Advance Access publication 29 October 2011
Treatment of trigger finger: randomized clinical trialcomparing the methods of corticosteroid injection,percutaneous release and open surgery
Edson S. Sato1, Joa˜o B. Gomes dos Santos1, Joa˜o C. Belloti1,Walter M. Albertoni1 and Flavio Faloppa1
Objective. The aim of this study is to evaluate the effectiveness of CS injection, percutaneous pulleyrelease and conventional open surgery for treating trigger finger in terms of cure, relapse and complication
Methods. One hundred and thirty-seven patients with a total of 150 fingers were randomly assigned andallocated into one of the treatment groups, with treatments allocated into 150 opaque and sealed enve-lopes. We included patients >15 years of age with a trigger on any finger of the hand (Types IIIV) andused a minimum follow-up time of 6 months. The primary outcome measures were cures, relapses andfailures.
Results. Forty-nine patients were assigned to the conservative group to undergo CS injections, whereas45 and 56 were assigned to undergo percutaneous release and outpatient open surgery, respectively. Thetrigger cure rate for patients in the injection method group was 57%, and wherever necessary, twoinjections were administered, which increased the cure rate to 86%. For the percutaneous and open
release methods, remission of the trigger was achieved in all cases.
Conclusions. The percutaneous and open surgery methods displayed similar effectiveness and provedsuperior to the conservative CS method regarding the trigger cure and relapse rates.
Trial registration. Current Controlled Trials, http://www.controlled-trials.com/, ISRCTN19255926.
Key words: trigger finger disorder, tendon entrapment, stenosing tenosynovitis, trigger digits, snappingfinger, trigger thumb, randomized controlled trial, controlled clinical trial, operative surgical procedure,tendon release
identified as triggering factors, there is no consensus inthe literature about its true cause and its aetiology remains
Trigger finger is a condition that occurs when the gliding
unknown Notta described trigger finger as a con-
movement of the tendon is blocked by the osteofibrous
dition caused by changes to the flexor tendon and its
canal of the A1 pulley, preventing the tendon from natur-
sheath. Hueston and Wilson demonstrated in an ana-
ally extending and returning to its initial position. Although
tomical study that the spiral arrangement of the architec-
synovial proliferation and fibrosis flexor sheath are
ture of the intratendon fibres leads to the formation ofnodules that form distally to the A1 pulley.
This pathology is more common in women, on the dom-
Department of Orthopedics and Traumatology, Discipline of Hand
and Upper Limb Surgery, UNIFESP Federal University of Sa˜o Paulo,
inant side, and in the sixth decade of life. The most af-
Sa˜o Paulo City, Sa˜o Paulo, Brazil.
fected finger is the thumb; however, the occurrence of the
Submitted 3 June 2011; revised version accepted 5 August 2011.
trigger is also common in the other fingers The symp-
Correspondence to: Edson S. Sato, Department of Orthopedics and
toms vary from a slight local discomfort to the formation of
Traumatology, Discipline of Hand and Upper Limb Surgery, UNIFESP
a tendon blockage, experienced principally in the morn-
Federal University of Sa˜o Paulo, Sa˜o Paulo City, Sa˜o Paulo, Brazil. E-mail: edsonsasahara@ig.com.br
ing, which leads to a deficit in actively extending the
! The Author 2011. Published by Oxford University Press on behalf of the British Society for Rheumatology. All rights reserved. For Permissions, please email: journals.permissions@oup.com
finger, which remains fixed in a flexed position Trigger
they were discharged from the study. For the injection
finger also appears to be linked to other diseases, such as
group, those that received a second injection were fol-
RA, gout, CTS, De Quervain’s disease and diabetes
lowed for 6 months starting from the second intervention.
