Fibromyalgia: practical treatments for the family physician
Perspectives: A View of Family Medicine in New Jersey
Fibromyalgia: Practical Treatments for the Family Physician Richard N. Podell, MD Source: Perspectives: A View of Family Medicine in New Jersey
(Written for Perspectives (4Q05), a journal of the New Jersey Academy of Family Physicians, and reprinted with permission.) Richard N. Podell, MD, Clinical Professor in the Department of Family Medicine at UMDNJ-Robert Wood Johnson Medical School, practices internal medicine in Springfield and Somerset, New Jersey. His website address is DrPodell.org. According to the Arthritis Foundation, women are seven times more likely to develop fibromyalgia than men, but the disease can affect individuals of any age, including children and the elderly. What Is Fibromyalgia?
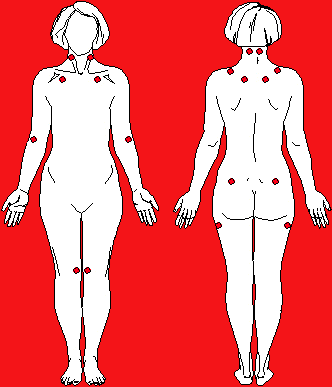
As defined by the American College of Rheumatology (ACR) in 1990 [1], the diagnosis of Fibromyalgia (FMS) requires: 1) one key point of history: chronic widespread pain and/or soreness in 4 quadrants of the body and 2) one key point of physical exam: painful tenderness at 11 or more of 18 designated anatomic sites, called tender points (See Figure 1). Figure 1: Anatomic Locations of the 18 Designated Fibromyalgia Tender Points
Tender points are areas of musculo-tendinous insertion. These sites are normally more sensitive to pressure than other sites on the body. “Normals” feel tenderness when pressed at these points using a force of 4 Kg.
Perspectives: A View of Family Medicine in New Jersey
When pushing with the thumb, this is roughly the force needed to make the thumbnail blanch. Where a normal person will feel tenderness at the tender points, fibromyalgia patients feel pain. Fibromyalgia, by this definition, affects some 2% of adult Americans. However, if we relax the 11 of 18 tender point requirement; diffuse, chronic fibromyalgia-like pain may affect about 10% of U.S. adults. Most fibromyalgia patients have mainly sore muscles with little else wrong. However, a significant number of patients have more complex, multi-system complaints. [2,3] These symptoms may include:
Mental concentration problems – also called “fibro fog”
Current research suggests that increased pain sensitivity in fibromyalgia is due to anatomical and functional up-regulation of the pain signaling pathways in the spinal cord and brain. [4,5] This neurological mechanism is called neural sensitization (think of the volume knob on a radio turned up to very high, amplifying and distorting the radio signal). Fibromyalgia patients report feeling pain at much lower levels of pressure, and at heat or cold stimulation than do healthy normal patients. Objective evidence supports the accuracy of these reports; i.e. they are not “making it up,” but actually feel the pain. Functional MRI studies provide the most dramatic support for this by showing increased regional blood flow to areas that are normally associated with a pain response. [6,7] Both normal patients and fibromyalgia patients show regional blood flow changes when they report pain; fibromyalgia patients show these changes at much lower levels of stimulus. The functional MRI results have been confirmed using other objective markers including SPECT scan and cerebral evoked potentials. [8,9]
In addition to having a lower pain threshold, repeated stimulation causes pain intensity to increase more rapidly in fibromyalgia patients. Once the stimulus stops, pain in the fibromyalgia patient fades more slowly than it does in normal patients. If one continues to apply very mild further stimulus the pain continues to fade in normal persons. However, with fibromyalgia patients, even very light continuing stimuli can keep the pain going. [10] Also, control subjects become less sensitive to painful stimuli shortly after they exercise. Fibromyalgia patients, in contrast, become more sensitive. [11] These findings are all independent of potential confounding factors such as co-morbid depression or disability litigation. Cerebrospinal fluid in Fibromyalgia Syndrome (FMS) shows the following abnormalities [12]:
An increased level of substance P, a pro-inflammatory mediator
Increased level of CSF (Cerebrospinal fluid) opiates
Reduced CSF levels of the neurohormone, serotonin.
