Gamma Knife Surgery for Essential Trigeminal Neuralgia: New Treatment Strategy with Robotized Micro-Radiosurgery M. Hayashi1,2,3, T. Ochiai1,3, M. Chernov1, K. Nakaya1, M. Izawa1, T. Hori 1 and K. Takakura1, 2 1Department of Neurosurgery, Neurological Institute, Tokyo Women’s MedicalUniversity, Tokyo, Japan; 2Graduate school of Medicine, Institute of AdvancedBiomedical Technology & Science, Tokyo Women’s Medical University, Tokyo,Japan; 3Saitama Gamma Knife Center, Sanai hospital, Saitama, JapanAbstract
Gamma knife surgery (GKS) is a minimally invasive treatment for brain
diseases, and is currently used for functional disorders. Moreover, a revisedversion of Gamma knife system, “Model C-APS (automatic positioningsystem)” started to be installed in Japan since 2001. This latest model ena-bles us to adjust coordinates by every 0.1 mm, and treat the patient auto-matically.
We have completed a retrospective study of 200 patients suffering from
essential trigeminal neuralgia (TGN) treated with GKS in which the targetwas localized at the retro-gasserian portion of the nerve (We have treated157 patients with essential TGN by “Model C-APS”). Among the patients,106 could be followed up more than 6 months, and we evaluated a cause-and-effect relationship between the technical development and the clinicalresults. We categorized patients into three groups based on the term men-tioned as follows; 1st are the patients treated by Model B without completedfusion images (CFI) in between 1999 and 2001, 2nd are the patients treatedby Model B with CFI in 2002, and 3rd are those treated by model C-APSwith CFI since 2003. Clinical result, initial pain free was observed in 62.9%(1st group), 85.7 % (2nd group), 99.1% (3rd group), complete recurrencewas observed in 12%, 8.3 %, 0 % for each groups, and postoperative com-plication was observed in 14.8%, 14.3%, and 9.5% respectively. We believethat precise dose planning, so-called “Robotized Micoro Radiosurgery”, is
F614C0614 231 14th Meeting of the World Society for Stereotactic and Functional Neurosurgery
the key to have a successful gamma knife surgery. Key Words: Gamma knife, radiosuregry, trigeminal neuralgia, APS
Introduction
Gamma knife surgery (GKS) has become one of the most advanced neu-
rosurgical treatments available. It is well known to be a minimally invasivesurgical procedure that can control tumor growth, and moreover, it is effi-cacious and safe for control of functional disorders without craniotomy.
Recently, we have focused on the management of intractable pain, par-
ticularly trigeminal neuralgia (TGN) that has become a functional diseasecommonly treated by GKS worldwide. Many clinical reports have demon-strated that GKS can provide satisfactory results for patients without seri-ous complications. In this chapter, we will present our institutional experi-ence of GKS treatment for TGN. Treatment options for TGN in general
In treating patients with TGN, we normally administer carbamazepine.
When the effect is insufficient, we must consider surgical procedures suchas glycerol rhizotomy, thermocoagulation, micro balloon compression, andmicrovascular decompression. The initial pain free rate is reportedly 74 to94 % and the recurrence rate 16 to 45 % 1) 2) 3). Recently, GKS has been re-garded as an alternative treatment for TGN. For the elderly patients in whomsurgery has failed and who suffer from possible risks associated with gen-eral anesthesia, GKS (the least invasive treatment) is particularly recom-mended. Treatment Concept for TGN in GKS
In GKS for TGN, we normally use only 1 isocenter with a 4 mm colli-
mator, and place it at the trigeminal nerve on the affected side. There aretwo different means of nerve target positioning. One target is exclusivelythe root entry zone (REZ), which is 2-4 mm from the emergence of the brainstem and the neuroanatomical border between oligodendrocytes and schwancells. This strategy is favored by the Pittsburgh group. Another target is theretro gasserian region (RGR), which is located at the trigeminal incisula. Thisis the approach of the Marseille group. At our institute, we’ve employed theRGR method for two main reasons;1) Efficacy and safety: The RGR target is adequately far from the brain
stem for an optimal dose (90Gy at maximum) to the nerve. To date,we have achieved greater effectiveness while avoiding damage tothe brain stem that could occur with high dose irradiation.
