Cholinergic blockade does not alter the nasalcongestive response to irritant provocation*
Dennis Shusterman1, Mary-Alice Murphy2, Paula Walsh1, John R. Balmes1
Division of Occupational and Environmental Medicine, University of California, San Francisco, U.S.A.
Department of Pediatrics, University of California, San Francisco, U.S.A. Objective: To understand the mechanism underlying the nasal congestive response to irritantchallenge. Methods: We exposed 22 subjects – 8 with seasonal allergic rhinitis (SAR), 6 with perennialallergic rhinitis (PAR), and 8 normals – to chlorine (Cl2) gas (1.0 ppm x 15 min.) by nasalCPAP mask. Control exposures (filtered air) were carried out on separate days, with counter-balancing of exposure order. Nasal airway resistance (NAR) was measured in triplicatebefore and after the provocation sequence using active posterior rhinomanometry. For eachsubject, this experiment was repeated twice, after [double-blinded] pre-treatment with: 1)ipratropium bromide (IB) 0.6% nasal spray, and 2) vehicle. Results: As a group, allergic rhinitics (SAR + PAR) showed greater [Cl2] exposure-relatedincreases in NAR than did normals on placebo (vehicle) pretreatment days (p < 0.05). IBpre-treatment, however, did not have a systematic effect on Cl2-induced congestion. Conclusion: Cholinergic mechanisms do not appear to be responsible for the nasal conges-tive response to irritant provocation.Key words: nasal irritation, nasal congestion, chlorine, cholinergic reflexes, ipratropiumbromide
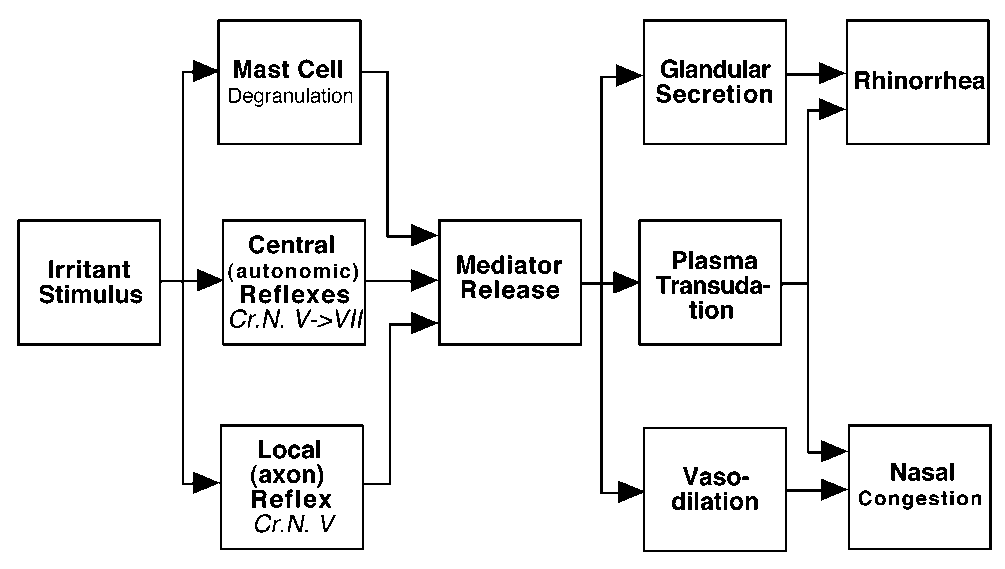
INTRODUCTIONPhysical or chemical irritation of the upper respiratory tractmay be associated with reflex responses, including nasal con-gestion and rhinorrhea (McLean et al., 1979; Widdicombe,1990; Bascom et al., 1991; Kjaergaard et al., 1995; Shustermanet al., 1998). Experiments involving exposure of human volun-teers to environmental tobacco smoke (ETS) suggest that non-allergic - including possible neurogenic - mechanisms may beresponsible for the acute congestive response to chemical nasalirritation (Bascom et al., 1991). Potential neurogenic mecha-nisms include both central (autonomic) and local (axon)reflexes (Figure 1) (Bascom, 1992). For the irritant-inducednasal secretion, evidence is compelling that central (parasym-
Figure 1. Potential mechanisms involved in acute reflex responses to
pathetic) reflexes are operative (Meltzer, 1992; Sanico and
nasal irritation (including nasal congestion and rhinorrhea).