Perspectives: A View of Family Medicine in New Jersey
Animal models have shown local injury can induce an increased sensitivity to pain similar to fibromyalgia. Activation of NMDA (N-methyl-D-aspartate) receptors play a central role in these experimental models. It has been shown that ketamine, an NMDA antagonist, can prevent neural sensitization in these animal models. NMDA receptors are also involved in human fibromyalgia. A single I.V. injection of ketamine improves pain in a large proportion of fibromyalgia patients. [13] Taken together these studies provide objective evidence to support the conclusion that fibromyalgia patients actually feel the pain they report, and that abnormal neural sensitization plays a key role in FMS. Primarily, FMS is a physical illness whose “end-organ” damage is mainly in the central nervous system. However, psychological issues can often be relevant not only as exacerbating factors, but as secondary effects of the illness. About half of all chronic fibromyalgia patients become anxious or depressed during the course of their illness, especially those whose symptoms are severe. Fibromyalgia sufferers are also more likely to have a prior history of depression or anxiety than are those of controls in research studies. This suggests that mood disorders and fibromyalgia may have some common risk factors or vulnerabilities. However, roughly half of fibromyalgia patients have no prior history of depression or anxiety and do not develop mood problems during their illness. And while several anti-depressants can help fibromyalgia pain, this improvement occurs independent of whether or not the patient is depressed. Our best explanation is that fibromyalgia and disorders of mood share common risk factors but are not the same. [14] The bottom line for clinicians: This is a physical, not mainly a mental, illness. But, when anxiety, depression, and/or poor coping skills co-occur with fibromyalgia, it is important to give each the attention it deserves. Differential Diagnosis and Evaluation:
Diagnosing fibromyalgia demands a number of other disease rule outs [2]: AUTOIMMUNE DISORDERS: The first rule outs are for autoimmune/inflammatory diseases such as polymyalgia rheumatica, Rheumatoid Arthritis (RA), myositis and Lupus. However, it is fairly common for a patient to have an autoimmune inflammatory disease and fibromyalgia at the same time. An estimated 25-40% of RA and Lupus (SLE) patients also have fibromyalgia (non-inflammatory) pain, which is often not recognized. This is important since the best medicines for fibromyalgia are different from those that work best for inflammation. An important differential point is that in fibromyalgia, while joint pain is common, joint swelling should not occur. Morning stiffness, however, is common in fibromyalgia. To evaluate chronic fibromyalgia patients for autoimmune disease, a sed rate ANA and CPK should be obtained. MUSCULOSKELETAL: Various musculoskeletal lesions produce widespread muscle pain through direct pressure within the CNS (a spinal disc or Chiari cerebellar tonsilar herniation). Peripheral orthopedic problems can also cause diffuse pain (osteoarthritis, poor posture, repetitive strain at work, or a short leg). Perspectives: A View of Family Medicine in New Jersey
If fibromyalgia is severe or worsening, consider an MRI of the brain and/or cervical spine. Always evaluate posture, factors affecting repetitive strain and an orthopedic exam. INFECTIOUS DISEASE: The best-documented infectious causes include Lyme disease and hepatitis B. Most likely, a wide variety of different viral illnesses can set off a fibro-like process. In areas with a high incidence of Lyme disease, such as New Jersey, strongly consider a Lyme screening test.
