Original Article Effect of Eucaloric High- and Low-Sucrose Diets With Identical Macronutrient Profile on Insulin Resistance and Vascular Risk
A Randomized Controlled Trial R. Neil A. Black,1 Michelle Spence,2 Ross O. McMahon,1 Geraldine J. Cuskelly,2 Cieran N. Ennis,1 David R. McCance,1 Ian S. Young,2 Patrick M. Bell,1 and Steven J. Hunter1 The long-term impact of dietary carbohydrate type, in
cise are associated with the dramatic increase in preva-
particular sucrose, on insulin resistance and the develop-
lence of diabetes in developed countries. Western diets are
ment of diabetes and atherosclerosis is not established.
characterized by excess energy intake and increased levels
Current guidelines for the healthy population advise re-
of both sugar and fat (7). Increased consumption of
striction of sucrose intake. We investigated the effect of
refined sugar, including fizzy drinks, may contribute to the
high- versus low-sucrose diet (25 vs. 10%, respectively, of
increased risk of diabetes (8). Combined lifestyle interven-
total energy intake) in 13 healthy subjects aged 33 ؎ 3
tion, including caloric restriction and increased physical
years (mean ؎ SE), BMI 26.6 ؎ 0.9 kg/m2, in a randomized crossover design with sequential 6-week dietary interven-
activity, particularly with weight loss, can improve the
tions separated by a 4-week washout. Weight maintenance,
degree of insulin sensitivity and reduce the risk of future
eucaloric diets with identical macronutrient profiles and
diabetes and vascular disease (9 –12). The relative impor-
fiber content were designed. All food was weighed and
tance of different aspects of this approach is unclear. In
distributed. Insulin action was assessed using a two-step
particular, while there is evidence regarding the effect of
euglycemic clamp; glycemic profiles were assessed by the
different dietary caloric balances and macronutrient pro-
continuous glucose monitoring system and vascular com-
files, there is a lack of evidence regarding aspects of
pliance by pulse-wave analysis. There was no change in weight across the study. Peripheral glucose uptake and suppression of endogenous glucose production were simi-
Cross-sectional, longitudinal, and case-control studies
lar after each diet. Glycemic profiles and measures of
demonstrate no consistent association between dietary
vascular compliance did not change. A rise in total and LDL
carbohydrate type and risk of diabetes (13,14). Interven-
cholesterol was observed. In this study, a high-sucrose
tional studies in animal models, however, strongly link
intake as part of an eucaloric, weight-maintaining diet had
high-fructose and -sucrose diets to decreased insulin sen-
no detrimental effect on insulin sensitivity, glycemic pro-
sitivity and hyperlipidemia, as well as obesity. However,
files, or measures of vascular compliance in healthy nondi-
these diets are either hypercaloric, which leads to obesity,
abetic subjects. Diabetes 55:3566 –3572, 2006
or have grossly elevated contents of fructose or sucrose(up to 70 – 80% of total caloric intake) (15). These resultstherefore cannot be extrapolated to humans taking more
palatable levels of sucrose or fructose. Studies in human
nsulin resistance is a key feature of type 2 diabetes
subjects show variable effects with alterations of dietary
and precedes the onset of glucose intolerance (1–3).
sucrose intake when using simple measures of insulin
Insulin resistance is also an independent risk factor
sensitivity (16). One small study in seven subjects without
for atherosclerotic vascular disease (4 – 6). Factors
diabetes demonstrated that a high– glycemic index diet
that reduce the degree of insulin resistance may reduce
(25% sucrose) was associated with detrimental effects on
the likelihood of developing diabetes or atherosclerosis.
insulin sensitivity compared with a low– glycemic index
Changing dietary patterns and reduced levels of exer-
diet (1.2% sucrose) over 4-week dietary periods (17). It isoften assumed that a high-sucrose diet will have a highglycemic index but certain high-sucrose foods may have
From the 1Regional Centre for Endocrinology and Diabetes, Royal Victoria
comparable glycemic indexes to starchy foods (e.g., a
Hospital, Belfast, U.K.; and the 2Nutrition and Metabolism Group, The Queen’sUniversity of Belfast, Belfast, U.K.
carbonated orange drink and a mashed potato). Further
Address correspondence and reprint requests to Dr. Steven J. Hunter,
studies in type 2 diabetes have shown either no effect or a
Regional Centre for Endocrinology and Diabetes, Royal Victoria Hospital,
detrimental effect of increased dietary sucrose, but these
studies have been either small or of short duration (18 –
Received for publication 15 February 2006 and accepted in revised form 23
Recently, a number of low-carbohydrate high-fat diets
R.N.A.B. and M.S. contributed equally to this work.