Togias, 1998). For irritant-related congestion, on the otherhand, direct evidence regarding mechanism (which must acton the vascular compartment in order to affect airway caliber)is largely lacking.
more responsive to this stimulus than are normal controls(Shusterman et al., 1998). We wished to build upon these find-
We have previously shown that low-level chlorine (Cl2) gas,
ings in order to better understand the pathophysiology of irri-
administered by nasal mask, is an effective stimulus for nasal
tant-related nasal congestion. The current study was designed to
congestion, and that seasonal allergic rhinitic subjects are
explore the role of autonomic (specifically, cholinergic) mecha-
*Received for publication: September 4, 2001; accepted: May 20, 2002
nisms in the congestive response to irritant provocation. To this
approved by the Committee on Human Research of the
end, the topical cholinergic blocker, ipratropium bromide (IB),
University of California, San Francisco. Detailed question-
was employed as a pharmacologic probe. IB was applied, alter-
naires were then administered to each potential subject, who
nating with placebo in a double-blinded manner, prior to nasal
was then provisionally classified as having seasonal allergic
irritant provocation with Cl2 gas, examining the effect, if any, of
rhinitis (SAR), perennial allergic rhinitis (PAR), no rhinitis
this pre-treatment on irritant-related nasal congestion.
(NR), or “other” based upon questionnaire responses.
Allergy skin prick tests (to 13 regionally common aeroallergens
The provocation experiment – which was repeated twice on
/ mixes, plus saline and histamine controls) were then admin-
each subject after double-blinded pretreatment with either IB
istered. For purposes of this study, “seasonal allergic rhinitics”
or placebo – consisted of a randomized, cross-over design
were defined as subjects with: 1) a history of seasonally occur-
comparing the response of allergic rhinitic (AR) and non-
ring sneezing, nasal pruritis, rhinorrhea, post-nasal drip, and/or
rhinitic (NR) subjects to a 15-minute controlled exposure to
nasal congestion, with or without known precipitants; and 2)
dilute Cl2 by nasal mask. The physiologic endpoint of interest
skin test reactivity to at least one seasonally occurring agent
was nasal airway resistance (NAR), measured before pretreat-
from the panel that corroborated the history. (“Skin test reac-
ment, after pretreatment, immediately after exposure, and
tivity” is defined as a wheal reaction to skin-prick testing with a
again 15 minutes after exposure. Exposures consist of either
diameter ≥p the histamine control.) “Perennial allergic
pure air (control conditions) or chlorine (1.0 ppm) diluted in
rhinitics” were defined as subjects with year-around symptoms
air. Cl2 and air exposures took place on separate days, roughly
who had predominant skin test reactivity to dust mites, molds,
one week apart. The study was counterbalanced with respect
pet danders or cockroach antigen(s). “Non-rhinitics” were
to order of exposure and subject gender (Figure 2).
defined as subjects who report, at most, infrequent nasal symp-toms, without identified seasonal variation or precipitants, and
with significant skin test reactivity to no more than one agent
Subjects were recruited through posters and newspaper adver-
in the panel of 13 aeroallergens. Prior to skin testing, subjects
tisements. Inclusion criteria were: age 18-40 yrs. and “general
were asked to refrain from taking antihistamines for 72 hours
good health”; exclusion criteria were: 1) a history of asthma, 2)
(hydroxyzine for 3 weeks, astemizole for 12 weeks).
cigarette smoking (active or within previous 6 months), 3)pregnancy or lactation, 4) a history of severe allergic reactions
(anaphylaxis or angioedema), and 5) continuous therapy with
SAR subjects were tested outside of their relevant pollen sea-
medications having antihistaminic side effects (e.g., tricyclic
son. All subjects were asked to avoid exercising, consumption
antidepressants). After completion of a screening question-
of spicy foods, or use of scented cosmetics on the day of test-
naire, subjects read and signed an informed consent document
ing. In addition to the above antihistamine preclusions, sub-jects were asked to avoid using nasal steroids for at least 2weeks, and nasal decongestants for at least 48 hours prior totesting. Upon arrival at the laboratory, subjects entered a cli-mate-controlled chamber (22 ± 1°C, 40 ± 3% RH) with filteredair (activated charcoal and high-efficiency particulate). After a15-min waiting period, baseline symptoms (nasal irritation,nasal congestion, rhinorrhea, post-nasal drip, and odor) wererated on a visual analog scale using a computer mouse(Performa 6115CD computer, Apple Computers, Cupertino,CA; LabView® software, National Instruments, Austin, TX). The scale was indexed at equal intervals with the words“none,” “slight,” “moderate,” “strong,” “very strong,” and“overpowering,” corresponding to the numerical range of 0.00to 5.00. Baseline nasal airway resistance (NAR) was thenobtained in triplicate via the technique of active posterior rhi-nomanometry using a commercial instrument (Model NR6-2,GM Instruments, Kilwinnig, UK). The rhinomanometer wascalibrated on a daily basis; the pressure channel to a tolerance
Figure 2. Counterbalanced, cross-over design of chlorine-provocation
experiment. Experiment was repeated twice, on a double-blinded
of ± 3% using a Model 405 incline manometer (Airflow
basis, after pre-treatment with either ipraropium bromide 0.6% (IB) or
Developments, Inc., High Wycombe, GB), and flow to a toler-
placebo (vehicle) nasal spray, 0.2 mL/nostril.