SLEEP DISORDERS: People who have fibromyalgia have a higher than expected rate of periodic leg movement disorder, sleep apnea, and also a more subtle version of sleep apnea called upper airway resistance syndrome (UARS). It is also known that disrupting slow wave sleep in a sleep lab can create fibromyalgia-type pain after just one night. Chronic pain in turn causes non-restorative sleep. At the very least, the sleeping patient should be observed at home by a family member for at least 30 minutes. It is also good practice to get an overnight sleep study on fibromyalgia patients who are chronic, severe or worsening. PSYCHIATRIC DISORDERS: A psychiatric and mental status exam is essential in the treatment of fibromyalgia, since fibromyalgia, anxiety and depression are often found together, each making the other illness worse. Many psychiatric illnesses can mimic fibromyalgia. For example, though not extremely common, some patients’ pain disappears entirely when treated for anxiety or depression. METABOLIC DISORDERS: Metabolic causes should be considered in fibromyalgia, including statin medications, low thyroid, low adrenals, and, rarely, neoplastic disease. Patients should be routinely screened for CBC, CMP, urinalysis and TSH. Also, obtain a cortisol evaluation if blood pressure is low or if the patient has lost weight. It is important to know that fibromyalgia patients tend to gain weight. If weight loss has occurred look for other causes for the symptoms. When conducting a physical on a fibromyalgia patient, be sure to check BP and pulse both sitting and after 5 minutes of standing. Orthostatic problems are fairly common. Neurogenic hypotension and postural orthostatic tachycardia are among the more treatable aspects of complex fibromyalgia. Try to avoid tilt- table testing, as it is apt to cause a prolonged flare-up of symptoms. Pharmacotherapy for Fibromyalgia Pain When it comes to pharmacotherapy for fibromyalgia there is good news and bad news. The good news is that we are finally starting to see double blind studies for a wide range of drugs. The bad news is that no one class of drugs is likely to help more than a subgroup of patients. Trial and error remains the best guide for which patients are likely to respond to which class of medicine. Severe or complex fibromyalgia patients tend to be unusually sensitive to the side effects of medication This may be another manifestation of their neural sensitivity. Among the patients with multi-system complaints there is often increased sensitivity to bright lights, loud noises, pungent smells, and a vulnerability to stress. When starting drug therapy in fibro patients:
1) Start new medicines at one half or less of the usual low-end starting dose 2) Titrate slowly over days or weeks
Perspectives: A View of Family Medicine in New Jersey
3) Forewarn the patient about potential side-effects and that these side effects tend to diminish over
There are no FDA approved drugs for fibromyalgia. However, 12 distinct drug classes now have data supporting their use in the treatment of fibromyalgia. (See Table 1). Of these, four classes are easily used by the family physician. These are tricylic anti-depressants, SSRI’s, norepinephrine/serotonin reuptake inhibitors (NSRI’s), and the GABA analogue anti-seizure drugs. Tricyclics: Both amitriptyline (Elavil) and cyclobenzaprine (Flexeril)–a muscle relaxant related to the tricyclics-- have favorable double blind studies supporting their use in fibromyalgia [15,16]. Other tricyclics, such as nortriptyline (Pamelor), may be effective, but double-blind studies have not been done. Trazadone, though not a tricyclic, has anecdotal support. The degree of benefit with tricyclics can be large, but often it is only modest. Side effects include sedation, dry mouth, prolonged QT interval, heart arrhythmia and weight gain. I usually start with nortriptyline, since it’s less sedating than amitriptyline. I begin at 10 mg qhs and work up slowly in increments of 10 mg. Benefit can be seen in one night, but a fair trial requires several weeks. SSRI’s: SSRI’s are worth a try but don’t expect too much benefit for pain, despite improved mood. Fluoxetine (Prozac) has had mixed results for fibromyalgia pain. Arnold found benefit in a 12 week long study using flexible dosing from 10 mg to 80 mg daily. [17] Goldenberg also found fluoxetine to be better than placebo, especially when combined with tricyclics. [18] Norepinephrine Serotonin Reuptake Inhibitors (NSRI):Duloxetine (Cymbalta), high-dose venlafaxine (Effexor), and the tricyclics are the main drugs available with both norepinephrine and serotonin-like actions. Duloxetine became available in late 2004. It has one good double blind study showing benefit for FMS pain. [19] This benefit was independent of its effect as an anti-depressant. In contrast, two open label venlafaxine studies showed no benefit for fibromyalgia pain. I find that duloxetine is very helpful for some patients but not at all helpful for others. Nausea is a major problem, even at low doses. However, it does tend to fade after a week or so. Duloxetine comes in 20 mg, 30 mg and 60 mg doses (samples are 30 mg). I suggest starting with 20 mg to 30 mg daily for a week, then work up toward 60 mg. This was the dose used in the double blind study. Several studies of depression used 120 mg daily. Do not open the duloxetine capsule, as the ingredients can cause gastric irritation. Do not mix with any other NSRI, or with SSRI’s or tricyclics–except for transitioning from one to another. There are no strict rules for how to switch over from these drugs to duloxetine. I taper down on the old drug while introducing duloxetine. Make sure to explain the (small) potential risk of hyperserotonin syndrome. If a psychiatrist is involved be sure to include him/her in the discussion. While the manufacturer has no recommendations for or against combining duloxetine with bupropion HCl (Wellbutrin) it is important to know that duloxetine is metabolized through the 2D6 cytochrome pathway. Bupropion may inhibit this pathway, in effect, raising the duloxetine dose. Perspectives: A View of Family Medicine in New Jersey
GABA-related: Gabapentin (Neurontin) while approved for seizure disorders, is also often used for pain syndromes, including fibromyalgia. Anecdotal reports are encouraging, although there are no double blind studies for fibromyalgia.