2) Efficacy and accuracy: we can correct the MRI distortion precisely
by using CT/MRI fusion images, because RGR targeting requires abone landmark; the trigeminal incisula at the top of the petrousbone. On the contrary, it is impossible to directly correct MRI dis-tortion with REZ targeting. Patient eligibility
In the field of functional radiosurgery, appropriate patient selection is
critical. TGN should be regarded as apparent TGN, to be confirmed clini-cally. Table 1 presents the features of six subjects with a tentative diagno-sis of TGN. Before concluding that GKS can be done, all subjects must befully informed. Our treatment aim is to prevent or reduce “electric discharge”. GKS procedure for TGN
With frame fixation of the head, the frame must be placed parallel to the
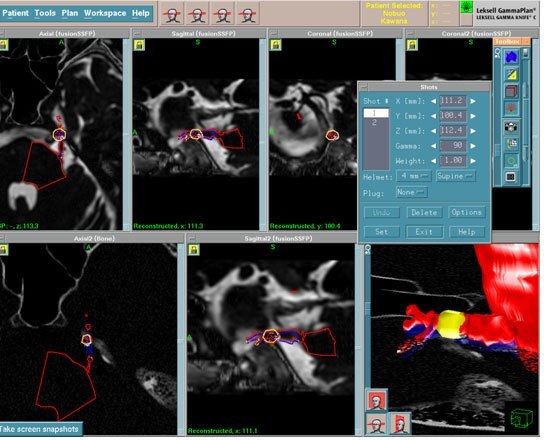
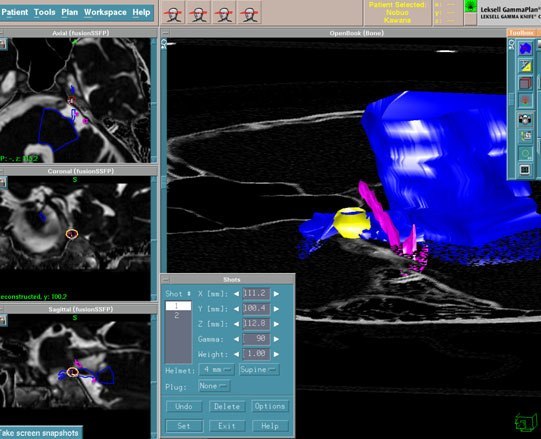
trigeminal nerve. Anatomical information regarding the nerve should alsobe confirmed. Next, we consider MRI sequence selection. Our aim is goodvisualization of the nerve in the cerebello-pontine cistern. Therefore, wenormally use ultra-thin sliced (0.5mm) 3D heavily T2 WI and thin sliced(1.0mm) axial CT bone images. Before dose planning, we obtain MRI/CTfusion images. We use RGR targeting, and an irradiation dose of 90Gy, atmaximum, considering the cerebello-pontine cistern space. If the cistern isnarrow, however, we use a beam plugging technique to modify the 20%isodose line (18Gy area), making it parallel to the surface of the brain stem,thus avoiding excessive radiation of the brain stem. We assess the existenceof MRI distortion using the MRI/CT fusion images and if any is detected,the amount of distortion is calculated precisely. After confirming the degreeof distortion between CT and MRI images, we can correctly and preciselyadjust it using an APS (automatic positioning system) by 0.1 mm level (Fig1). The most important aspect of TGN is radiosurgery that delivers suffi-cient energy to the nerve with the smallest possible collimator. This meansthat the isocenter should fall precisely on the center of the true trigeminalnerve. We can achieve this precision by using 3D images (Fig 2) in the fi-nal stage of dose planning. Efficacy and Clinical Outcome
We have treated one hundred and one patients with TGN (including two
underwent second GKS) by gamma knife using RGR targeting. Among them,147 followed up for more than 6 months were clinically evaluated. Initialpain reduction was observed in 98.6% (145/147), complete relief of “elec-tric discharge” was observed in 91.1% (134/147). Delay of significant ef-fects were ranged from 1 to 90 (mean 26.4) days. True recurrence was ob-
14th Meeting of the World Society for Stereotactic and Functional NeurosurgeryFig. 1 demonstrates 2D image and Fig3 shows 3D image. Both figures display theanatomical relationships including the trigeminal nerve and surrounding vital struc-tures. The artery obviously conflicts the trigeminal nerve located on trigeminal incisula,and the never is properly covered by the 50% isodose area of 4mm isocenter.Fig. 1, 2: Irradiation planning for trigeminal neuralgia (GammaPlan)