Quinnell classified the trigger finger using five typesduring flexion and extension: normal movement (Type 0),
uneven movement (Type I), actively correctable (Type II),
The patients were initially treated by outpatient hand sur-
passively correctable (Type III) and fixed deformity (Type IV).
gery in the Discipline of Hand and Upper Limb Surgery,
Although some patients may experience a spontaneous
Department of Orthopedics and Traumatology, Paulista
cure or a disappearance of the symptoms by means of the
Medical School Federal University of Sa˜o Paulo
treatment strategies of immobilization or CS injections,
(UNIFESP) Brazil. Treatment was started for a group of
many may require surgery for release of the A1 pulley
137 patients presenting 150 cases of trigger finger. The
, Some authors support a conservative treat-
patients were treated by resident physicians, assistant
ment based on steroid injection, whereas others advocate
physicians and the author of this article according to the
A CS in conjunction with anaesthesia may be adminis-
The study participants and each finger submitted to
tered to the flexor muscle sheath, and this strategy has
treatment were grouped and numbered chronologically.
been demonstrated to produce good results
In cases in which the patient presented with two trigger
However, that technique can result in a relapse rate of up
fingers, each finger received its own order number regard-
less of whether the fingers were on the same or different
Release through open surgery has a high rate of suc-
cess with minimal morbidity and recurrence, although
In the study, 12 patients had a trigger on more than one
they do occur, principally in cases of long-standing illness
finger of a hand. Each trigger finger received an order
and in which there was a failure of a conservative remedy;
number. Eleven patients participated in the study on two
however, accounts of complications do exist, such as
occasions, and one participated on three occasions.
painful scarring, infections and nerve damage, in addition
Calculation of the size of the study sample was based
on the primary outcome of the differences in cure rates
In 1958, Lorthioir described a treatment method for
among the different proposed treatment techniques, with
trigger finger consisting of a delicate tenotomy. Other au-
the sample being considered dichotomically and categor-
thors have also reported good results by using percutan-
ically variable. The difference in cure rates was originally
determined to be $25%. Each group finally consisted of
We developed this randomized prospective study with
50 fingers, after 43 were calculated per group with a
the objective of verifying the most effective treatment
b-value of 80% and an a statistical significance of 5%.
method for this pathology by comparing the techniques
For the purposes of randomization, we used a six-sided
of CS injection, percutaneous release of the A1 pulley and
die, with the treatment method selection depending on the
conventional open surgery in terms of their rates of cure,
result obtained. When sides one and six were scored, the
selected method was injection, surgical release was se-lected when sides three and four were scored and percu-
taneous release was selected when sides five and sixwere scored, resulting in three study groups. The draw
was conducted before the study by a person independent
The study compared the rates of cure, relapse and com-
of the research. There were 150 draws conducted. As the
plications of treatments for trigger finger based on CS in-
methods were drawn, each result was placed in an
jection, percutaneous release and open release of the A1
opaque envelope, which was then sealed; envelopes
pulley as realized in the period from November 2002 to
were numbered from 1 to 150. None of the project par-
March 2007. The research project was analysed and
ticipants had prior access to the envelope contents.
approved by the Ethics Research Committee of the
Before treatment, the envelope was opened and the
paper, with either one, two or three methods to be used,
(CEP No. 0349/03 on 23 May 2003). Written informed con-
was read by the assistant physician. The patient was in-
sent was obtained from all the participants.
formed of the type of treatment he or she would receive
For both genders, the inclusion criteria were 515 years
and was led to the operating theatre. In this manner, each
of age and symptomatologies of trigger finger movement
patient received treatment according to his or her number
blockage on either hand in subjects who had not under-
(e.g. the first patient received the treatment indicated
gone previous treatment of any type and were classified
as Quinnell Types II—IV We excluded individuals with
Type I trigger fingers, which are considered congenitaland secondary to the partial lesion to the tendon.