(including the Atkins diet) have been proposed as a
DOI: 10.2337/db06-0220 2006 by the American Diabetes Association.
substitute for challenging modifications in lifestyle, but the
The costs of publication of this article were defrayed in part by the payment of page
long-term impact of such diets on cardiovascular and
charges. This article must therefore be hereby marked “advertisement” in accordancewith 18 U.S.C. Section 1734 solely to indicate this fact.
diabetes risk is still under investigation and debate (21–
R.N.A. BLACK AND ASSOCIATES
22). A meta-analysis has also highlighted that weight loss
at the beginning and end of each diet period. Blood pressure was measured
associated with such diets is associated more with caloric
using an oscillometric device (Omron Healthcare U.K., Milton Keynes, U.K.)
restriction than reduced carbohydrate content (23). It
and taken as the average of the second and third readings after 30-min supine. Insulin resistance, vascular compliance, and 72-h continuous subcutaneous
could be inferred that the same relationship holds for
glucose monitoring were assessed in the last week of each dietary period.
changes in insulin sensitivity. The concept of carbohydrate
Diets. A 7-day cyclic menu plan was formulated for both sucrose diets using
quality is also attracting attention, and a focus on glycemic
the dietary analysis program WISP (weighed intake software program; Tinu-
index forms the basis of an alternative dietary approach
viel Software, Warrington, U.K.). The low- and high-sucrose diets provided 10
(24 –26). A more conventional and proven approach is to
versus 25% of total dietary energy as sucrose, respectively (sucrose derived
advocate a balanced macronutrient profile, in conjunction
from both solid food and beverages). Diets were otherwise identical in theirmacronutrient and fiber intakes, both providing ϳ55% energy from carbohy-
with caloric restriction and other lifestyle measures, in
drate, 30 –35% energy from fat, 10 –15% energy from protein, and 18 g/day fiber.
both weight-reduction and weight-maintenance diets.
Volunteers attended daily, or on alternate days, throughout the interven-
Traditionally, dietary sugar or sucrose content is the
tion and were supplied with all appropriate foodstuffs (preweighed into daily
major focus of carbohydrate-based dietary guidelines. The
portions) for their particular diet. At each visit, the nutritionist discussed
term “sugars” is conventionally used to describe mono-
concerns and assessed dietary compliance. Throughout the study, caloric
and disaccharides. “Sugar,” by contrast, is used to describe
intake was adjusted if body weight (measured twice weekly) increased ordecreased on two successive occasions. Foods, ad libitum, included nonca-
purified sucrose (table sugar), as are the terms “refined
loric beverages (water, diet cola, black tea, and coffee) and seasoning. Alcohol
sugar” and “added sugar” (27). In 2003, the World Health
was not permitted. Representative menus for a single day for the high- and
Organization/Food and Agriculture Organization issued
low-sucrose diets are shown in Table 1. The energy distribution between the
guidelines for prevention of chronic disease in terms of
different meals was similar for both diets.
macronutrient balances, and although acknowledging a
Assessment of insulin action. At the end of each dietary period, insulin
lack of evidence, included a recommendation to restrict
sensitivity was assessed by a two-step euglycemic-hyperinsulinemic clamp, aspreviously described (32). A cannula was inserted into the left arm for
free sugars to Ͻ10% of total caloric intake (7). The
infusions and in the right arm for samples. The right hand was placed in a
American Heart Association adopted a similar approach
temperature-controlled plexiglass box (55°C) to arterialize the venous blood.
commenting on the potential detrimental effects of a
A primed-continuous infusion of high-performance liquid chromatography–
high-sucrose content diet with expected adverse effects
purified [3-3H]glucose was administered during a 2-h equilibration period
when content exceeded Ͼ20% of total energy intake (28).
(Ϫ120 min to zero time). The initial tracer prime was adjusted, based on
Such effects included a fall in HDL levels, a rise in
fasting plasma glucose (22). A two-step sequential, continuous infusion ofinsulin was commenced: 0.4 mU ⅐ kgϪ1 ⅐ minϪ1 (zero time to 120 min) then 2.0
triglycerides, and decreased vitamin and mineral content.
mU ⅐ kgϪ1 ⅐ minϪ1 (120 –240 min). Plasma glucose was measured at 5-min
In the U.K., the Department of Health recently suggested
intervals on a bedside analyzer (Beckman Glucose Analyzer 2; Beckman, High
reducing mean added sugar intake from 12.7 to 11% (29).
Wycombe, U.K.) and maintained at the desired fasting concentration by an
To inform dietary guidelines and develop advice regard-
exogenous infusion of 20% wt/vol glucose. Exogenous glucose was prelabeled
ing the impact of varying sucrose intake, we performed a
with [3-3H]glucose to match the predicted basal plasma glucose specific
randomized controlled trial of 10 and 25% sucrose diets (as
activity as described (32), with the modification that the primed-continuoustracer infusion was reduced to 50% of the basal rate after 20 min and to 25%
percent of total energy intake). The diets were isocaloric
of the basal rate after 140 min of insulin infusion (to maintain tracer steady
and weight maintaining with matched macronutrient pro-
files. (Specifically, the total carbohydrate quantity was the
Analytical techniques. Arterialised venous blood was used for all analyses
same in the trial diets, and the form of carbohydrate was
in the glucose clamp studies. Plasma for measurement of glucose specific
varied.) We examined the effect of these two diets on the
activity was deproteinized with barium hydroxide and zinc sulfate by the
primary outcome variable of insulin resistance, assessed
method of Somogyi (32). Aliquots of tracer infusate and labeled exogenousglucose infusion were spiked into nonradioactive plasma and processed in
using the isoglycemic-hyperinsulinemic clamp combined
parallel to allow calculation of [3-3H]glucose infusion rates. Serum insulin was
with isotope dilution techniques in healthy male volun-
measured by enzyme-linked immunosorbent assay (Abbot Imx; Abbott Labo-
teers. We also assessed 24-h glycemic profiles, serum
ratories, Berkshire, U.K.). Glucose was measured using an automated glucose
oxidase method using a Beckman Glucose Analyzer 2. Commercial kits wereused to estimate C-peptide (Dako Diagnostics, Ely, U.K.) and nonesterifiedfree fatty acids (Wako Chemicals, Neuss, Germany). RESEARCH DESIGN AND METHODS Calculations. The nonsteady state equations of Steele et al. (33), as modified
Fourteen healthy male volunteers were recruited (female subjects were
by De Bodo et al. (34), were used to determine the glucose appearance (R )
excluded to avoid the effect of the menstrual cycle on study end points).