Because FMS patients are especially sensitive to side effects, I usually start with a 100 mg test dose of gabapentin at night. I then build up to at least 300 mg qhs before adding daytime medications. If daytime dosing is not tolerated I slowly increase the nighttime treatment dose up to 1200 mg or so qhs. Optimal dosing for fibromyalgia pain might be at about 900 mg tid (about 2700 mg daily) though this is higher than the manufacturer’s recommendation of up to 1800 mg a day. Sedation, mental cloudiness, dizziness, ataxia, double vision, and tremor often limit dosing. Unusually, increased serum creatinine has been reported. Pregabalin (Lyrica) has been approved for diabetic neuropathy and should be available soon. Pregabalin has one good double blind study showing benefit in FMS. [20] Side effects are probably similar to those of gabapentin. Other Pain Therapies:
Aspirin and the ibuprofen class are not as good for managing fibromyalgia as they are for inflammatory disease. Corticosteroids are also not very good. If these anti-inflammatories work well, reconsider the diagnosis. Some fibromyalgia specialists use methadone, hydrocodone (Vicodin), fentanyl transdermal system (Duragesic) or other opiates while others refuse to use narcotics. Unless you have a special interest in pain medicine, most primary care physicians should probably not get involved with chronic opioid treatment. However, prescribing occasional narcotics for breakthrough pain is generally acceptable. Tramadol hydrochloride tablets (Ultram), when effective, is the first choice among potential opioid class treatments. Tramadol hydrochloride/acetaminophen and acetaminophen may have a synergistic effect–as in Tramadol hydrochloride (Ultracet). [21] However, acetaminophen is potentially hepatotoxic. Counsel patients not to take acetaminophen with alcohol nor when fasting (with a flu) as fasting inactivates the main detox pathway of glucoronidation. If it is necessary to take acetaminophen regularly, oral N-acetyl cysteine (Mucomist), a precursor of glutathione, is available in health food stores. NAC via glutathione might protect against acetaminophen liver problems.
Innovative Therapies:
Other drugs for fibromyalgia pain are likely to help certain sub-groups of patients, however a pain specialist should manage their use. These “innovative” FMS drugs include: Sodium oxybate (Xyrem) - a GABA-B receptor agonist: This drug is approved for a sub-type of narcolepsy, however there are three double blind studies which show benefit for fibromyalgia. [22,23] The most recent report was by Jon Russell, M.D., presented in abstract at the November, 2005 meeting of the American College of Rheumatology. This study showed that Xyrem was substantially more effective than placebo with a P value—the likelihood that the result could have arisen by change—being less than one chance in 500. Still Xyrem is definitely not a cure-all. Only 34.5% of persons using Xyrem were classified Perspectives: A View of Family Medicine in New Jersey
as “responders”; but this was much better than the response rate for persons on placebo. Only 12.5% of placebo treated patients had a positive response. My personal experience have truly dramatic improvement with Xyrem both for fibromyalgia pain and for quality of sleep. And it is encouraging is that sodium oxybate is one of only a few drugs with good data that proves it can increasing the duration of deep stage 3-4 sleep. However, I have also found that Xyrem is a difficult medicine to use. Initially, side effects are very common. These often but do not always fade out after a few weeks on the drug. Many of my patients have had to stop Xyrem because of these side effects. I recommend that persons interested in taking Xyrem should have an over night sleep study first. Persons with sleep apnea should probably not be put on Xyrem at this point, since Xyrem can have respiratory depressant effects. The ordering physician should request that the sleep specialist specifically look for the presence of alpha-delta sleep. (This is not always done routinely.) Anecdotal suggestions are that persons with the alpha-delta pattern—about half of fibromyalgia patients—may be more likely to improve from taking Xyrem. It is important to strictly manage and monitor the use of sodium oxybate as it is identical to the “date-rape” street drug GHB (gamma hydroxybutyric acid). To prevent abuse and assure physician and patient education all U.S. prescriptions for sodium oxybate are processed through a single mail-order pharmacy. There have been no cases of abuse reported with this program. 