CS injection consisted of an injection of 2 ml of methyl-
Outpatient follow-up was conducted over a minimum
prednisolone acetate 40 mg/ml at the site corresponding
period of 6 months. The patients were prospectively as-
to the A1 pulley, attempting to inject the solution within the
sessed after 1, 2 weeks, 1, 2, 4 and 6 months, after which
osteofibrous canal Percutaneous release consisted
of release of the A1 pulley with a 40 Â 12 needle, using
6 months after the treatment. Complications, including
longitudinal movements, in the direction of the axis of
those linked to the treatment methods used, infection,
the flexor tendon, and this release was introduced at
total lesion of the flexor tendon and lesion of the digital
Conventional open surgery consisted of an incision of2 cm in the skin transverse to the axis of the finger at
the palmar skin fold, followed by subcutaneous dissection
Analysis of variance (ANOVA) was used to compare the
and longitudinal opening of the A1 pulley
averages of the numerical variables. For the categoricalvariables, we used the Pearson’s chi-square test. For all
tests, an a-value of 5% was used, with P < 0.05 indicating
statistical significance. All analyses were performed using
Cure of the trigger was considered as the remission of the
trigger, cessation of blockage (bending) of the finger, and
We analysed the homogeneity among participants of
the free flow of its movement. Patients were deemed
the study according to their gender, the onset of diabetes,
cured if they maintained remission of the ‘trigger’ for
age and duration of disease at the date they committed to
6 months of follow-up. Relapse of the trigger was classi-
the protocol. The Pearson’s chi-square test was used to
fied as the relapse or return of blockage of the finger
verify the existence of the link among the categorical vari-
within the 6 months of post-study follow-up. With respect
ables, gender and onset of diabetes. ANOVA was used to
to percutaneous release and open release, we classified
make comparisons among the averages of the numeric
as failures those fingers that relapsed or in which block-
variables, gender and duration of disease at the date of
age of the finger was maintained after treatment. For the
committing to the protocol. We used Pearson’s chi-
purposes of the injection, we considered as failures those
square test for the statistical analysis of the frequency of
fingers that relapsed or in which blockage of the finger
complaints regarding pain subsequent to the treatments,
was maintained after the second injection.
both at the site of the procedure as well as at the IP jointsof the digits. We used ANOVA for the statistical analysis
of the variation of movement of the fingers before and
Topical pain was defined as pain at the site of the pro-
after the treatments. Pearson’s chi-square test was used
cedure 1 and 2 weeks and 1, 2, 4 and 6 months after the
for statistical comparisons among the cure rates for the
procedure. Articular pain was defined as pain at the IP
injection, percutaneous and open methods.
joint of the thumb and at the PIP joint of the fingers 1
and 2 weeks and 1, 2, 4 and 6 months after the procedure.
For the purposes of assessing the active movement of thefingers, we used the total active motion (TAM) method as
advocated by the Committee for Tendon Lesions of the
The three groups were homogeneous in terms of age,
International Federation of Societies of Hand Surgery
comorbidity, gender, time of onset of trigger finger and
To calculate the TAM value, we added the degree of flex-
classification (and The data pertaining to
ure of the joints of the fingers with active flexure and sub-
the analysis of the rates of cure, relapse and failure
tracted the loss of extension as measured with the finger
observed among the injection, percutaneous and open
in active extension. The measurements were collected
using a goniometer in the dorsal region of the fingers. Themeasurements were taken before and 1, 2, 4 and
TABLE 1 Epidemiological data: gender, onset of diabetes,age in years and disease time in months
*Chi-square test. n: number of patients per group.
The injection group presented a rate of trigger finger
relapse of 12.5%. All relapses received a second injection.
The open and percutaneous methods resulted in signifi-
The group that received two injections presented a re-
cantly higher rates of cure of trigger finger than the injec-
lapse rate of 18%. No relapse was observed in the groups
treated by percutaneous release and open surgery.
There were seven failures in the injection method groupafter the second injection: four occurred as a result of the
TABLE 2 Distribution of patients by classification
persistence of the trigger and three occurred as a result ofrelapse. There were no failures in the percutaneous and
open surgery groups. The results of the interventions aresummarized in
The percentage of patients experiencing topical pain in
the injection group was statistically lower than those inthe percutaneous and open surgery groups after 1 week
*Chi-square test. n: number of patients per group.