and disappearance (R ), assuming a pool fraction value of 0.65 and an
Before commencing the study, a brief clinical history and examination was
extracellular volume of 190 ml/kg. This was measured over three 30-min time
carried out to ensure that those selected did not have significant obesity (BMI
periods: before insulin infusion (Ϫ30 to 0 min), during the final stages of the
Ͼ35 kg/m2) or cardiac, hepatic, or renal disease. Other exclusion criteria
low-dose insulin infusion (90 –120 min), and during the final stages of the
included a history of diabetes, blood pressure Ͼ140/80 mmHg, or hyperlipid-
high-dose insulin infusion (210 –240 min). The [3-3H]glucose infusion rates
emia (LDL Ͼ3.0 mmol/l and triglycerides Ͼ2.0 mmol/l). All patients gave
were calculated as the sum of the tracer infused continuously and the tracer
written informed consent, and the protocol for the study was approved by the
in the labeled exogenous glucose infusion. Rates of endogenous (hepatic)
research ethics committee of The Queen’s University of Belfast and the
glucose production were then calculated by subtraction of the exogenous
Administration of Radioactive Substances Advisory Committee.
glucose infusion rates required to maintain euglycemia from isotopically
Habitual dietary intake was assessed at baseline using a 4-day food diary
determined rates of glucose appearance.
(including at least one weekend day). Thereafter, volunteers were assigned to
Continuous glucose monitoring system. A continuous glucose monitoring
a randomized crossover trial consisting of a 6-week period of either low- or
system developed by MiniMed (CGMS; MiniMed, Northrodge, CA) was used to
high-sucrose intake, followed by a second 6-week period on the complemen-
monitor the concentration of interstitial fluid glucose for 48 –72 h using a
tary diet. The dietary periods were designed to meet projected isocaloric
subcutaneous sensor and was calibrated with a standard glucometer.
needs (estimated by multiplying basal metabolic rate by an appropriate
Arterial stiffness. Arterial stiffness was determined using pulse-wave anal-
activity factor [30]) and were separated by a 4-week washout phase during
ysis (model SCOR-Px; PWV Medical, Sydney, Australia), as described previ-
which volunteers returned to their usual diet. Volunteers were advised to
ously (35,36). All volunteers rested for 15 min in the supine position, and
maintain their usual level of physical activity throughout the study. Subjects
measurements were taken immediately following determination of brachial
were randomized in blocks of four using a random-number generator to
artery blood pressure. The right radial artery blood pressure waveform was
ensure that equal numbers of volunteers received high- or low-sucrose diets
recorded using a tonometer and calibrated according to the brachial systolic