5HT3 (Serotonin subtype 3) Receptor Antagonists - Odansetron (Zofran): This drug, and others in the class, can cause serious constipation and/or ischemic colitis. Only a small minority of patients are able to tolerate odansetron on an on-going basis. However, for those that do, it can be worthwhile. There are also several double blind European studies of topisetron (not available in the U.S.) that show clear benefit for fibromyalgia pain for a large minority of patients. [24,25] NMDA (N-Methyl-D-Aspartate) Receptor Antagonists: Double blind studies show that a single infusion of the NMDA antagonist anesthetic, ketamine, can often reduce fibromyalgia pain for hours or even days. [26] Unfortunately, I.V. ketamine requires very careful monitoring due to potential cardiac and psychiatric side effects. Ketamine’s street name, “Special K”, reflects it’s high potential for abuse. We look forward to industry’s development of safer NMDA receptor antagonist drugs. Growth Hormone: Nearly 90% of fibromyalgia patients fail to show the expected rise in growth hormone levels immediately after exercise. [27] Pyridostigmine (Mestinon), a parasympathetic/acetyl-choline enhancer, corrects the growth hormone defect within hours [28] but there is no clinical improvement short term. However, one very good, but as yet unpublished, study suggested that pyridostigmine improved fibromyalgia related fatigue and sleep quality. Pain also improved, but was not statistically significant. Growth hormone injections were also effective over a six month time frame when given to the approximately 30% of FMS patients whose IGF1 level is in the low or low average range. However, the degree of improvement, while statistically significant, was relatively modest. Pyridostigmine is contraindicated if there is heart block or bradycardia. Side effects include abdominal cramps, increased salivation, sweating, increased bronchial secretion, diarrhea, and hyperacidity. Perspectives: A View of Family Medicine in New Jersey
Dopamine enhancing medicines: Holman and Myers published a double blind study using pramipexole (Mirapex) for fibromyalgia pain. (Pramipexole’s usual use is for Parkinson’s Disease and also for Periodic Leg Movement Disorder.) Mirapex was substantially better than placebo with 42% of Mirapex treated patients improving by 50% or more compared with only 14% for placebo treated patients. Critical to their success may be that Holman and Myers started treatment at a very low dose, 0.125 mg. They then increased the dose very slowly, so that it took several months to reach the high doses at which statistically significant benefit was found. Nausea was a common side-effect. Using an anti-nausea agent such as Tigan in the early stages might potentially improve tolerance. Selegeline (also known as Deprenyl) also increases dopamine action but in a different way. There have been anecdotal reports of benefit for fibromalgia pain, but no double blind studies. Other Drugs: Tizanidine (Zanaflex) and baclofen, usually used for multiple sclerosis muscle spasm, are occasionally useful for fibromyalgia. CAUTION: The Food and Drug Administration has not approved any drugs as effective for fibromyalgia. Thus, all medicines discussed in this essay are “off label” uses. It is perfectly legal, ethical and proper for a physician to prescribe these for fibromyalgia, and for a patient to take them. However, we should be aware that the studies done to date have not risen to the very high level of proof that FDA approval demands. The potential side effects for all these drugs are listed in the package insert that you can obtain from your druggist, or one can look these up in a reference book such as the PDR. Potential drug interactions pose a more difficult problem. Some of these are known e.g. the potential interaction between the new norepinephrine/serotonin reuptake inhibitor, Cymbalta, and the serotonin/SSRI class of drugs such as Prozac. However, for the most part, interactions are not tested for systematically. So, it’s important persons taking new combinations be especially alert for adverse symptoms and also stay in close touch with their doctors. Perspectives: A View of Family Medicine in New Jersey