(P = 0.000), 2 weeks (P = 0.000) and 1 month (P = 0.008) offollow-up. After 2, 4, and 6 months of follow-up, the per-centage of patients experiencing topical pain was similar
TABLE 3 Distribution of results with grouping by method:
The percentage of patients complaining of articular pain in
the injection group was statistically lower than those in the
percutaneous and open surgery groups after 1 week(P = 0.014), 2 weeks (P = 0.023) and 1 month (P = 0.029)
of follow-up. After 2, 4 and 6 months of follow-up, the
percentage of patients complaining about pain was similar
There was no difference in the TAM values among the
injection, percutaneous release and open surgery groups
in the pre-treatment period and 6 months after treatment.
FIG. 2 Flowchart of the intervention results.
TABLE 4 Distribution of topical and joint pain frequency
TABLE 5 Distribution of the average measurements
of movement of the fingers by active movement
(TAM values) by method before and 1, 2, 4 and6 months after treatment
*ANOVA. **Statistically significant (P < 0.05). Before: TAM
indicated for Type I due to the need for active demonstra-
tion of the flexionextension activity of the finger for that
procedure. With Type I, the trigger occurs sporadically at
the time of surgery and a blockage may not occur, which
would give an erroneous impression of remission.
The open and percutaneous surgery methods proved
similar and superior to injection in terms of cure and re-lapse rates. In the injection group, a 57% cure rate of the
trigger was achieved with CS injection. The cases of fail-
ure of relapse were submitted to a second injection; in thismanner, the cure rate increased to 86% over a 6-monthfollow-up period. A third injection was not offered, and
No differences were observed after 1, 2 and 4 months of
the relapses were considered failures, which were then
follow-up between the injection and percutaneous release
treated by means of open or percutaneous release. The
groups. Lower values were observed in the open surgery
results for those patients were computed in the initially
group than in the injection and percutaneous release
randomized group, in line with the principle of intent of
groups after 1 (P = 0.012), 2 (P = 0.048) and 4 months
treatment. Of the cases in which there were failures in
the remission of the trigger, six were initially classified asType II, and one was classified as Type III. We did not find
any studies related to the percentage of cure by injection
We did not record any complications such as infection
in conjunction with the type of trigger in the literature. The
and total lesion of the flexor tendon or digital nerve
patients in the percutaneous and open release groups had
among the three groups receiving CS injections, percu-
remission rates of 100%, similar to the results presented
taneous release or conventional open surgery.
by Gilberts et al. in a randomized prospective studycomparing the percutaneous method with the open
method, in which they reported remission rates of 98%with the open surgery method and 100% with the percu-
The treatment approach to trigger finger can be conser-
vative, such as the method of CS injection, or can be
The patients in the injection group experienced a lower
surgical, such as open surgical and percutaneous release
incidence of pain in the first month of follow-up compared
methods. Conclusive evidence regarding the best treat-
with those of the open and percutaneous groups, which
ment option is lacking. We consequently developed this
had similar incidences. Authors such as Chao et al.
randomized-format study based on a homogeneous popu-
compared the percutaneous and injection methods and
lation to test the effectiveness of the three methods.