during the first phase. Anthropometric measurements (weight, height, and
and diastolic pressures. Analysis of the central aortic waveform obtained
waist and hip circumference), fasting blood samples (plasma glucose, insulin,
using the SphygmoCor software identified the outgoing and reflected pressure
C-peptide, HbA , renal function, and lipids), and blood pressure were taken
waves (augmentation), occurring during systole. The augmentation index
SUCROSE, INSULIN RESISTANCE, AND VASCULAR RISK
TABLE 1Sample menus for a typical day on each intervention diet
Cornflakes (35 g), bran-based cereal (3 g)
Strawberry jam (20 g)Orange juice (200 g)
Yogurt with fruit purée (175 g)Carbonated orange drink (330 g)
Gravy, reconstituted (70 g)Carbonated orange drink (330 g)
Apple (170 g)Polyunsaturated margarine (15 g)
(expressed as a percentage) was defined as the ratio of augmentation to pulse
Weight and physical activity remained constant through-
pressure and was used to estimate overall systemic arterial stiffness (37). The
out the study. While no formal instrument to compare
timing of the reflected waveform (a measure of the transit time between the
physical activity was used, as weight and energy consump-
ascending aorta and the first main reflectance site) was also identified andtherefore used to indirectly estimate aortic pulse-wave velocity and, hence,
tion were the same after each diet, it can be assumed that
aortic stiffness (38). Arterial waveforms were also recorded by consecutively
the level of physical activity between the dietary periods
applanating the carotid and radial arteries gated to a three-lead electrocardio-
gram to enable calculation of pulse-wave velocity as previously described
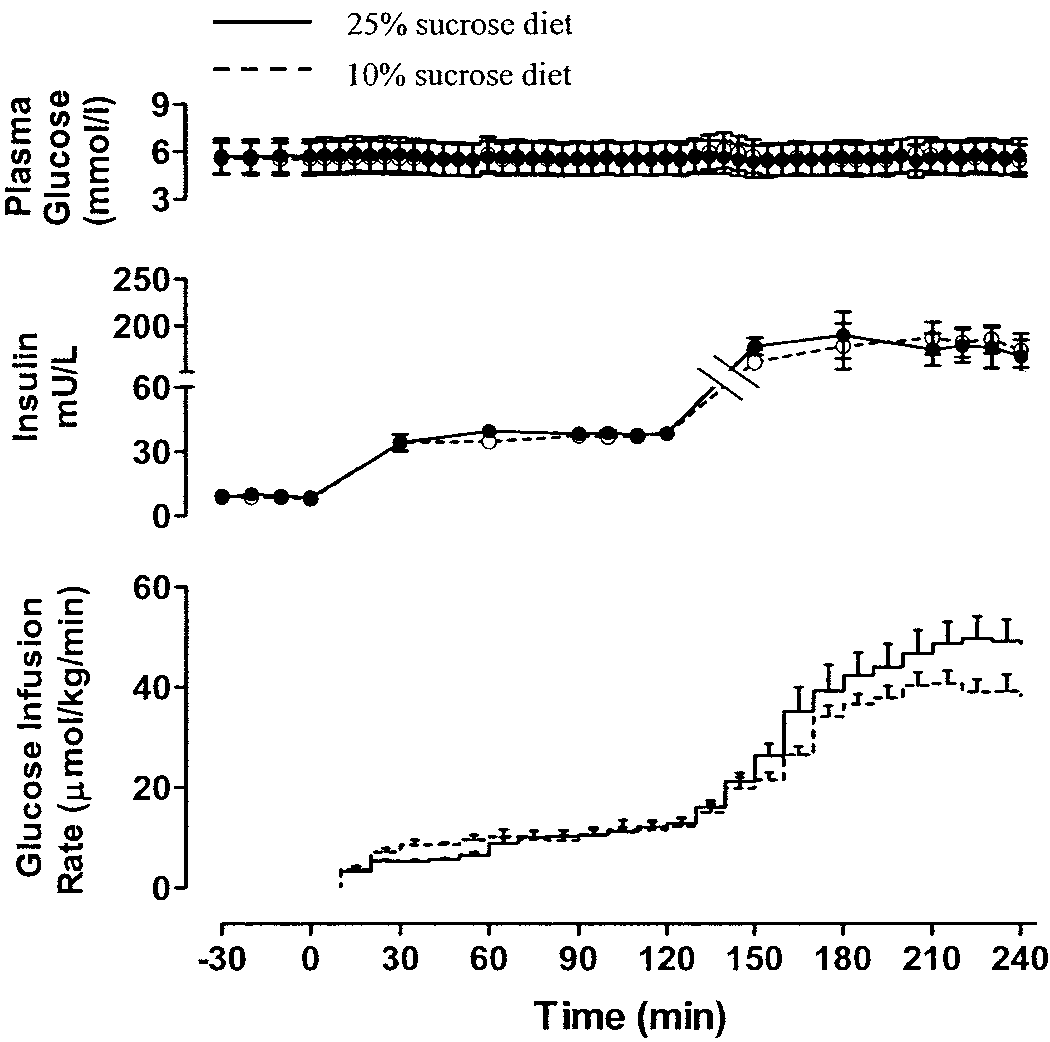
Clamp studies. Serum insulin levels in the fasting state
and during each infusion period were the same during
Statistical methods. Statistical analysis was as recommended by Hills and
both dietary periods. Plasma glucose was maintained at a
Armitage (40), enabling comparison of the effects of the treatment to beadjusted for period effects. Results are described as means Ϯ SE. Variables
constant level by exogenous glucose infusion with a
that were nonnormally distributed are described as median (lower quartile,
coefficient of variation Ͻ5% as the plateau for each clamp
upper quartile) and were logarithmically transformed before analysis. Where
(glucose infusion rates at plateau after 25 and 10% sucrose
parameters were assessed at the baseline and end of each period, ANCOVA
were 13.9 Ϯ 1.6 vs. 15.4 Ϯ 2.9 mol ⅐ kgϪ1 ⅐ minϪ1,
was used with baseline values as covariates. The power of the study,
respectively, after low-dose insulin and 47.5 Ϯ 3.5 vs.
calculated from previous clamp data, gave a 90% chance of detecting a 10%
42.5 Ϯ 3.0 mol ⅐ kgϪ1 ⅐ minϪ1 after high-dose insulin
change in insulin action at the 5% level of significance.
