and avoid clutter in the bed-
Mean age and racial distribution were similar between
room. The home visit to patients in this group involved vacuuming
groups. Racial minorities are overrepresented in this
of pillow and mattress, application of tannic acid placebo to the
sample compared with the composition of the greater
child’s bedroom carpet every 4 months, and phone call reminders to
Seattle area, where the minority population is approxi-
families to spray tannic acid placebo on carpets at 2, 6, and 10
mately 13% (communication from Chamber of Com-
months. Aggressive intervention consisted of the application of dust
mite–impermeable covers (donated by Allergy Control Products,
Medication profiles of the groups were similar, with 9
Inc, Ridgefield, Conn) to mattress, box spring, and pillow; laundry
and 11 of the standard and aggressive intervention
service delivery of a clean blanket and 4 sets of bed linens every
patients, respectively, taking cromolyn; 5 standard and 7
month; and tannic acid application to the bedroom and living roomcarpet every 2 months. Families were instructed to dust and vacuum
aggressive intervention patients taking triamcinolone;
weekly and to avoid clutter. A vacuum cleaner was provided if a
and 3 standard and 1 aggressive intervention patient
family in either group lacked one, which occurred in only one
using albuterol only in spite of anti-inflammatory recom-
instance. With each delivery of bedding, compliance with environ-
mendations. This changed little during the trial.
mental intervention (eg, special covers on beds) was confirmed.
Dust samples were collected from all homes at baseline and 4, 8,
Diaries and symptoms
and 12 months after randomization. The collection procedure con-
Attempts to collect daily symptom and peak flow
sisted of 2 minutes of vacuuming of the following areas: 2 m2 of the
diaries were futile. Although patients were encouraged to
upper surface of the child’s mattress (sheets removed but special
mail these, there were no reminder calls built into the
encasings in place), 1 m2 of carpet near and underneath the child’s
protocol. Symptom scores and quality-of-life outcomes
bed, a major piece of upholstered furniture in the family area, 1 m2of carpet underneath a major piece of upholstered furniture in the
were assessed at baseline and at 6- and 12-month visits.
family area, and 1 m2 of the kitchen floor. The technique for prepa-
Parents rated their child’s asthma severity as mild, mod-
ration, storage, and analysis of the samples has been described.11
erate, or severe. There were no significant changes frombaseline to 12 months for each group nor were there any
Statistical analysis
differences between the groups. Quality of life was mea-
Logistic regression was used to detect a significant effect of the
sured on a 14-point scale, with 0 representing no symp-
aggressive household intervention compared with standard treat-
toms and 14 representing many symptoms. These scores
ment. A doubling in PD20 dosage units, determined by using base-
were similar for the groups and did not change during the
line and 12-month follow-up results, was compared between groups
year. Exacerbations measured in terms of hospitaliza-
after adjusting for baseline concentrations of dust mite in the home
tions, emergency department visits, and steroid bursts
and baseline levels of bronchial hyperresponsiveness (in PD20
were similar for the 2 groups. Although there were more
dosage units). The chi-squared statistic was used to detect signifi-cant differences between groups for categorical measures, including
steroid bursts for the standard than for the aggressive
the incidence of patient exacerbation during the course of the study
intervention group (11 vs 5), this did not reach statistical
(emergency department visits, hospitalizations, and steroid cours-
Shapiro et al 1071 TABLE III. Medication use of patients with PD20 doubling Patient no. Baseline medication PD20 (dosage units) 12-month medication PD20 (dosage units) prn, As required; qd, daily; bid, twice daily; tid, three times daily; qid, four times daily. Pulmonary function and methacholine
The same was true for Can f 1 (dog antigen). Table IV
reactivity
lists the relative amounts of pet antigen in homes. For catantigen, the number of patients with a positive skin prick
Pulmonary function was similar between groups at the
test response and the number of patients with a cat in the
beginning and end of the trial. Mean FEV1 (L/sec) was
home in addition to having a positive skin test response
1.93 ± 0.97 for the standard intervention group and 1.85 ±
are noted. Skin testing for dog antigen was not performed.