reported that the group given injections also presented a
We included patients >15 years of age with a trigger on
lower incidence of patients with pain in the first month
any finger, although authors such as Bain et al. [have
after the procedure than patients submitted to percutan-
indicated that a greater risk of lesion to the neurovascular
sheath exists with the percutaneous release of the thumb
For all three groups, TAM values in the sixth month of
and small finger. With respect to the stage of disease,
follow-up were greater than the values observed before
we included Types IIIV triggers because in a previous
treatment, similar to the findings of Marcus et al. [The
study we observed that the percutaneous method is not
open group had lower TAM values than the injection and
percutaneous groups after 1, 2 and 4 months of follow-up,
10 Rhoades CE, Gelberman RH, Manjarris JF. Stenosing
which may be explained by the greater morbidity of the
tenosynovitis of the fingers and thumb. Clin Orthop Relat
We did not observe any lesion of the digital nerve
11 Marks MR, Gunther SF. Efficacy of cortisone injection in
among the three treatment groups, which would be a dis-
treatment of trigger fingers and thumbs. J Hand Surg Am
tressing factor, principally for the percutaneous method
group. We believe that the demarcation of the longitudinal
12 Newport ML, Lane LB, Stuchin SA. Treatment of trigger
axis of the tendon in the percutaneous technique and pre-
finger by steroid injection. J Hand Surg Am 1990;15:
cise anatomical knowledge of the pulleys are important
factors for preventing complications, which is similar to
13 Benson LS, Ptaszek AJ. Injection versus surgery in the
the conclusion reached in anatomical studies
treatment of trigger finger. J Hand Surg Am 1997;22:13844.
14 Ring D, Lozano-Caldero´n S, Shin R et al. A prospective
randomized controlled trial of injection of dexamethasone
The levels of effectiveness of open surgical and percutan-
versus triamcinolone for idiopathic trigger finger. J Hand
eous methods were superior to the conservative method
of using CSs based on the cure and reappearance rates of
15 Turowski GA, Zdankiewicz PD, Thomson JG. The results
of surgical treatment of trigger finger. J Hand Surg Br1997;22:1459.
16 Thorpe AP. Results of surgery for trigger finger. J Hand
. Trigger finger should be treated first by steroid
17 Lorthioir J. Surgical treatment of trigger-finger by a
subcutaneous method. J Bone Joint Surg Am 1958;40:
. Trigger finger treatment by percutaneous pulley
release and open surgery showed similar levels ofpain.
18 Tanaka J, Muraji M, Negoro H et al. Subcutaneous release
. Steroid injection is a less painful method than
of trigger thumb and fingers in 210 fingers. J Hand Surg Br
surgery for treating trigger finger.
19 Lyu SR. Closed division of the flexor tendon sheath for
trigger finger. J Bone Joint Surg Br 1992;74:41820.
Disclosure statement: The authors have declared no
20 Cohen TJ. Percutaneous treatment of trigger finger. Rev
21 Nagoshi M, Hashizume H, Nishida K et al. Percutaneous
release for trigger finger in idiopathic and hemodialysis
patients. Acta Med Okayama 1997;51:1558.
Quinnell RC. Conservative management of trigger finger.
of trigger finger. Acta Orthop Scand 1998;69:1678.
Notta A. Research on a particular condition of tendon
23 Blumberg N, Arbel R, Dekel S. Percutaneous release of
sheaths of the hand, characterized by the development of
trigger digits. J Hand Surg Br 2001;26:2567.
a nodule in the path of flexor tendons and blocking their
24 Ragoowansi R, Acornley A, Khoo CT. Percutaneous trig-
movements. Arch Ge´n Med 1850;24:14261.
ger finger release: the ‘lift-cut’ technique. Br J Plast Surg
Hueston JT, Wilson WF. The aetiology of trigger finger.
25 Wang HC, Lin GT. Retrospective study of open versus
Weilby A. Trigger finger. Incidence in children and adults
percutaneous trigger thumb in children. Plast Reconstr
and the possibility of a predisposition in certain age
groups. Acta Orthop Scand 1970;41:41927.
26 Fu YC, Huang PJ, Tien YC et al. Revision of incompletely
Eastwood DM, Gupta KJ, Johnson DP. Percutaneous
released trigger fingers by percutaneous release: results
release of the trigger finger: an office procedure. J Hand
and complications. J Hand Surg Am 2006;31:128891.