Both study diets were well tolerated (one subject left for
Baseline clinical and anthropometric characteristics (n ϭ 13)
reasons unrelated to the study). The clinical and anthro-
pometric characteristics of the volunteers are given in
Table 2. Volunteers were adult males who were, on
average, overweight (mean BMI 26.6 Ϯ 0.9 kg/m2) but were
normotensive with normal fasting lipid profiles and in-
dexes of glycemia. Simple fasting measures of insulin
sensitivity (insulin and homeostasis model assessment of
insulin resistance) indicated that the subjects were mod-
erately insulin resistant. The habitual dietary intake data
(Table 3) suggested that mean consumption of macronu-
trients was comparable with intakes reported for the adult
population of the U.K. (41). Within the group, the total
dietary energy provided by sucrose (preintervention)
ranged from 2 to13%. Daily intervention intakes of energy
and macronutrients during the high- and low-sucrose diets
are displayed in Table 3. Diets were matched for energy,
Data are means Ϯ SE or median (interquartile range). HOMA-IR,
macronutrient profile, and fiber intake (Table 4).
homeostasis model assessment of insulin resistance. R.N.A. BLACK AND ASSOCIATES
TABLE 3Habitual daily energy and nutrient intakes of the volunteers atbaseline
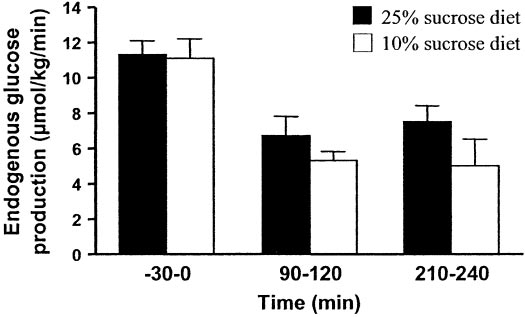
Data are means Ϯ SE. n ϭ 13. FIG. 2. Suppression of endogenous glucose production during euglyce-
infusion; Fig. 1). Endogenous glucose production was
mic-hyperinsulinemic clamp. Data are means ؎ SE.
similar in the fasting state and similarly suppressed afterlow- and high-dose insulin infusion on the 25 and 10%
effect on insulin resistance or measures of vascular risk in
sucrose diets (Figs. 2 and 3). Peripheral glucose utilization
healthy nondiabetic subjects. Evidence-based dietary
was no different after either low- or high-dose insulin
guidelines are urgently required to tackle the global epi-
infusion on the 25 and 10% sucrose diets. Serum nonest-
demic of diabetes. The absence of specific evidence in
erified fatty acids were suppressed similarly after 25 and
relation to sucrose has resulted in a lack of clear guide-
lines from some groups and variation in recommendations
Hemodynamic studies. Blood pressure, central augmen-
by others. Average sugar intake is much higher in the U.S.,
tation pressure, augmentation index corrected to heart
where 15% of men and 21% of women aged 19 –50 years
rate of 75 bpm, time to reflectance, and pulse-wave veloc-
have a sucrose intake Ͼ25% (42). In the present study, we
ity were not changed by diet (Table 6).
chose to compare a sucrose intake of 25%, which is a level
Metabolic profiles. Fasting plasma glucose, serum insu-
substantially above recommended intakes and a level
lin, and interstitial glucose levels over 24 h did not change
some guidelines consider may be detrimental to health,
with alteration of dietary sucrose content (Table 7). Total
with a 10% intake, which compares with the lowest
and LDL cholesterol were higher after 25% sucrose com-
recommended restriction, while keeping total carbohy-
pared with 10% sucrose. HDL cholesterol and fasting
triglycerides were similar on the two diets.
Evidence from animal studies has generally shown that
increased sucrose intake has a detrimental effect on
DISCUSSION
insulin sensitivity and cardiovascular risk factors. How-ever, the levels of sucrose intake in these studies, of up to
This study demonstrates that a high-sucrose diet, with 25%
60 –70% of dietary energy intake as sucrose or fructose,
of total energy intake from sucrose, has no detrimental
have generally been at a level that is nonphysiological and,for most human subjects, unpalatable. Furthermore, thediets studied were in many cases hypercaloric, makinginterpretation of the relative impact of sucrose intake andweight gain impossible (15). Human studies have pro-duced conflicting findings. Interventional studies haveshown variable effects on insulin sensitivity, and, in many,the method of assessing insulin resistance has been sub-optimal but the study period relatively short and thesample size small (43).
TABLE 4Intervention intakes of energy and macronutrients during thehigh- and low-sucrose diets
FIG. 1. Plasma glucose, serum insulin, and glucose infusion rates during euglycemic-hyperinsulinemic clamp. Data are means ؎ SE. SUCROSE, INSULIN RESISTANCE, AND VASCULAR RISK
TABLE 5Serum nonesterified fatty acid levels at basal state and afterlow-dose insulin infusion (0.4 mU ⅐ kgϪ1 ⅐ minϪ1) plateau at90 –120 min and high-dose insulin infusion (2.0 mU ⅐ kgϪ1 ⅐minϪ1) plateau at 210 –240 min
Data are means Ϯ SE. NS, not significant.