served in 3.0% (4/134). Delayed recurrence was detected at 6-24 months(mean 9 months). Postoperative complications (hypoesthesia and dysesthesia)developed in 10.9%(16/147), but there were no mortalities. In those whoreceived GKS only once, this rate was 9.5% (14/147). We also investigatedclinical outcome according to the following treatment factors:1) First generation group (1998-2001): treatment using model B with-
out completely fusion images: 29 cases (27 cases with follow-up)
2) Second generation group (2002): treatment using model B with com-
pletely fusion images: 14 cases (all with follow-up)
3) Third generation group (2003-2004): treatment using model C-APS
with completely fusion images: 157 cases (106 cases with follow-up)
Initial significant pain reduction was observed in 92.6% (25/27) of the
first group, 100% of the second (14/14) and the third (106/106). The respectivepain free (= complete relief of electric discharge) rate was 63% (17/27), 85.7%(12/14), and 99.1% (105/106). Those with true recurrence were 12% (3/25),8.3% (1/12) and 0% (0/105). Postoperative complication rates were 14.8%(4/27), 14.3% (2/14) and 9.5% (10/105). Both third group cases that developedpostoperative dysesthesia underwent GKS twice. Although the follow-upof the third group is yet insufficient, the results are clearly the best amongthe three.
At our institution, no significant predictive parameter has been identi-
fied from our clinical results, age, gender, affected side, topology,carbamazepine dose, delay of onset, previous intervention, cistern space,nerve atrophy, etc. Discussion
TGN is the most common functional disease that can be controlled well
by GKS. This has already been established as single isocenter irradiationwith a 4mm collimator. However, clinical outcomes differ markedly fromone institution to another.
Regis et al 3) (Marseille group) reported the clinical outcomes of 110
patients with RGR targeting in their prospective study. The initial pain freerate was observed in 97.2% (104/107), and delay of effects was seen at 26.2days on average (1day-6months). True recurrence was observed in 14.4%(15/104), postoperative complications in 4.5% (5/107). On the other hand,Kondziolka et al 4) 5) (Pittsburgh group) reported their clinical experience with220 patients in whom the initial pain free rate was 70.3%, that of true re-currence 13.6%, and postoperative complications were seen in 10.2%.
Fukuoka 6) evaluated treatment data (1145 cases) and clinical outcomes
from multiple Japanese facilities and found that targeting position varies
14th Meeting of the World Society for Stereotactic and Functional Neurosurgery
among institutions. REZ targeting was more widely used in Japan (69.4%)than RGR targeting (20.4%). MRI/CT fusion images were not used in allinstitutions. Significant pain reduction was observed in 85% (973/1145) ofcases, approximately 70% (800/1145) of whom had initial pain relief, andthe delay of effect was 30 days on average (1-120 days). True recurrencewas observed in 9.5% (109/1145), and delayed recurrence at 6.4 months onaverage (0-48 months). Postoperative complications developed in 12.3 %(141/1145), including 1.4% (16/1145) with severe complaints. Clinicaloutcomes at our institution, particularly for the third group (model C-APSwith MRI/CT fusion images) were close to those of the Marseille group.
