European Journal of Cardio-thoracic Surgery 16 (1999) 469±470
Overdose of tetracycline for pleurodesis leading to chemical burns
H. Chaugle*, C. Parchment, D.J.M. Keenan, G.J. GroÈtte
Department of Cardiothoracic Surgery, Manchester Heart Centre, Manchester Royal In®rmary, Oxford Road, Manchester M13 9WL, UK
Received 27 January 1999; received in revised form 12 July 1999; accepted 4 August 1999
Chemical pleurodesis using tetracycline is an accepted and commonly employed treatment of pneumothorax and pleural effusions. We
describe a case of chemical burn of the pleura in a ventilated 41-year-old who came to thoracotomy after 3 days of continuous intrapleural
infusion of tetracycline at another hospital. To our knowledge this has not been previously reported although other adverse effects of this
procedure are documented. We suggest that damage to the pleura and underlying lung may occur if excessive amounts of tetracycline are
used in attempted pleurodesis. q 1999 Published by Elsevier Science B.V. All rights reserved. Keywords: Tetracycline; Pleurodesis
chlocitromazine and dothiepin complicated by a right basal
aspiration pneumonia, which progressed to ARDS. He was
Pleurodesis is the obliteration of the pleural space and is
ventilated on admission and 15 days later developed a right
used to prevent the recurrence of pneumothorax,
tension pneumothorax while in the ITU of another hospital.
haemothorax, pleural effusion or chylothorax. It may
Two chest drains were inserted but there was a persistent air
occur spontaneously after in¯ammation or be induced by
leak for 12 days. An intrapleural tetracycline pleurodesis
the insertion of a chest drain, but if not, an irritant may be
was attempted via an intrapleural catheter. An infusion of
instilled into the pleural space. Chemical pleurodesis is a
1 g tetracycline in 50 ml of normal saline was commenced
common procedure not only during thoracoscopy but also
and continued at the rate of 5 ml/h after a bolus of 20 ml.
on general wards and intensive care units. The advantages
This was continued for 3 days leading to a total dose of
and disadvantages of a range of sclerosing agents such as
approximately 7 g tetracycline. Pleurodesis was not success-
talc, tetracycline and its derivatives, anti-neoplastic agents
ful and the catheter was removed. The patient was trans-
and immunomodulating agents have been debated [1]. The
ferred to our hospital for further management.
antibiotic tetracycline is commonly used and has been
Since the patient had persistent massive air leak it was
recognised as a pleural sclerosant for over a decade [2]. It
decided to perform thoracotomy and tackle the source of air
is easily available, cheap and has been shown to be fairly
leak. At surgery a large black eschar measuring about 8 £ 10
effective [3]. Some adverse effects of tetracycline pleurod-
cm was found on the right parietal and visceral pleura (Fig.
esis have already been reported and we present another
1). The tissue appeared burned and charred, and was loca-
complication that was not found in a review of the literature.
lised to one congruent area around the site where the intra-
pleural catheter had been inserted. No other area of the
pleura was similarly affected. There was a massive air
leak from the charred lung surface. A right pleurectomy
and lung biopsy was performed. The histopathology of the
A 41-year-old male intensive therapy unit (ITU) patient
pleura showed that the largest area of blackened tissue was 8
was referred to our unit with a persistent air leak. He had
cm in diameter and consisted of a super®cial layer of necro-
originally been admitted 4 weeks earlier with an overdose of
tic material with discoloration, with underlying granulation
tissue and ®brosis suggestive of `chemical burn of the
* Corresponding author. Tel.: 144-161-276-8521; fax: 144-161-276-
pleura'. The lung biopsy showed similar changes with
new interstitial ®brosis and granulation tissue.
E-mail address: hchaugle@hotmail.com (H. Chaugle)
1010-7940/99/$ - see front matter q 1999 Published by Elsevier Science B.V. All rights reserved.