ance of ± 5% with a Model 235 flow meter (Cole-
Parmer/Gilmont Instruments, Vernon Hills, IL). Finally, base-
and either a paired Student's t or a paired non-parametric test
line pulmonary peak flow was obtained in triplicate using a
(Wilcoxon signed-ranks) utilized as appropriate. Subjects acted
hand-held peak flow meter (Wright Peak Flow Mini-Meter,
as their own controls in paired group analysis of NAR changes
Clement Clarke International, Ltd., UK).
on Cl2 exposure vs. air days. Results were then compared for
After rating baseline symptoms and having baseline rhino-
IB- vs. vehicle (placebo) pretreatmet.
manometry and pulmonary peak flow measurements, subjectswere administered either IB or placebo (vehicle) on a double-
blinded basis. Both agents were administered by aerosol spray
A total of 22 subjects were enrolled, consisting of 8 seasonal
unit (No. 34478, Pfeiffer of America, Princeton, NJ), consisting
allergic rhinitics, 6 perennial allergic rhinitics, and 8 non-
of 3 sprays of 0.067 mL each (total volume, 0.20 ± 0.01
rhinitic controls. Each group was evenly divided by gender.
mL/nostril). Fifteen min later, symptom rating, rhinomanome-
The mean age for each subgroup was 27.8, 28.0, and 29.3 years,
try, and pulmonary peak flow were repeated.
The investigator then stepped behind a screen and adjusted thebreathing mixture for the nasal mask assembly. The chlorine
Individual rhinomanometry data appear in Table 1. Because of
dilution apparatus blended compressed medical-grade air and
small subgroup size and power considerations, SAR and PAR
compressed chlorine diluted to 10 ppm in medical-grade air
subjects were combined for purposes of analysis of rhino-
(Nellcor Puritan-Bennett, San Ramon, CA) in a stainless steel
manometry data. For baseline NAR values, there was no signifi-
mixing chamber (Model FMX7311: Omega Engineering,
cant effect of pretreatment with either IB or placebo (data not
Stamford, CT). Diluent air was pre-conditioned to 22°C and 40%
shown). As a consequence, baseline values for the NAR and
RH using a Model 009700 humidifier-heater (Intertech
symptom analyses were taken after pretreatment with either IB
Corporation, Bannockburn, IL). Immediately downstream from
or vehicle. Nasal provocation with dilute (1.0 ppm) Cl2 for 15
the mixing chamber was the sampling port for an electrochemi-
min. produced a significantly greater congestive response among
cal chlorine monitor (Model 1340; Interscan Corp., Chatsworth,
allergic rhinitic (AR) subjects than among nonrhinitic controls
CA), which continuously sampled the gas mixture and fed its
(p < 0.05 for three of four testing conditions - Table 2). With the
output to a strip chart recorder (Model 1200; Linear Instruments,
exception of a single individual (subject # 20), pretreatment
Inc., Irvine, CA). The gas mixture was conveyed to the subject
with IB (0.06%; 0.2 mL/nostril) 15 min. prior to Cl2 challenge
with 2.5 cm diameter corrugated respiratory tubing, connected by
did not significantly alter the magnitude of reflex congestion
T-piece to a nasal CPAP* mask (Series 3121; Respironics, Inc.,
among AR subjects (treatment effect p = 0.98 immediately post-
Murraysville, PA), which was sized according to the individual
exposure, and p = 0.49 at 15 min. post-exposure).