So far, we have regarded RGR targeting as more advantageous than REZ
targeting in terms of both efficacy and safety. The reasons are; 1) possibleto irradiate with optimal dose (90Gy) with care to protect brain stem, 2) moreaccurate treatment with availability of MRI/CT fusion images. Indications for Elderly Patients with Intractable TGN
In order to confirm GKS indications for elderly patients (more than 65
years old) suffering from intractable TGN, Hayashi et al 7) investigated 69elderly subjects from the Marseille prospective study of 110 patients. Threeissues were considered:1) Comparison of clinical outcomes between elderly and younger groups:
Initial pain relief was observed in 95.7% of the elderly group (vs. 100% in younger group), true recurrence in 16.7% (vs. 10.5% inyounger group), and postoperative complications in 2.9% (vs. 5.4%in younger group). As to the response of TGN for GKS, the youngergroup had slightly more favorable results than the elderly group. However, results are apparently acceptable for elderly patients.
2) Comparison of clinical outcome in between previous surgical inter-
vention (PSI) and no previous surgical intervention (NPSI) group:Initial pain relief was observed in 92.6% (PSI) and 97.6%(NPSI),true recurrence in 20%(PSI) and 24.4%(NPSI), and postoperativecomplications in 12%(PSI) and 9.8%(NPSI), respectively. The NPIgroup had better results than the PI group, indicating that elderlypatients with TGN should undergo GKS as the critical procedurebefore surgical intervention.
3) Comparison of clinical outcomes between 90Gy and lower dose
groups: Initial pain relief was observed in 96.8% of 90 Gy group(vs. 94.7% in lower dose group), true recurrence in 12.9% (vs. 27.8%in lower dose group), and postoperative complications in 3.2% (vs. 2.6% in lower dose group). Notably, the rate of true recurrence wassignificant higher in the lower dose group (p<0.05). On the otherhand, the rate of postoperative complication did not differ signifi-cantly. Thus, 90 Gy appears to be an optimal dose for elderly pa-tients.
In treating elderly patients with TGN, we recommend using the optimal
radiosurgical dose (90Gy at maximum) before any surgical intervention. Overall Management and Treatment Indications for TGN
If the patient is relatively younger, we recommend surgical intervention
first, because the long-term effects of radiosurgery for TGN are yet unknown. Surgical procedures should be selected according to localization of the pain,severity of vessel involvement and patient choice (Fig.3). If surgical pro-cedures fail or the effect is inadequate, we recommend GKS. If the patientis older, we recommend GKS as the first treatment for TGN prior to surgi-cal procedures (Fig.3). Likewise, in young patients, if surgery fails or its effectis inadequate, we recommend a second GKS or other surgical proceduresas necessitated by the patient’s condition. Conclusions
Overall, 15,000 cases suffering from TGN have been treated by GKS
worldwide. In addition, many published reports on clinical results and strat-egies have emphasized that GKS provides satisfactory results to most pa-tients with few severe complications. To date, TGN has been widely acceptedas an indication for GKS in the functional disease field. However, its mecha-nism of action has not yet been elucidated. If GKS produces destructive changein the nerve itself, patients will have sensory loss affecting half of the face. Fig. 3: Clinical indication for essential Trigeminal Neuralgia. TGN: Trigeminal neuralgia,MS: Multiple sclerosis, MVD: Micro vascular decompression, RF: Radiofrequency.14th Meeting of the World Society for Stereotactic and Functional NeurosurgeryTable 1. The list of treatment indications and diagnostic criteria for essential TGN
3) No neurological deficit (no sensory abnormality of face, no corneal hyporeflex)
4) No other type of pain (no atypical pain)
5) Trigger (touch & face washing/ tooth brushing/ mastication/ speech/ etc, swallowing)
A 90 Gy dose appears to be sufficient to produce a functional effect, termedthe “Biological Differential Effect”, on the normal nerve/CNS without tis-sue ablation. This concept is expected to play an important role in treatingother functional diseases. Epilepsy and cancer pain have been managed withpituitary radiosurgery. Therefore, both basic and clinical studies are neededto confirm the efficacy and safety of GK radiosurgery for functional diseases. Of course, it goes without saying that we need much longer follow-up af-ter treatment to make an evaluation if GKS is an appropriate treatment forpatients with TGN. References
1) Mullan S, Lichtor T: Per cutaneous microcompression of the trigeminal
ganglion for trigeminal neuralgia. J Neurosurg 59: 1007-1012, 1983.