A strength of the present study is the randomized
controlled design and rigorous dietetic supervision. Due to
FIG. 3. Peripheral glucose uptake during euglycemic-hyperinsulinemic
the wide interindividual but low intraindividual variation
clamp. Data are means ؎ SE.
in the degree of insulin resistance in normal subjects, atwo-period crossover design separated by a washout pe-
between the two dietary periods. The study was powered
riod was chosen with each subject acting as their own
to exclude a 10% difference in insulin action, which is a
control (44). The 6 weeks of dietary intervention per
level assumed likely to have a clinically relevant impact.
assessment period compares favorably with other relevant
The results in fact showed a trend toward an increase in
human studies; however, it is not possible to predict the
insulin sensitivity with the high-sucrose diet, although this
effect of a high-sucrose intake over a more prolonged
was not statistically significant. No plausible biological
period. Although it is impossible to measure compliance
mechanism exists to explain why a high-sucrose diet might
with the diets under study, volunteers were reviewed
improve insulin sensitivity, and it is likely that this finding
every 2–3 days throughout the dietary periods and were
is due to chance. Furthermore, we found no difference in
questioned regarding palatability and compliance with the
fasting levels of serum nonesterified fatty acid concentra-
food that was provided for the duration of the study. In
tions during the dietary periods and a comparable degree
addition, the absence of any change in weight is further
of suppression during hyperinsulinemia, indicating no
evidence of careful dietary planning and supervision.
detrimental effect on adipose tissue insulin action.
The primary outcome measure of insulin resistance was
The premise of this study is that a high-sucrose diet may
assessed using the reference standard technique of the
alter the risk of type 2 diabetes and cardiovascular dis-
hyperinsulinemic-isoglycemic clamp combined with iso-
ease. Although the primary outcome of the study was
tope dilution techniques. The sensitivity to insulin varies
assessment of insulin resistance, a feature of both condi-
widely in different insulin-responsive tissues, and abnor-
tions, it is possible that other mechanisms may link
malities of these responses may occur separately in insu-
high-sucrose intake to cardiovascular disease. We also
lin-resistant states. There was no significant effect of
used the noninvasive technique of pulse-wave analysis to
altering dietary sucrose content on either fasting hepatic
assess arterial stiffness, which is increasingly being recog-
glucose production or its suppression during low-dose
nized as an important determinant of cardiovascular risk
insulin infusion, which are both measures of hepatic
(45). Stiffening of the arterial tree increases the velocity
insulin action. This result suggests no abnormality of
and amplitude of reflected pulse waves from the periph-
hepatic insulin action, which is recognized to be an early
ery, with the result that larger waves return to the aorta
feature of type 2 diabetes (3). The high-dose insulininfusion results in maximally stimulated glucose uptake
and reflects skeletal muscle or peripheral insulin sensitiv-
Effect of sucrose diets on metabolic variables
ity. We found no difference in peripheral insulin resistance
Effect of sucrose diets on hemodynamic variables
Data are means Ϯ SE or median (interquartile range). NS, not
Data are means Ϯ SE. NS, not significant. R.N.A. BLACK AND ASSOCIATES
earlier. This augments central systolic pressure, which
subjects compared with a low-sucrose diet. These results
increases left ventricular workload and, thus, myocardial
suggest that important pathogenic processes that precede
oxygen demand. In the present study, we found no differ-
diabetes and vascular disease are not significantly wor-
ence in markers of arterial stiffness, such as augmentation
sened by sucrose itself. These findings should be incorpo-
pressure/index, time to reflectance, or brachial pulse-wave
rated in dietary guidelines for the prevention of diabetes
velocity. It should be noted that this study was powered
and cardiovascular disease. It is likely that other dietary
for the primary outcome of insulin sensitivity; although in
factors, such as caloric excess, and lifestyle factors, such
a smaller cohort, we have previously shown (39) that
as physical inactivity and weight gain, may be more
acute elevation of plasma glucose is associated with
important determinants of insulin action than carbohy-
significant adverse changes on pulse-wave analysis. In this
drate type. The results of this study cannot be extrapo-
study, continuous monitoring of interstitial glucose levels
using a continuous glucose monitoring system showed no
information regarding the impact of severe restriction of
difference in 24-h or postprandial glycemic exposure.
sucrose intake in low-carbohydrate weight-reduction diets
A rise in total and LDL cholesterol and a trend toward
increased triglycerides were observed during the 25%sucrose diet compared with the 10% sucrose diet. Al-
ACKNOWLEDGMENTS
though the mean changes were relatively modest and
This study was supported by an unrestricted research
levels remained within normal ranges, it is possible that
grant from The Sugar Bureau and Suikerstichting, the
more marked abnormalities could arise in subjects with
Netherlands. R.N.A.B. was in receipt of an R&D Fellow-
hyperlipidemia at baseline. Other studies have demon-
ship from the Northern Ireland Department of Health and
strated increased triglyceride levels with sucrose contents
Social Services Research and Development Office.