0.56 for the aggressive intervention group at baseline, with
Cockroach antigen concentration (Bla g 2) was mea-
little change during the year. Describing asthma on the
sured as being low (<1 µg/g dust), moderate (1 to <8
g/g dust), or high (≥8 µg/g dust). Only 3 samples con-
dicted value), moderate (60% to 79% of predicted value),
tained moderate levels; the rest were low.
or severe (59% or less of predicted value), the groups had
Correlation of PD
a similar composition, which was constant for the year. 20 doubling, dust mite con-
Bronchial hyperresponsiveness, measured as PD
centration, and cat antigen concentration
showed initial similarity between the groups. The 12-
There was no direct correlation between changes in
month challenge showed a more pronounced increase in
PD20 and dust mite level (Fig 2). No threshold determi-
PD20 for the aggressive intervention group than the stan-
nation appeared to change this. The 13 patients (4 in the
dard intervention group. There was a doubling of PD20
standard and 9 in the aggressive intervention groups)
for 4 members of the standard intervention group and 9
who experienced a doubling of PD20 had a mean
members of the aggressive intervention group (P = .049).
decrease in house dust mite concentration of 5.4 µg/g,
Changes in PD20 are seen in Tables II and III. Changes in
and those who did not had a mean decrease of 2.4 µg/g.
daily asthma therapy, including controlling for inhaled
The presence of cats did not have a predictable effect
steroid use, did not account for this difference.
on dust mite environmental control outcome. The 7patients with positive skin test responses to cat antigen
Antigen content of dust samples
and a cat in the home had a mean increase in PD20 of 10.9
Antigen content of samples showed abundant quanti-
dosage units, and those without cat had a mean increase
ties of dust mite, cat, and dog allergen. The quantities of
of 7.8 dosage units, showing that the presence of a cat did
cockroach allergen were very low. Dust mite (pooled Der