subject. The second limb of the T-piece connected to a low-pres-
Subjectively, subjects reported modest increases in odor and
sure scavenger system, which led to an exhaust outside of the
nasal irritation ratings from baseline to post-chlorine exposure,
chamber and building. The combination of a high flow rate (60
regardless of diagnostic subgroup or pre-treatment status
l/min) and the scavenger system allowed subjects to breathe with
(Table 3). Pooling data across subjects, significant increases in
negligible superimposed pressure or resistance. The chlorine
self-rated odor and irritation were apparent immediately post-
meter was re-calibrated on a daily basis using the [certified] con-
exposure for both IB and placebo pretreatment days. There
tents of the chlorine cylinder as the standard.
were no significant changes in self-rated nasal congestion post-
The 15-minute exposure period via nasal mask took place on a
exposure. Interestingly, there was a trend toward decreasing
single-blinded basis, and the order-of-presentation was subject
rhinorrhea and post-nasal drip ratings after either Cl2 or air
to limited randomization (within the constraints of the coun-
provocation, unrelated to pre-treatment status (i.e., IB vs.
terbalanced study design). Immediately after cessation of expo-
placebo). No systematic changes in pulmonary peak flow were
sure – and then again 15 minutes later – the investigator asked
observed after either Cl2 or air exposure (data not shown).
subjects to re-rate nasal symptoms using visual analog scales. NAR was re-measured in triplicate after each symptom rating
session, and finally, pulmonary peak flow was re-assessed.
Reflex nasal congestion has been documented in response toirritant provocation with ammonia (NH3), sidestream tobacco
smoke (STS), Cl2, and mixed volatile organic compounds
Statistical analysis was performed using JMP (SAS Institute,
(VOCs) (McLean et al., 1979; Bascom et al., 1991; Kjaergaard
Carey, NC). The hypotheses tested were: 1) that seasonal aller-
et al., 1995; Shusterman et al., 1998). Given the lack of markers
gic rhinitic subjects would show a significantly greater increase
of mast cell degranulation noted after STS provocation,
in NAR over baseline (comparing chlorine- vs. air-exposure
Bascom (1992) hypothesized that neurogenic mechanisms –
days); and 2) that pretreatment with IB would reduce or elimi-
including central (autonomic) and local (axon) reflexes – may
nate this difference. Data were first examined for normality,
be responsible for the congestive response to nasal irritation. Direct evidence on this issue is largely lacking. With regard to
* CPAP = Continuous positive airway pressure
central reflexes, however, McLean and colleagues (1979) pre-
Table 1. Individual Rhinomanometry Data (Pa/L/s).
treated subjects with atropine (a cholinergic blocker) prior to
rhinitic subjects. Specifically, rhinitics alone showed significant
NH3 challenge, and did not note a systematic effect on irritant-
congestive response, both immediately – and 15 min. after –
irritant provocation. Pre-treatment with IB did not materiallyalter this response. This suggests that any parasympathetic
In this experiment, we again found differential sensitivity to
reflex response elicited by Cl2 exposure did not have a signifi-
irritant (Cl2) provocation among allergic rhinitic vs. non-
cant effect upon the vascular compartment of the nose (which
Our findings are consistent with previous work, including both
Table 2. Mean Change in Nasal Airway Resistance, Chlorine MinusAir Trial (Pa/L/s ± SEM).
agonist and antagonist studies, suggesting that cholinergicstimulation affects nasal glandular secretion to a greater degree
than it does vascular function and upper airway caliber(McLean et al, 1979; Gerth van Wijk and Dieges, 1994). The
specific mechanism of irritant-induced nasal congestion is
unknown, but based upon work to-date, neither parasympa-thetic reflexes nor mast cell degranulation appear to be likely
explanations. Another candidate mechanism involves the axon
reflex, with release of vasoactive peptides (including substance
P) locally. Our future studies will address this possibility in amore direct fashion.
"Post-1" = Immediately post-exposure; “Post-2” = 15 min.
This work was supported by the National Institute on
Deafness and Other Communication Disorders (DC K23
* p < 0.05, baseline to post-exposure, rhinitics vs. controls
00121) and the National Institute of Environmental HealthSciences (ES R01 10424). Funding for formulation of ipratropi-um bromide and placebo was received in the form of an unre-
is believed to be responsible for nasal congestion)
stricted gift from Boehringer-Ingelheim Pharmaceuticals.