20%; however, the LDL increase is more unusual (46). A
We are grateful to Dr. C. Patterson, The Queen’s Univer-
similar change in lipoprotein profiles has been noted in
sity of Belfast, for statistical advice, to Dr. C. Mercer,
high-fructose diets in man (47). Fructose is the more
Department of Medicine, The Queen’s University of Bel-
lipogenic component, as it bypasses a major rate-control-
fast, for carrying out nonesterified fatty acid assays, and to
ling step in glycolysis (48). The food selection that was
Mr. Brian Sheridan and the staff at Belfast Link Laborato-
necessary to achieve the balance resulted in a change in
ries for carrying out insulin and C-peptide assays.
fat quality but no change in total fat quantity. The high-sucrose diet had 29% higher energy content from saturatedfat and 29% lower polyunsaturated fat than the low-
REFERENCES
sucrose diet. We hypothesize that this alteration in satu-
1. Perry IJ, Wannamethee SG, Shaper AG, Alberti KG: Serum true insulin
rated fat intake may have contributed to the rise in LDL
concentration and the risk of clinical non-insulin dependent diabetes
cholesterol rather than by a direct effect of sucrose.
during long-term follow-up. Int J Epidemiol 28:735–741, 1999
2. Hunter SJ, Garvey WT: Insulin action and insulin resistance: diseases
An important limitation of this study must be recog-
involving defects in insulin receptors, signal transduction, and the glucose
nized. The subjects were a defined group without signifi-
transport effector system. Am J Med 105:331–345, 1998
cant metabolic or clinical abnormality. They were of male
3. Ferrannini E: Insulin resistance versus insulin deficiency in non-insulin-
sex, white Western-European origin, relatively young (on
dependent diabetes mellitus: problems and prospects. Endocr Rev 19:477–
average), and did not have diabetes or significant hyper-
lipidemia. All these factors can alter baseline insulin
4. Despres JP, Lamarche B, Mauriege P, Cantin B, Dagenais GR, Moorjani S,
Lupien PJ: Hyperinsulinemia as an independent risk factor for ischemic
sensitivity and may influence interventional responses. In
heart disease. N Engl J Med 334:952–957, 1996
addition, the caloric intakes were controlled rather than
5. Lakka HM, Lakka TA, Tuomilehto J, Sivenius J, Salonen JT: Hyperinsulin-
ad libitum to allow conclusions to be drawn regarding
emia and the risk of cardiovascular death and acute coronary and
carbohydrate quality itself rather than the complicating
cerebrovascular events in men: the Kuopio Ischaemic Heart Disease Risk
factor of differing energy intakes and balances. Outside
Factor Study. Arch Intern Med 160:1160 –1168, 2000
such study conditions, differing diet quality could have
6. Yip J, Facchini FS, Reaven GM: Resistance to insulin-mediated glucose
disposal as a predictor of cardiovascular disease. J Clin Endocrinol Metab
differing effects on satiety and food intake, which may be
mediated via leptin and other adipokines, and could result
7. World Health Organisation. Diet, Nutrition and the Prevention of Chronic
in different energy intakes, balance, and weight change; all
Diseases: Report of a Joint WHO/FAO Expert Consultation. Geneva,
of which could impact insulin sensitivity (49). Certainly, in
World Health Org., 2002 (Tech. Rep. Ser., no. 916)
children, increased servings of sugar-sweetened drinks
8. Mann J: Free sugars and human health: sufficient evidence for action?
were associated with obesity in a prospective observa-
9. Hu FB, Willett WC: Optimal diets for prevention of coronary heart disease.
tional study (50). Furthermore, although 24-h glycemic
profiles and insulin clearance were similar on the high- and
10. Kromhout D, Menotti A, Kesteloot H, Sans S: Prevention of coronary heart
low-sucrose diets, we did not directly assess insulin secre-
disease by diet and lifestyle: evidence from prospective cross-cultural,
tion or postprandial metabolic changes. It is, however,
cohort, and intervention studies. Circulation 105:893– 898, 2002
possible that a high-sucrose diet could have detrimental
11. Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT, Hamalainen H, Ilanne-
effects on insulin secretion and postprandial glucose and
Parikka P, Keinanen-Kiukaanniemi S, Laakso M, Louheranta A, Rastas M,Salminen V, Aunola S, Cepaitis Z, Moltchanov V, Hakumaki M, Mannelin M,
lipid metabolism, particularly in established type 2 diabe-
Martikkala V, Sundvall J, Uusitupa M: Prevention of type 2 diabetes by
tes where these are recognized to be important features.
changes in lifestyle among subjects with impaired glucose tolerance.
The conclusions from these data regarding effects of a
N Engl J Med 344:1343–1350, 2004
high-sucrose diet on insulin secretion and postprandial
12. Diabetes Prevention Program Research Group: Reduction in the incidence
metabolism must therefore be limited to the described
of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med
healthy group taking an eucaloric diet.