H. Chaugle et al. / European Journal of Cardio-thoracic Surgery 16 (1999) 469±470
renal function, may be affected [6]. Indeed, a case of
acute renal failure associated with tetracycline pleurodesis
was reported in 1993 [7]. Local problems are rare but pyop-
neumothorax with bronchopleural ®stula has been reported
following tetracycline pleurodesis in a patient on CAPD [8].
The very effectiveness of tetracycline as a sclerosant
depends to some extent on the exciting an in¯ammatory
reaction in two pleural surfaces, and as such some damage
to the tissues is to be expected. The pathophysiology
includes stimulation of ®broblast proliferation, mesothelial
sloughing, pleural ¯uid clotting, inhibition of ®brinolysis
and resultant ®brosis [9]. However we were surprised to
see the extent of charring tissue damage caused by the
attempted pleurodesis in this case. Contributing factors
seem to be the lack of dispersal of the tetracycline, the
length of time the intrapleural instillation had been contin-
ued for and the total dose of tetracycline. The sahn protocol
modi®ed by Guzman et al. suggests one dose of 20±30 mg/
kg of tetracycline powder in 50 ml of saline instilled into the
pleural cavity after intrapleural administration of 300 mg
lidocaine. In their protocol the tube is clamped for 2 h and
the patient is repositioned frequently [8]. The total dose
given to our patient was several times larger than this, and
there may have been problem with regular repositioning of a
There appears to be some variation in the protocols used
for chemical pleurodesis. In view of the complications
previously reported, an the extent of the tissue damage we
observed in our patient, we conclude that caution should be
employed in the use of tetracycline intrapleurally and that
Fig. 1. Right parietal pleura removed from patient after 3 days of contin-
uous intrapleural administration of tetracycline showing charred eschar.
large or repeated doses should be avoided.
We would like to thank Dr Isabelle Hanson and the Histo-
Thesurgicalpleurodesiswas successfulandthe patient was
pathology Department at Manchester Royal In®rmary for
eventually extubated, rehabilitated and discharged home.
permission to reproduce photographs and section of the
There has been some debate in the literature as to which is
[1] Light RW, Vargas FS. Pleural sclerosis for the treatment of pneu-
the safest and most ef®cient agent to use for chemical pleur-
mothorax and pleural effusion. Lung 1997;75(4):213±222.
odesis. Acute respiratory failure is a rare but signi®cant side
[2] Olsen PS, Anderson HO. Long term results after tetracycline pleurod-
effect of talc pleurodesis [4]. Anti-neoplastic such as bleo-
esis in spontaneous pneumothorax. Ann Thorac Surg Jun;
mycin may be used for malignant pleural effusions but have
not been evaluated for pneumothorax. Immunomodulating
[3] Stephenson LW. Treatment of pneumothorax with intrapleural tetra-
agents such as C. parvum and OK-432 are more expensive
[4] Milanez JRC, Werebe EC, Light RW. Respiratory failure due to insuf-
and dif®cult to obtain than antibiotics or talc. Thus tetracy-
¯ated talc. Lancet 1997;349:251±252.
cline and derivative such as doxycycline have been recom-
[5] Herrington JD, Gora-Harper ML, Salley RK. Chemical pleurodesis
with doxycycline 1 g. Pharmacotherapy Mar 1996;16(2):208±285.
Despite this there have been several adverse effects asso-
[6] Wooten SA, Barbarash RA, Strange C, Sahn SA. Systemic absorption
of tetracycline and lidocaine following intrapleural instillation. Chest
ciated with tetracycline pleurodesis. Pain and fever are
commonly noted side effects but are also seen when other
[7] Smythe WR, Bavaria JE. Tetracycline pleurodesis associated acute
chemical sclerosant are used. Perhaps more signi®cantly
renal failure. Chest Oct 1993;104(4):1274±1276.
one study claims that a single dose of 20 mg/kg of intra-
[8] Abraham G, Cherian JH, Gopalakrishnan TJ. Pyopneumothorax with
pleural tetracycline administration leads to therapeutic
bronchopleural ®stula following tetracycline pleurodesis in a patient on
CAPD. Perit Dial Int 1992;12(3):237±238.