(Widdicombe, 1990). Objective congestion, on the other hand,
Aerosol spray delivery units were kindly provided by Pfeiffer
occurred with modest subjective nasal irritation, suggesting
of America. The authors also wish to thank Joanne Whitney of
that the reflex mechanism involved is sensitive to relatively
the UCSF Drug Product Services Laboratory for her expert
Table 3. Mean Chlorine-related Symptoms (0 to 5 scale, immediately post-exposure) by Diagnostic Subgroup and Pre-treatment Status. Subgroup Pre-Treatment Irritation Congestion Rhinorrhea Post-Nasal
Bascom R, Kulle T, Kagey-Sobotka A, Proud D (1991) Upper res-piratory tract environmental tobacco smoke sensitivity. Am RevRespir Dis 143: 1304-1311.
Bascom R (1992) Differential responsiveness to irritant mixtures:Possible mechanisms. Ann NY Acad Sci 641: 225-247.
Gerth van Wijk R, Dieges PH (1994) Nasal reactivity to histamineand methacholine: Two different forms of upper airway respon-siveness. Rhinology 32: 119-122.
Kjaergaard S, Rasmussen TR, Molhave L, Pedersen OF (1995) Anexperimental comparison of indoor air VOC effects on hayfever-and healthy subjects. In: Healthy Buildings '95 (Proceedings),University of Milano.
McLean JA, Mathews KP, Brayton PR, Solomon WR, Bayne NK(1979) Effect of ammonia on nasal resistance in atopic andnonatopic subjects. Ann Otol 88: 228-234.
Meltzer EO (1992) Intranasal anticholinergic therapy of rhinor-rhea. J Allergy Clin Immunol 90: 1055-1064.
Sanico A, Togias A (1998) Noninfectious, nonallergic rhinitis(NINAR): Considerations on possible mechanisms. Am J Rhinol12: 65-72.
Shusterman D, Murphy M-A, Balmes J (1998) Seasonal allergicrhinitic and non-rhinitic subjects react differentially to nasal provo-cation with chlorine gas. J Allergy Clin Immunol 101: 732-740.
Widdicombe JG (1990) Nasal pathophysiology. Respir Med 84 SupA: 3-10.
Dennis Shusterman, MD, MPHUpper Airway Biology LaboratoryUniversity of California, San Francisco1301 So. 46th Street, Bldg. 112Richmond, CA 94804USA
Tel: +1-510-231-9551Fax: +1-510-231-5636E-mail: dennis@itsa.ucsf.edu
Supplemental Graphics
The Ethics of Social Work. Principles and Standards Adopted by the IFSW General Meeting, Colombo, Sri Lanka, July 6 -8, 1994 1. Background Ethical awareness is a necessary part of the professional practice of any social worker. His or her ability to act ethically is an essential aspect of the quality of the service offered to clients. The purpose of IFSW's work on ethics is to
MEDICATING FERAL KITTENS Some Helpful Guidelines for Medicating Feral Kittens from www.urbancatleague.org With sickly feral kittens try to use your vets most effective but least traumatic treatment available. Handling kittens unnecessarily to medicate them will set back the socialization process and sometimes make a timely socialization impossible. Along with medical treatment
 Cholinergic blockade does not alter the nasalcongestive response to irritant provocation*
Dennis Shusterman1, Mary-Alice Murphy2, Paula Walsh1, John R. Balmes1
Division of Occupational and Environmental Medicine, University of California, San Francisco, U.S.A.