2) Barker FG, Janetta PG, Bissonette DJ, et al: The longterm outcome of
microvascular decompression for trigeminal neuralgia. N Engl J Med, 334:1077-1083, 1996.
3) Régis J, Bartolomei F, Metellus P, et al: Radiosurgery for Trigeminal Neuralgia
and Epilepsy. Application of Radiosurgery. Neurosurg Clin N Am, 10: 359-377, 1999.
4) Kondziolka D, Lunsford D, Flickinger JC, et al: Stereotactic radiosurgery
for trigeminal neuralgia: A multi-institutional study using the gamma unit. J Neurosurg 84: 940-945, 1996.
5) Maesawa S, Salame C, Flickinger JC, et al : Clinical outcomes after stere-
otactic radiosurgery for idiopathic trigeminal neuralgia. J Neurosurg 94:14-18, 2001.
6) Fukuoka S: Gamma knife radiosurgery for trigeminal neuralgia – Multi-
institute study of 1145 cases in Japan -. Presented at 12th Leksell Interna-tional Conference of Gamma Knife Society, Vienna, Austria, 2004.
7) Hayashi M: Current Gamma knife surgery for intractable pain [in Japa-
nese]. Pain Clinic 24 (2): 213-231, 2003.
MONSTRUL I FILOSOFII R spunzînd unei întreb ri a lui Hans-Jürgen Heinrichs, Peter Sloterdijk observ c exist o rezisten a filosofilor în fa a a ceea ce este imposibil de controlat ra ional, în fa a fenomenelor care dau de gîndit i care amenin s pun sub semnul întreb rii certitudinile intelectuale larg acceptate. Din acest punct de vedere, filosofia s-ar asem na cu gîndirea comun i n-ar
2ND YEAR RESEARCH ELECTIVE RESIDENT’S JOURNAL Randomized, Placebo-Controlled, Double Blinded Clinical Trial of Bupropion (*Wellbutrin) vs. Venlafaxine (*Effexor) for the Treatment of Hot Flashes in Men undergoing Androgen Ablation Therapy for Prostate Cancer Andrew B. Brown A. Study Purpose and Rationale Hot Flashes pose a significant clinical problem worldwide in men who are
 14th Meeting of the World Society for Stereotactic and Functional Neurosurgery
Fig. 1 demonstrates 2D image and Fig3 shows 3D image. Both figures display theanatomical relationships including the trigeminal nerve and surrounding vital struc-tures. The artery obviously conflicts the trigeminal nerve located on trigeminal incisula,and the never is properly covered by the 50% isodose area of 4mm isocenter.