not prohibit improvement in PD20. Removing the 7
p 1 and Der f 1) concentration was categorized as low (<2
patients with positive skin test responses to cat antigen
µg/g dust), moderate (2 to <10 µg/g dust), or high (≥10
and a cat in the home from analysis reduces the power
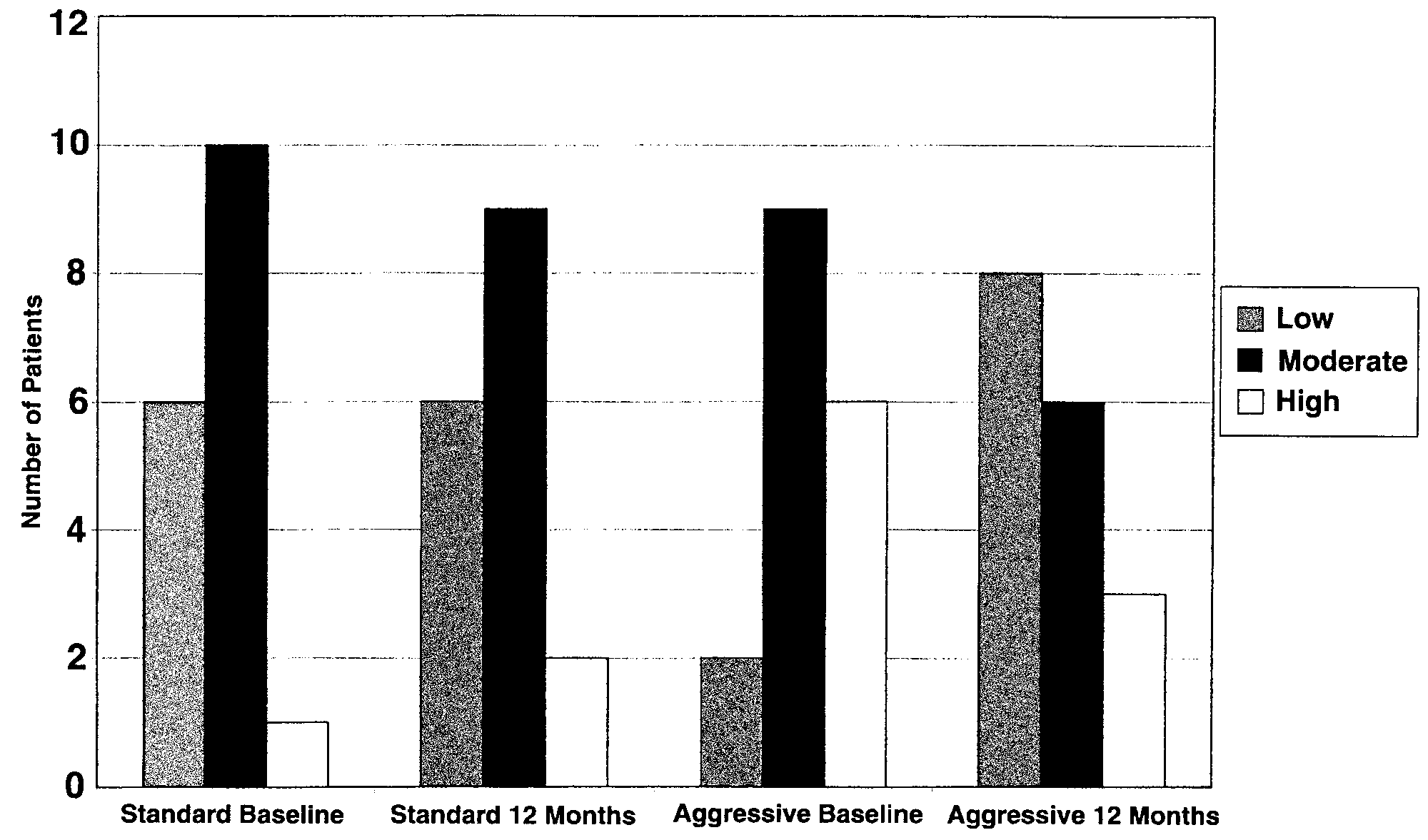
µg/g dust). A change in designation to a lower category
substantially. The relationship between doubling PD20
occurred in 16.7% of the standard intervention homes
and dust mite intervention becomes a trend (P = .17). The
and 50% of the aggressive intervention homes (P = .03;
removal of patients with a positive skin test response to
Fig 1). From randomization to 12 months later, the stan-
cat and cat antigen in the home without a cat reduces the
dard intervention group had a mean 33% increase in dust
sample too drastically for meaningful analysis.
mite levels, whereas the treatment group had a mean19.6% decrease in dust level (P = .2). DISCUSSION
Levels of Fel d 1 were moderate (<8 µg/g dust) or high
(≥8 µg/g dust) in almost all homes at each visit regardless
This trial began with the hypothesis that aggressive
of cleaning regimen or the presence of a cat in the home.
environmental intervention directed at house dust mite
1072 Shapiro et al FIG 1. Changes in dust mite concentration levels by group (low, <2 µg/g; moderate, 2 to 10 µg/g; and high, ≥10
µg/g). The number of patients with household dust mite concentrations in the low, moderate, and high rangeare depicted at the baseline and 12-month collection periods. The change to a lower concentration range wassignificant for the aggressive compared with the standard intervention groups (P < .03). TABLE IV. Cat/dog antigen levels Moderate Standard Aggressive Standard Aggressive Standard Aggressive
All values are from the first home visit. SPT, Skin prick test.
elimination could have a positive effect on asthma in dust
courses; aggressive intervention group, 5 courses), this
mite–sensitive children from homes of lower-income
did not reach statistical significance.