Cholinergic blockade does not alter the nasalcongestive response to irritant provocation*
Dennis Shusterman1, Mary-Alice Murphy2, Paula Walsh1, John R. Balmes1
Division of Occupational and Environmental Medicine, University of California, San Francisco, U.S.A.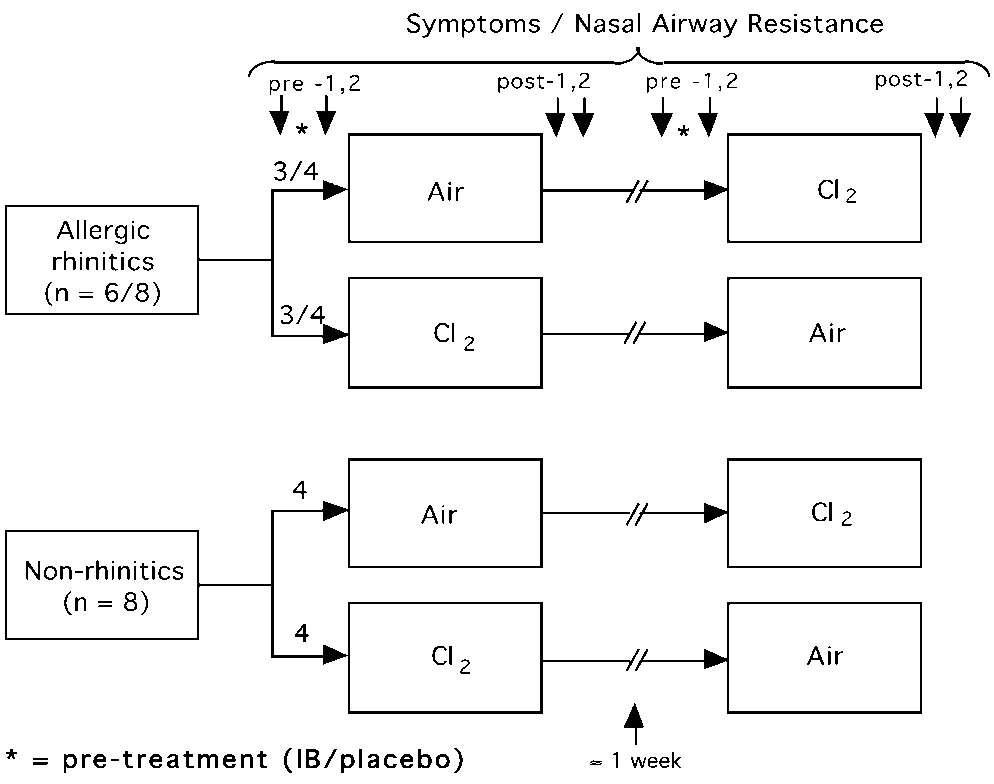 nisms in the congestive response to irritant provocation. To this
approved by the Committee on Human Research of the
end, the topical cholinergic blocker, ipratropium bromide (IB),
University of California, San Francisco. Detailed question-
was employed as a pharmacologic probe. IB was applied, alter-
naires were then administered to each potential subject, who
nating with placebo in a double-blinded manner, prior to nasal
was then provisionally classified as having seasonal allergic
irritant provocation with Cl2 gas, examining the effect, if any, of
rhinitis (SAR), perennial allergic rhinitis (PAR), no rhinitis
this pre-treatment on irritant-related nasal congestion.
nisms in the congestive response to irritant provocation. To this
approved by the Committee on Human Research of the
end, the topical cholinergic blocker, ipratropium bromide (IB),
University of California, San Francisco. Detailed question-
was employed as a pharmacologic probe. IB was applied, alter-
naires were then administered to each potential subject, who
nating with placebo in a double-blinded manner, prior to nasal
was then provisionally classified as having seasonal allergic
irritant provocation with Cl2 gas, examining the effect, if any, of
rhinitis (SAR), perennial allergic rhinitis (PAR), no rhinitis
this pre-treatment on irritant-related nasal congestion.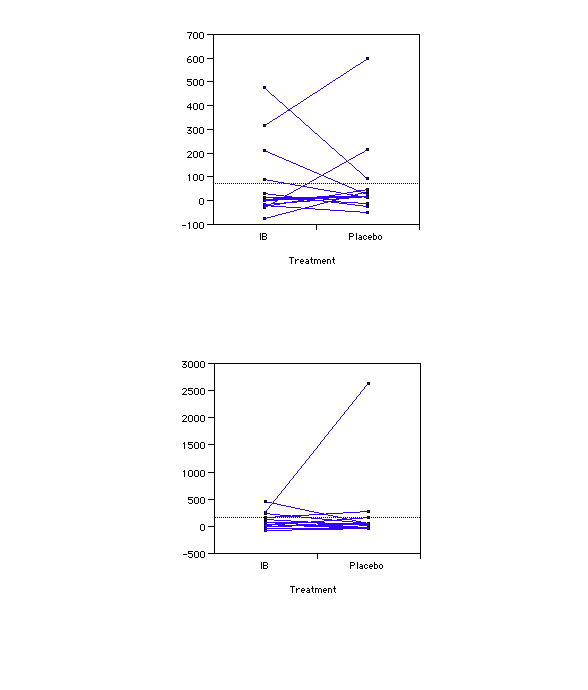 Supplemental Graphics
Supplemental Graphics