27 Sato ES, Albertoni WM, Leite VM et al. Trigger finger: a
Freiberg A, Mulholland RS, Levine R. Nonoperative treat-
prospective analysis of 76 fingers treated surgically by
ment of trigger fingers and thumbs. J Hand Surg Am 1989;
percutaneous release. Rev Bras Ortop 2004;396:30922.
28 Kleinert HE, Verdan C. Report of the Committee
Ryzewicz M, Wolf JM. Trigger digits: principles,
on Tendon Injuries (International Federation of Societies
management, and complications. J Hand Surg Am 2006;
for Surgery of the Hand). J Hand Surg Am 1983;8:7948.
29 Bain GI, Turnbull J, Charles MN et al. Percutaneous A1
Patel MR, Bassini L. Trigger fingers and thumb: when to
pulley release: a cadaveric study. J Hand Surg Am 1995;
splint, inject, or operate. J.Hand Surg Am 1992;17:1103.
Kolind-Sorensen V. Treatment of trigger fingers. Acta
30 Gilberts EC, Beekman WH, Stevens HJ et al.
Prospective randomized trial of open versus percutaneous
surgery for trigger digits. J Hand Surg Am 2001;26:
33 Wilhelmi BJ, Mowlavi A, Neumeister MW et al. Safe
treatment of trigger finger with longitudinal and transverse
31 Chao M, Wu S, Yan T. The effect of miniscalpel-needle
landmarks: an anatomic study of the border fingers for
versus steroid injection for trigger thumb release. J Hand
percutaneous release. Plast Reconstr Surg 2003;112:
32 Marcus AM, Culver JE Jr, Hunt TR 3rd. Treating trigger
34 Fiorini HJ, Santos JB, Hirakawa CK et al. Anatomical
finger in diabetics using excision of the ulnar slip of the
study of the A1 pulley: length and location by means of
flexor digitorum superficialis with or without A1 pulley
cutaneous landmarks on the palmar surface. J Hand Surg
Efavirenz Marca comercial: Clase de medicamento: Inhibidor de la transcriptasa inversa no análogo El efavirenz, conocido también como EFV o Sustiva, es un tipo de antirretroviral llamado inhibidor de latranscriptasa inversa no análogo de los nucleósidos (NNRTI). Esta clase de medicamentos bloquea latranscriptasa inversa, una proteína que necesita el VIH para multiplicarse.
Kurt W. Rathjen, M. D. Patient Registration Form PATIENT INFORMATION Patient’s Name:________________________________________________________ Sex: M F Marital Status:_________________ SS#____________________________________ DOB__________________________________ Age____________________________Home Address:____________________________________________________________________________
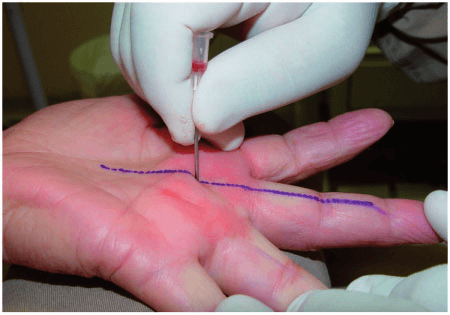 of release of the A1 pulley with a 40 Â 12 needle, using
6 months after the treatment. Complications, including
longitudinal movements, in the direction of the axis of
those linked to the treatment methods used, infection,
the flexor tendon, and this release was introduced at
total lesion of the flexor tendon and lesion of the digital
Conventional open surgery consisted of an incision of2 cm in the skin transverse to the axis of the finger at
the palmar skin fold, followed by subcutaneous dissection
Analysis of variance (ANOVA) was used to compare the
and longitudinal opening of the A1 pulley
averages of the numerical variables. For the categoricalvariables, we used the Pearson’s chi-square test. For all
tests, an a-value of 5% was used, with P < 0.05 indicating
statistical significance. All analyses were performed using
Cure of the trigger was considered as the remission of the
trigger, cessation of blockage (bending) of the finger, and
We analysed the homogeneity among participants of
the free flow of its movement. Patients were deemed
the study according to their gender, the onset of diabetes,
cured if they maintained remission of the ‘trigger’ for
age and duration of disease at the date they committed to
6 months of follow-up. Relapse of the trigger was classi-
the protocol. The Pearson’s chi-square test was used to
fied as the relapse or return of blockage of the finger
verify the existence of the link among the categorical vari-
within the 6 months of post-study follow-up. With respect
ables, gender and onset of diabetes. ANOVA was used to
to percutaneous release and open release, we classified
make comparisons among the averages of the numeric
as failures those fingers that relapsed or in which block-
variables, gender and duration of disease at the date of
age of the finger was maintained after treatment. For the
committing to the protocol. We used Pearson’s chi-
purposes of the injection, we considered as failures those
square test for the statistical analysis of the frequency of
fingers that relapsed or in which blockage of the finger
complaints regarding pain subsequent to the treatments,
was maintained after the second injection.