Table 1: MEDICINES FOR FIBROMYALGIA PAIN. CLASS/medicine Evidence Level*
NOREPINEPHRINE/SEROTONIN REUPTAKE INHIBITORS (NSRI)
Sodium Oxybate (Xyrem) (also known as GHB)
• Evidence level: A=3+ double-blind controlled studies. B=one or two positive double-blind
studies. C=Mixed results or anecdotal support
Perspectives: A View of Family Medicine in New Jersey
Exercise: The Goldilocks Principle
Most experts recommend exercise as a core fibromyalgia treatment. Decreased physical activity leads to de-conditioning, which tends to worsen fibromyalgia pain, mood, sleep and other aspects of health. However, following the “no pain no gain” approach can often do more harm than good. [30, 31, 32] How much exercise is appropriate? Goldilocks’ answer is best: “not too much or too little, but just the right amount.” Unfortunately, “just right” is different for different patients at different times. Walking half a mile may be appropriate for one person during one period of their illness, while 50 yards might work best for another person at another time. We cannot rely on the standard heart rate and shortness of breath criteria for how much exercise is just right. That’s because with fibromyalgia the adverse effects of over-doing exercise are often delayed. A patient will not know that they over did it until the pain, stiffness and/or fatigue flare-up occurs hours later or the next day. Fortunately, patients usually learn their limits, and can then slowly increase their level of exercise. I recommend starting an every other day program to make it easier to recognize the delayed flare-up response. If your patient is working with physical therapists and “trainers” it is important for them to understand the delayed post-exertion flare-up phenomenon so they can adjust their treatments accordingly. [Call out box – to go in exercise section] Several recent reports suggest that exercise in a warm water pool may be an especially useful exercise for fibromyalgia patients. [33]
[End call out box] Coping with Chronic Illness–Cognitive Behavioral Therapy (CBT) [34, 35, 36, 37]
Many people who suffer from chronic illness - not just fibromyalgia - develop habits of thought and action that tend to make their symptoms worse. They may over-do activity on good days, causing symptoms to flare. They may feel angry and/or not “in control.” They may under-appreciate the positive and catastrophically over-react to the negative. Family members may have their own mal-adaptive responses. While normal, these responses must be addressed, whether or not anxiety or depression also is a problem. Short-term cognitive behavioral therapy (CBT) or “talk” therapy which focuses on coping skills can prevent or interrupt the vicious cycle of physical distress, and poor coping, which in turn makes the illness worse. Most psychologists who do short term therapy use some variant of CBT. Formal controlled studies using CBT for fibromyalgia tend to show at least a modest degree of benefit as an adjunctive treatment. Patients with moderate or severe fibromyalgia should be evaluated to see how their coping skills are faring. Relaxation skills such as deep breathing or biofeedback might also have value. Perspectives: A View of Family Medicine in New Jersey
Fibromyalgia and Sleep Are Intimately Inter-related [38, 39, 40] Almost all fibromyalgia patients complain of non-restorative sleep. Unfortunately, most sleep medicines, including tricyclics, are often not very good at improving sleep quality. People sleep more but don’t feel well-rested. Sodium oxybate or gamma hydroxybutyrate (Xyrem) may be an exception. It improves slow wave sleep and sleep quality. Because of the safety concerns associated with the use of this drug, the distribution of it is tightly restricted. Because fibromyalgia is a chronic disease there is an unavoidable tension between the goals of treating insomnia and of avoiding dependence on sleep medications. I tend to err on the side of treating sleep problems aggressively, except among those who are at high risk for drug abuse. The best choice will differ for each doctor and each patient and should be discussed frankly.