Fig. 1, 2: Irradiation planning for trigeminal neuralgia (GammaPlan)
served in 3.0% (4/134). Delayed recurrence was detected at 6-24 months(mean 9 months). Postoperative complications (hypoesthesia and dysesthesia)developed in 10.9%(16/147), but there were no mortalities. In those whoreceived GKS only once, this rate was 9.5% (14/147). We also investigatedclinical outcome according to the following treatment factors:1) First generation group (1998-2001): treatment using model B with-
out completely fusion images: 29 cases (27 cases with follow-up)
2) Second generation group (2002): treatment using model B with com-
pletely fusion images: 14 cases (all with follow-up)
3) Third generation group (2003-2004): treatment using model C-APS
with completely fusion images: 157 cases (106 cases with follow-up)
Initial significant pain reduction was observed in 92.6% (25/27) of the
first group, 100% of the second (14/14) and the third (106/106). The respectivepain free (= complete relief of electric discharge) rate was 63% (17/27), 85.7%(12/14), and 99.1% (105/106). Those with true recurrence were 12% (3/25),8.3% (1/12) and 0% (0/105). Postoperative complication rates were 14.8%(4/27), 14.3% (2/14) and 9.5% (10/105). Both third group cases that developedpostoperative dysesthesia underwent GKS twice. Although the follow-upof the third group is yet insufficient, the results are clearly the best amongthe three.
14th Meeting of the World Society for Stereotactic and Functional Neurosurgery
Fig. 1 demonstrates 2D image and Fig3 shows 3D image. Both figures display theanatomical relationships including the trigeminal nerve and surrounding vital struc-tures. The artery obviously conflicts the trigeminal nerve located on trigeminal incisula,and the never is properly covered by the 50% isodose area of 4mm isocenter.
Fig. 1, 2: Irradiation planning for trigeminal neuralgia (GammaPlan)
served in 3.0% (4/134). Delayed recurrence was detected at 6-24 months(mean 9 months). Postoperative complications (hypoesthesia and dysesthesia)developed in 10.9%(16/147), but there were no mortalities. In those whoreceived GKS only once, this rate was 9.5% (14/147). We also investigatedclinical outcome according to the following treatment factors:1) First generation group (1998-2001): treatment using model B with-
out completely fusion images: 29 cases (27 cases with follow-up)
2) Second generation group (2002): treatment using model B with com-
pletely fusion images: 14 cases (all with follow-up)
3) Third generation group (2003-2004): treatment using model C-APS
with completely fusion images: 157 cases (106 cases with follow-up)
Initial significant pain reduction was observed in 92.6% (25/27) of the
first group, 100% of the second (14/14) and the third (106/106). The respectivepain free (= complete relief of electric discharge) rate was 63% (17/27), 85.7%(12/14), and 99.1% (105/106). Those with true recurrence were 12% (3/25),8.3% (1/12) and 0% (0/105). Postoperative complication rates were 14.8%(4/27), 14.3% (2/14) and 9.5% (10/105). Both third group cases that developedpostoperative dysesthesia underwent GKS twice. Although the follow-upof the third group is yet insufficient, the results are clearly the best amongthe three.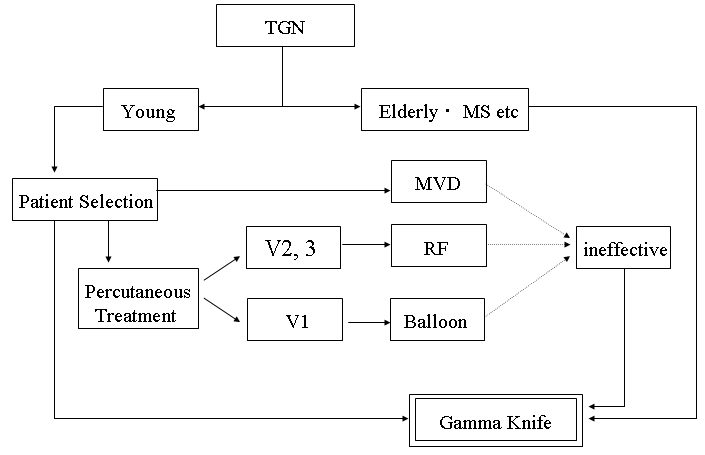 In treating elderly patients with TGN, we recommend using the optimal
radiosurgical dose (90Gy at maximum) before any surgical intervention.
In treating elderly patients with TGN, we recommend using the optimal
radiosurgical dose (90Gy at maximum) before any surgical intervention.