serum levels in four out of ®ve patients and warns that
[9] Guzman C, Quijada C. Tetracycline pleurodesis. Chest Mar
those with sensitivity to the antibiotic, in compromised
Der Gemeinderat orientiert Keine Gemeindeversammlung am 14. April 2010 Die vorsorglich auf den 14. April 2010 terminierte Gemeindeversammlung findet nicht statt. Es liegen keine behandlungsreife Geschäfte zur Beratung vor. Rücktritt von Marianne Maag als Gemeindeammann und Betreibungsbeamtin per 1. April 2010 Der Gemeinderat hat von der vorzeitigen Entlassung von Marianne Maag
Jamie’s Healing www.healingautism.com As seen in Jamie’s Healing By Krista Vance In the first year of their life, Jack and Jamie were beautiful and growing perfect. Jamie was walking, had wonderful words, and was very agile and coordinated. However, after a traumatic illness, Jamie slipped away from us, falling into a place called Autism. This is the story of how we got
 European Journal of Cardio-thoracic Surgery 16 (1999) 469±470
Overdose of tetracycline for pleurodesis leading to chemical burns
H. Chaugle*, C. Parchment, D.J.M. Keenan, G.J. GroÈtte
Department of Cardiothoracic Surgery, Manchester Heart Centre, Manchester Royal In®rmary, Oxford Road, Manchester M13 9WL, UK
Received 27 January 1999; received in revised form 12 July 1999; accepted 4 August 1999
Chemical pleurodesis using tetracycline is an accepted and commonly employed treatment of pneumothorax and pleural effusions. We
describe a case of chemical burn of the pleura in a ventilated 41-year-old who came to thoracotomy after 3 days of continuous intrapleural
infusion of tetracycline at another hospital. To our knowledge this has not been previously reported although other adverse effects of this
procedure are documented. We suggest that damage to the pleura and underlying lung may occur if excessive amounts of tetracycline are
used in attempted pleurodesis. q 1999 Published by Elsevier Science B.V. All rights reserved.
European Journal of Cardio-thoracic Surgery 16 (1999) 469±470
Overdose of tetracycline for pleurodesis leading to chemical burns
H. Chaugle*, C. Parchment, D.J.M. Keenan, G.J. GroÈtte
Department of Cardiothoracic Surgery, Manchester Heart Centre, Manchester Royal In®rmary, Oxford Road, Manchester M13 9WL, UK
Received 27 January 1999; received in revised form 12 July 1999; accepted 4 August 1999
Chemical pleurodesis using tetracycline is an accepted and commonly employed treatment of pneumothorax and pleural effusions. We
describe a case of chemical burn of the pleura in a ventilated 41-year-old who came to thoracotomy after 3 days of continuous intrapleural
infusion of tetracycline at another hospital. To our knowledge this has not been previously reported although other adverse effects of this
procedure are documented. We suggest that damage to the pleura and underlying lung may occur if excessive amounts of tetracycline are
used in attempted pleurodesis. q 1999 Published by Elsevier Science B.V. All rights reserved.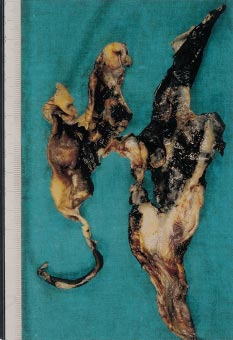 H. Chaugle et al. / European Journal of Cardio-thoracic Surgery 16 (1999) 469±470
renal function, may be affected [6]. Indeed, a case of
acute renal failure associated with tetracycline pleurodesis
was reported in 1993 [7]. Local problems are rare but pyop-
neumothorax with bronchopleural ®stula has been reported
following tetracycline pleurodesis in a patient on CAPD [8].
H. Chaugle et al. / European Journal of Cardio-thoracic Surgery 16 (1999) 469±470
renal function, may be affected [6]. Indeed, a case of
acute renal failure associated with tetracycline pleurodesis
was reported in 1993 [7]. Local problems are rare but pyop-
neumothorax with bronchopleural ®stula has been reported
following tetracycline pleurodesis in a patient on CAPD [8].