When working with sleep issues, sleep hygiene maneuvers such as regular bedtime, hot baths a few hours before sleep, and gearing down throughout the evening should be the first step. Non-habit forming sedating medications include amitryptiline, cyclobenzaprine, trazadone, gabapentin, tizanidine, eszopiclone (Lunesta), baclofen, and anti-histamines can be considered. Some physicians believe that the benefits outweigh the risks for long-term use of zolpidem (Ambien), zaleplon (Sonata) or benzodiazepines such as clonazepam (Klonopin). Conclusion: We are finally beginning to see double blind studies on fibromyalgia treatments. Results are encouraging. Many different drug classes seem likely to help certain subsets of patients. We are also beginning to understand the underlying mechanisms of fibromyalgia as an abnormality involving the central nervous system’s pain signaling pathways. The simple form of fibromyalgia can usually be treated fairly well with a combination of medication, appropriately monitored exercise and cognitive therapy support. The complex form of fibromyalgia remains a frustration, but we are beginning to see signs that we have begun to make progress. References 1. Wolfe F, Smythe H, Yunus M, et. al. The American College of Rheumatology 1990 criteria for the classification of fibromyalgia: Report of the Multicenter Criteria Committee Arthritis Rheum 1990;33:160–725. 2. Russell IJ, Editor. The fibromyalgia syndrome: a clinical case definition for practitioners, Journal of Musculoskeletal Pain, 2003;11:1-107. 3. Clauw D, Crofford L. Chronic widespread pain and fibromyalgia: what we know, and what we need to know. Best Practice & Research Clinical Rheumatology 2003; 17:685-701. 4. Bennett R. Emerging concepts in the neurobiology of chronic pain: evidence for abnormal sensory processing in fibromyalgia. Mayo Clin Proc. 1999;74:385-98. 5. Bennett R. Disabling fibromyalgia: appearance versus reality. Journal of Rheumatology 1993:20:1821-2. Perspectives: A View of Family Medicine in New Jersey
6. Gracely R, Petzke F, Wolf J, et. al. Functional magnetic resonance imaging evidence of augmented pain processing in fibromyalgia. Arthritis Rheum. 2002;46:1333-43. 7. Gracely R, Grant M, Giesecke T. Evoked pain measures in fibromyalgia. Best Practice & Research Clinical Rheumatology. 2003;17;593-609. 8. Staud R, Domingo M. Evidence for abnormal pain processing in Fibromyalgia. Pain Medicine, 2001;2:208-15. 9. Staud R, Vierck C, Robinson M, et. al. Spatial summation of heat pain within and across dermatomes in fibromyalgia patients and pain-free subjects. Pain. 2004; 111:342-50. 10. Staud R, Price D, Robinson M, et. al. Maintenance of windup of second pain requires less frequent stimulation in fibromyalgia patients compared to normal controls. Pain. 2004;110:689-96. 11. Vierck C, Staud R, Price D, et. al. The effect of maximal exercise on temporal summation of second pain (windup) in patients with fibromyalgia syndrome. The Journal of Pain. 2001;2:334-44. 12. Russell IJ, Orr M, Littman B, et. al. Elevated cerebrospinal fluid levels of substance P in patients with the fibromyalgia syndrome. Arthritis Rheum. 1994;37:1593-601. 13. Graven-Nielsen T, Aspergren Kendall S, Henriksson K, et. al. Ketamine reduces muscle pain, temporal summation and referred pain in fibromyalgia patients. Pain. 2000;85:483-501. 14. Arnold L, Hudson J, Hess E, et. al. Family study of fibromyalgia. Arthritis & Rheumatism. 2004;50:944-52. 15. Carette S, Bell M, Reynolds W, et. al. Comparison of amitriptyline, cyclobenzaprine and placebo in the treatment of fibromyalgia. A randomized, double-blind clinical trial. Arthritis Rheum. 1994;37:32-10. 16. Hannonen P, Malminiemi K, Yli-Kerttula U, et. al. A randomized, double-blind , placebo-controlled study of mecolobemide and amitryptiline in the treatment of fibromyalgia in females without psychiatric disorder. Br J Rheumatol. 1998;37:1279-86. 17. Arnold L, Hess E, Hudson J, et. al. A randomized, placebo-controlled, double-blind, flexible-dose study of fluoxetine in the treatment of women with fibromyalgia. Am J Med. 2002;112:191-7. 18. Goldenberg D, Felson D, Dinerman H. A randomized controlled trial of amitryptiline and naproxen in the treatment of patients with fibromyalgia. Arthritis and Rheum. 1986;29:1371-7. 19. Arnold L, Lu Y, Crofford L, et. al. A double-blind, multicenter trial comparing duloxetine with placebo in the treatment of fibromyalgia patients with or without major depressive disorder. Arthritis, Rheum. 2004:50:2974-84. 20. Crofford L, Rowbotham M, Mease P, et. al. Efficacy of pregabalin for treatment of pain and associated symptoms in patients with FMS. J Musculoskeletal Pain. 2004; 12 (Suppl 9): S49.