families. The change in the primary outcome variable,
The concentrations of cat and dog antigens in these
doubling of PD20, confirmed this premise. Along with
homes were impressive. The number of homes with
this change, a decrease in dust mite antigen in home sam-
moderate and high levels of pet antigen and no resident
pet is in keeping with the findings of others.13 Cleaning
It is disappointing that home symptom diaries and
practices directed at dust mite mitigation did not signifi-
peak flows were not available. Had we built in more
cantly decrease these levels. Some of our subjects had
patient visits or phone contacts, we might have been
positive skin test responses to cat antigen and had sub-
more successful with this. However, other studies on
stantial concentrations of antigen in the home, a situation
asthma among low-income patients have had similar dif-
that could have obscured more dramatic benefits of dust
ficulties in obtaining peak flow or symptom diaries.12
mite environmental control. We cannot prove, however,
Parental reporting of overall asthma severity and quality
that cat antigen decreased the benefit of dust mite inter-
of life at 6-month visits failed to show intergroup differ-
ences. Although there were differences in the number of
The literature to support dust mite intervention for
prednisone courses (standard intervention group, 11
asthma control is extensive.14-20 Nonintervention studies
Shapiro et al 1073 FIG 2. Changes in mean PD20 before to 12 months after initiation of dust mite intervention. Mean PD20 is expressed for the standard and aggressive intervention groups at baseline and 12 months later. The standard group showed a mean increase in PD20 of 24.2%, whereas the aggressive intervention group showed a mean increase of 63.3%.
show correlations between antigen levels and clinical
or removed carpeting and upholstery with those living in
markers of disease severity.4 Custovic et al1 described a
standard bedrooms. Patients with aggressive environmen-
correlation between mite exposure, methacholine reac-
tal control had significant improvement in the
tivity, and decreased FEV1 in adults. Chan-Yeung et al2
FEV1/forced vital capacity ratio, PEFR, and bronchial
noted that dust mite–sensitive asthmatic children showed
hyperresponsiveness (histamine), but not FEV1, com-
a positive relationship of mean daily symptom score to
total mite allergen level and a negative relationship of
Our trial represents the first demonstration of the pos-
daily mean PEFR to dust mite level. Sensitization to dust
itive effect of dust mite reduction measures in a low-
mites has been associated with acute childhood asthma
income US population. It confirms previous observations
in more affluent communities of a correlation between
Australian investigators have reported that changes in
decreased dust mite concentrations and improvement in
allergen concentration in bedding were significantly cor-
bronchial hyperresponsiveness.21 In concert with other
related with bronchial hyperresponsiveness to histamine
trials, bronchial hyperresponsiveness appears to be more
and to symptom scores.16 They cited small within-patient
sensitive to change with environmental intervention than
variations in PD20 explained by antigen levels and failed,
FEV1, PEFR, or symptoms.16,17 The contribution of
as we did, to see significant changes in peak flow or
other antigens in the home and the complexity of dealing
FEV1. European investigators have documented the
with them in American homes, particularly pet antigens,
value of impermeable mattress covers combined with use
of filters in improving bronchial hyperresponsiveness.17Reduction in mite antigen correlated with a significant
REFERENCES
1. Custovic A, Taggart SCO, Francis HC, Chapman MD, Woodcock A.
Exposure to house dust mite allergens and the clinical activity of asthma.
were unchanged, as with our evaluation.
J Allergy Clin Immunol 1996;98:64-72.
These more recent studies reinforce other trials from
2. Chan-Yeung M, Manfreda J, Dimich-Ward H, Lam J, Ferguson A, War-
the last decade. Murray and Ferguson19 studied asthmatic
ren P, et al. Mite and cat allergen levels in homes and severity of asthma.
children in dust-free bedrooms that included impermeable
Am J Respir Crit Care Med 1995;152:1805-11.
covers for pillows, mattress, and box spring; no carpets;
3. Sporik R, Holgate ST, Platts-Mills TAE, Cogswell JJ. Exposure to house-
dust mite allergen (Der p 1) and the development of asthma in childhood.
and limited toys. Children living in these special rooms
A prospective study. N Engl J Med 1990;323:502-7.
compared with children living in standard bedrooms
4. Nelson RP, DiNicolo R, Fernandez-Caldas E, Seleznick MJ, Lockey RF,
showed fewer days of wheezing, fewer days requiring
Good RA. Allergen-specific IgE levels and mite allergen exposure in
medication, and fewer days with abnormal peak flow
children with acute asthma first seen in an emergency department and innonasthmatic control subjects. J Allergy Clin Immunol 1996;98:258-63.