of release of the A1 pulley with a 40 Â 12 needle, using
6 months after the treatment. Complications, including
longitudinal movements, in the direction of the axis of
those linked to the treatment methods used, infection,
the flexor tendon, and this release was introduced at
total lesion of the flexor tendon and lesion of the digital
Conventional open surgery consisted of an incision of2 cm in the skin transverse to the axis of the finger at
the palmar skin fold, followed by subcutaneous dissection
Analysis of variance (ANOVA) was used to compare the
and longitudinal opening of the A1 pulley
averages of the numerical variables. For the categoricalvariables, we used the Pearson’s chi-square test. For all
tests, an a-value of 5% was used, with P < 0.05 indicating
statistical significance. All analyses were performed using
Cure of the trigger was considered as the remission of the
trigger, cessation of blockage (bending) of the finger, and
We analysed the homogeneity among participants of
the free flow of its movement. Patients were deemed
the study according to their gender, the onset of diabetes,
cured if they maintained remission of the ‘trigger’ for
age and duration of disease at the date they committed to
6 months of follow-up. Relapse of the trigger was classi-
the protocol. The Pearson’s chi-square test was used to
fied as the relapse or return of blockage of the finger
verify the existence of the link among the categorical vari-
within the 6 months of post-study follow-up. With respect
ables, gender and onset of diabetes. ANOVA was used to
to percutaneous release and open release, we classified
make comparisons among the averages of the numeric
as failures those fingers that relapsed or in which block-
variables, gender and duration of disease at the date of
age of the finger was maintained after treatment. For the
committing to the protocol. We used Pearson’s chi-
purposes of the injection, we considered as failures those
square test for the statistical analysis of the frequency of
fingers that relapsed or in which blockage of the finger
complaints regarding pain subsequent to the treatments,
was maintained after the second injection.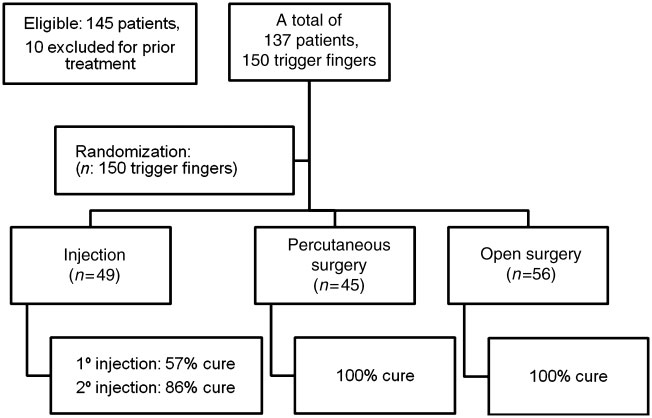 The injection group presented a rate of trigger finger
relapse of 12.5%. All relapses received a second injection.
The injection group presented a rate of trigger finger
relapse of 12.5%. All relapses received a second injection.