Perspectives: A View of Family Medicine in New Jersey
21. Bennett RM, Kamin M, Karim R, Rosenthal N. Tramadol and acetaminophen combination tablets in the treatment of fibromyalgia pain: a double-blind, randomized, placebo-controlled study. Am J Med. 2003 May;114(7):537-45. 22. Scharf M, Baumann M, Berkowtiz D. The effects of sodium oxybate on clinical symptoms and sleep pattern in patients with fibromyalgia. J Rheumatol. 2003; 30:1070-4. 23. Scharf M, Hauck M, Stover R, et. al. Effect of gamma-hydroxybutyrate on pain, fatigue, and the alpha sleep anomaly in patients with fibromyalgia. Preliminary reports. J Rheumatol 1998; 25:1986-90. 24. Haus U, Varga B, Stratz T, et. al. Oral treatment of fibromyalgia with tropisetron given over 28 days: influence on functional and vegetative symptoms, psychometric parameters and pain. Scand J Rheumatol Suppl. 2000;113:55-89. 25. Farber L, Stretz T, Bruckle W, et. al. Efficacy and tolerability of tropisetron in primary fibromyalgia–a highly selective and competitive 5-HT3 receptor antagonist. German Fibromyalgia Study Group. Scand J Rheumatol Suppl. 2000;113:49-54. 26. Sorensen J, Bengtsson A, Ahlner J, et. al. Fibromyalgia–are there different mechanisms in the processing of pain? A double blind crossover comparison of analgesic drugs. J Rheumatol. 1997:24:1615-21. 27 Bennett R, Clarck S, Walczyk J. A randomized, double-blind, placebo-controlled study of growth hormone in the treatment of fibromyalgia. Am J Med. 1998;104:227-31. 28. Jones K, Bennett R, Burckhardt C, et. al. Improving Growth Hormone Secretion in Fibromyalgia: Response to Pyridostigmine and Exercise. J Musculoskeletal Pain. 2004; 12 (Suppl 9): S49 34. 29.Holman A, Myers R. A randomized, double-blind, placebo-controlled trial of pramipexole, a dopamine agonist, in patients with fibromyalgia receiving concomitant medications. Arthritis Rheum. 2005 Aug; 52(8):2495-505. 30 Jones K, Clark S, Bennett R. 2002 Prescribing exercise for people with fibromyalgia. AACN Clin Issues. 2002;13:277-93. 31. Clark S, Jones K, Burckhardt C. Exercise for patients with fibromyalgia: risks versus benefits. Curr Rheumatol Rep. 2001;3:135-46 . 32. Jones K, Burckhardt C, Clark S. A randomized controlled trial of muscle strengthening versus flexibility training in fibromyalgia. J Rheumatol. 2002;29:1041-8.
33. Mannerkorpi K, Ahlmen M, Ekdahl C. Six and 24 month follow-up of pool exercise therapy and education for patients with fibromyalgia. Scand J Rheumatol. 2002;31:306-10. 34. Sim J, Adams N. Systematic review of randomized controlled trials of nonpharmacological interventions for fibromyalgia. Clin J Pain. 2002;18:324-36.
Perspectives: A View of Family Medicine in New Jersey
35. Williams D, Cary, M, Groner K, et. al. Improving physical functional status in patients with fibromyalgia: a brief cognitive behavioral intervention. J Rheumatol. 2002;29: 1280-6. 36. Rossy L, Buckelew S, Dorr N, et. al. A meta-analysis of fibromyalgia treatment interventions. Ann Behav Med. 1999;21:180-91. 37. Cedraschi C, Desmeules J, Rapiti E, et. al. Fibromyalgia: a randomized, controlled trial of a treatment program based on self management. Ann Rheum Dis. 2004;63:290-6. 38. Moldofsky H, Scarisbrick B, England R, et al. Musculoskeletal symptoms and non-REM sleep disturbance in patients with fibrositis syndrome and healthy subjects. Psychosomatic Medicine 1975:37:341-51. 39. Gupta, M, Moldowfsky H. Dysthymic disorder and rheumatic pain modulation disorder (fibrositis syndrome): A comparison of symptoms and sleep physiology. Can J Psychiatry. 1986;31:608-16. 40. Lentz M, Landix C, Rothermel J, et. al. Effects of selective slow wave sleep disruption on musculoskeletal pain and fatigue in middle aged women. J Rheumatol. 1999;26:1586-92. Dr. Podell can be reached at 105 Morris Avenue, Springfield, NJ 070781 or 973-218-9191. Web: www.DrPodell.org
Prescription Drug Overdose Is Leading Cause of Accidental Death in U.S. Addiction Shreds the Emotional Fabric of Families Prescription drug overdose is now the second leading cause of accidental death in the United States. (Motor vehicle deaths are first.) Approximately 26,000 Americans are dying from prescription drug overdoses annually, according to the Center for Disease Control and
soft drinks white wines beers on tap > mineral water medium or without gas bottle 0,75 lt. 3,80 > Müller-Thurgau Kressbronner Berghalde QbA, regional, dry 0,25 lt. 4,30 > Farny Premium-Pils Oskar Farny, lager bitter > mineral water medium or without gas bottle 0,33 lt. 2,40 > tasting fresh, lively and like muscatel > L
 Perspectives: A View of Family Medicine in New Jersey
Perspectives: A View of Family Medicine in New Jersey