rates. Walshaw and Evans20 evaluated adult asthmatic
5. Burrows B, Sears MR, Flannery EM, Herbison GP, Holdaway MD, Silva
subjects and compared those living in bedrooms with spe-
PA. Relation of the course of bronchial responsiveness from age 9 to age
cial bed covers, weekly laundered bedding, and cleaned
15 to allergy. Am J Respir Crit Care Med 1995;152:1302-8. 1074 Shapiro et al
6. Sparrow D, O’Connor G, Colton T, Barry CL, Weiss ST. The relationship
14. Platts-Mills TAE. Dust mite allergens and asthma—a worldwide prob-
of non-specific bronchial responsiveness to the occurrence of respiratory
lem. J Allergy Clin Immunol 1989;83:416-27.
symptoms and decreased levels of pulmonary function. The Normative
15. Platts-Mills TAE, Woodfolk JA, Chapman MD, Heymann PW. Changing
Aging Study. Am Rev Respir Dis 1987;135:1255-60.
concepts of allergic disease: the attempt to keep up with real changes in
7. Burney PGJ, Britton JR, Chinn S, Tattersfield AE, Papacosta AO, Kelson
lifestyle. J Allergy Clin Immunol 1996;98:S297-306.
MC, et al. Descriptive epidemiology of bronchial reactivity in an adult
16. Marks GB, Tovey ER, Green W, Shearer M, Salome CM, Woolcock AJ.
population: results from a community study. Thorax 1987;42:38-44.
The effect of changes in house dust mite allergen exposure on the sever-
8. Rijcken B, Schouten JP, Weiss ST, Speizer FE, van der Lende R. The
ity of asthma. Clin Exp Allergy 1995;25:114-8.
association of airways responsiveness to respiratory symptom prevalence
17. van der Heide S, Kauffman HF, Dubois AE, de Monchy JGR. Allergen
and to pulmonary function in a random population sample. Bull Eur
reduction measures in houses of allergic asthmatic patients: effects of air-
cleaners and allergen-impermeable mattress covers. Eur Respir J
9. Clifford RD, Howell JB, Radford M, Holgate ST. Associations between
respiratory symptoms, bronchial response to methacholine, and atopy in
18. Korsgaard J. Mite asthma and residency. A case-control study on the
two age groups of schoolchildren. Arch Dis Child 1989;64:1133-9.
impact of exposure to house-dust mites in dwellings. Am Rev Respir Dis
10. Guidelines for the diagnosis and management of asthma. Bethesda (MD):
National Institutes of Health; National Heart, Lung, and Blood Institute;
19. Murray AB, Ferguson AC. Dust-free bedrooms in the treatment of asth-
April 1997. NIH publication no. 97-4051.
matic children with house dust or house dust mite allergy: a controlled
11. Childhood Asthma Management Program Research Group. The Child-
hood Asthma Management Program (CAMP): design, rationale, and
20. Walshaw MJ, Evans CC. Allergen avoidance in house dust mite sensitive
methods. Control Clin Trials 1999;20:91-120.
adult asthma. Q J Med 1986;58:199-215.
12. Rosenstreich DL, Eggleston P, Kattan M, Baker D, Slavin RG, Gergen P,
21. Ehnert B, Lau-Schadendorf S, Weber A, Buettner P, Schou C, Wahn U.
et al. The role of cockroach allergy and exposure to cockroach allergen in
Reducing domestic exposure to dust mite allergen reduces bronchial
causing morbidity among inner-city children with asthma. N Engl J Med
hyperreactivity in sensitive children with asthma. J Allergy Clin Immunol
13. Bollinger ME, Eggleston PA, Flanagan E, Wood RA. Cat antigen in
homes with and without cats may induce allergic symptoms. J AllergyClin Immunol 1996;97:907-14.
Regione che vai, cura che trovi. L'accesso ai farmaci e la terapia alle prese con la regionalizzazione. Primo dossier diCittadinanzattiva-Tribunale per i diritti del malato Pazienti costretti a fingere o a cambiare Regione di residenza per accedere ad un farmaco che possa migliorare la loroqualità di vita. Non si tratta della trama di un film di fantasia, ma la triste realtà a cui sono sottopo
 1072 Shapiro et al
1072 Shapiro et al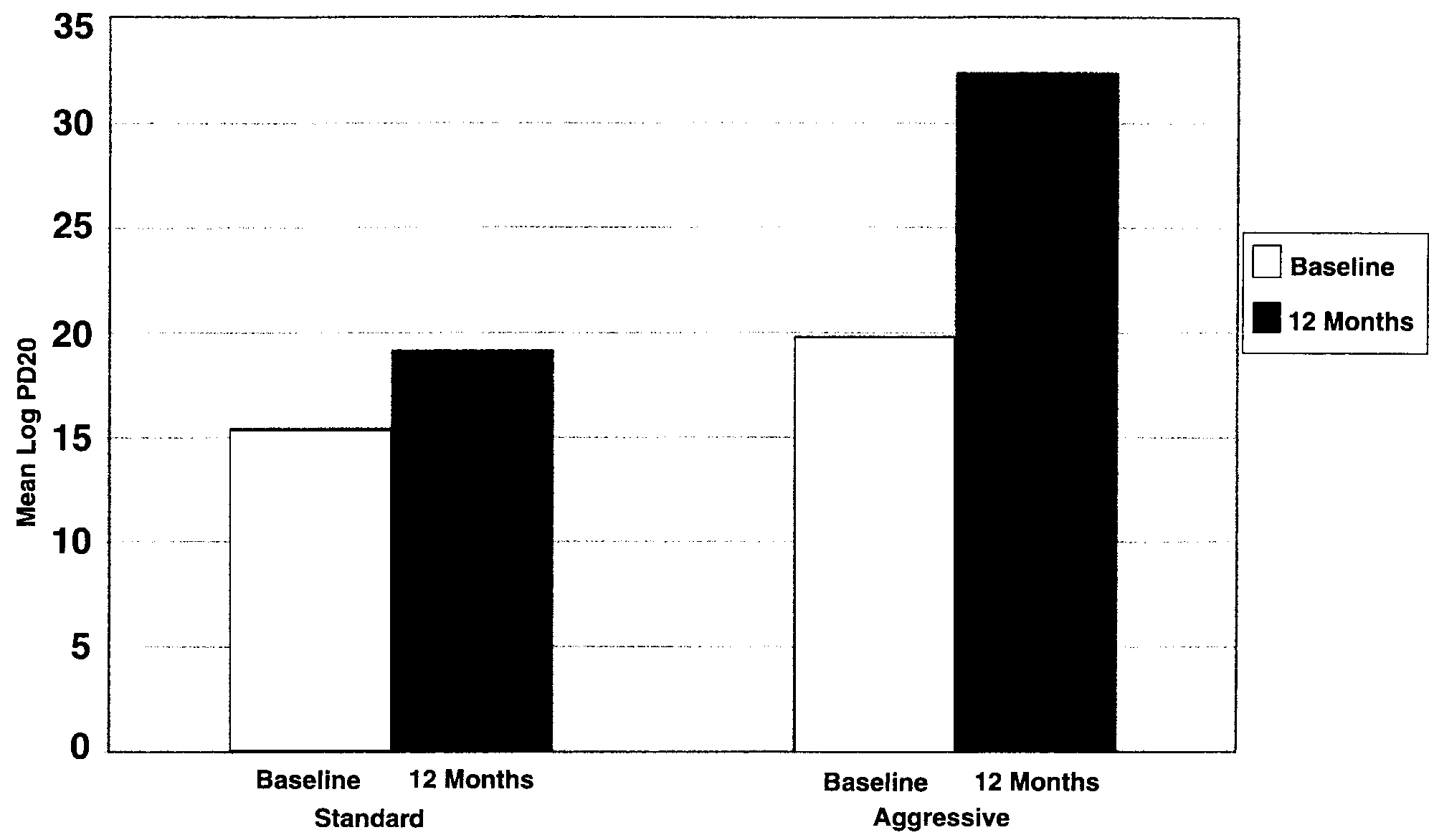 Shapiro et al 1073
Shapiro et al 1073