13. Marshall JA, Hoag S, Shetterly S, Hamman RF: Dietary fat predicts
In conclusion, a high-sucrose intake as part of a bal-
conversion from impaired glucose tolerance to NIDDM. Diabetes Care
anced, eucaloric, weight-maintaining diet had no detrimen-
tal effect on insulin sensitivity in healthy nondiabetic
14. Hodge AM, Montgomery J, Dowse GK, Mavo B, Watt T, Zimmet PZ: A
SUCROSE, INSULIN RESISTANCE, AND VASCULAR RISK
case-control study of diet in newly diagnosed NIDDM in the Wanigela
diabetic plasma and decreased biological activity assessed by euglycemic-
people of Papua New Guinea. Diabetes Care 19:457– 462, 1996
hyperinsulinemic clamp technique in humans. Diabetes 52:492– 498, 2003
15. Storlien LH, Higgins JA, Thomas TC, Brown MA, Wang HQ, Huang XF, Else
32. Somogyi M: Determination of blood sugar. J Biol Chem 160:69 –73, 1945
PL: Diet composition and insulin action in animal models. Br J Nutr 83
33. Steele R, Wall JS, De Bodo RC, Altszuler N: Measurement of size and
turnover rate of body glucose pool by the isotope dilution method. Am J
16. McClenaghan NH: Determining the relationship between dietary carbohy-
drate intake and insulin resistance. Nutr Res Rev 18:222–240, 2005
34. De Bodo RC, Steele R, Altszuler N, Dunn A, Bishop JS: On the hormonal
17. Kiens B, Richter EA: Types of carbohydrate in an ordinary diet affect
regulation of carbohydrate metabolism: studies with C14 glucose. Recent
insulin action and muscle substrates in humans. Am J Clin Nutr 63:47–53,
35. Wilkinson IB, Fuchs SA, Jansen IM, Spratt JC, Murray GD, Cockcroft JR,
18. Colagiuri S, Miller JJ, Edwards RA: Metabolic effects of adding sucrose and
Webb DJ: Reproducibility of pulse wave velocity and augmentation index
aspartame to the diet of subjects with noninsulin-dependent diabetes
measured by pulse wave analysis. J Hypertens 16:2079 –2084, 1998
mellitus. Am J Clin Nutr 50:474 – 478, 1989
36. Filipovsky J, Svobodova V, Pecen L: Reproducibility of radial pulse wave
19. Thorburn AW, Crapo PA, Griver K, Wallace P, Henry RR: Long-terms
analysis in healthy subjects. J Hypertens 18:1033–1040, 2000
37. Wilkinson IB, Cockcroft JR, Webb DJ: Pulse wave analysis and arterial
effects of dietary fructose on carbohydrate metabolism in non-insulin–
stiffness. J Cardiovasc Pharmacol 32 (Suppl. 3):S33–S37, 1998
dependent diabetes mellitus. Metabolism 39:58 – 63, 1990
38. Marchais SJ, Guerin AP, Pannier BM, Levy BI, Safar ME, London GM: Wave
20. Koivisto VA, Yki-Yarvinen H: Fructose and insulin sensitivity in patients
reflections and cardiac hypertrophy in chronic uremia: influence of body
with type 2 diabetes. J Intern Med 233:145–153, 1993
size. Hypertension 22:876 – 883, 1993
21. Sheard NF, Clark NG, Brand-Miller JC, Franz MJ, Pi-Sunyer FX, Mayer-
39. Mullan BA, Ennis CN, Fee HJ, Young IS, McCance DR: Protective effects of
Davis E, Kulkarni K, Geil P: Dietary carbohydrate (amount and type) in the
ascorbic acid on arterial hemodynamics during acute hyperglycemia. Am J
prevention and management of diabetes: a statement by the American
Physiol Heart Circ Physiol 287:H1262–H1268, 2004
Diabetes Association. Diabetes Care 27:2266 –2271, 2004
40. Hills M, Armitage P: The two-period cross-over clinical trial. Br J Clin
22. Lara-Castro C, Garvey WT: Diet, insulin resistance, and obesity: zoning in
on data for Atkins’ dieters living in south beach. J Clin Endocrinol Metab
41. Henderson L, Gregory J: The National Diet and Nutrition Survey ofAdults Aged 19 – 64 Years. Volume 1: Types and Quantities of Food
23. Astrup A, Meinert Larsen T, Harper A: Atkins and other low-carbohydrate
diets: hoax or and effective tool for weight loss? Lancet 364:897– 899, 1994
42. Murphy SP, Johnson RK: The scientific basis of recent US guidance on
24. Hodge AM, English DR, O’Dea K, Giles GG: Glycemic index and dietary
sugars intake. Am J Clin Nutr 78:827S– 833S, 2003
fiber and the risk of type 2 diabetes. Diabetes Care 27:2701–2706, 2004
43. Daly ME, Vale C, Walker M, Alberti KG, Mathers JC: Dietary carbohydrates
25. Meyer KA, Kushi LH, Jacobs DR, Slavin J, Sellers TA, Folsom AR:
and insulin sensitivity: a review of the evidence and clinical implications.
Carbohydrates, dietary fibre, and incident type 2 diabetes in older women. Am J Clin Nutr 66:1072–1085, 1997
44. Yeni-Komshian H, Carantoni M, Abbasi F, Reaven GM: Relationship
26. Salmeron J, Ascherio A, Rimm EB, Colditz GA, Spiegelman D, Jenkins DJ,
between several surrogate measures of insulin resistance and quantifica-
Stampfer MJ, Wing AL, Willett WC: Dietary fiber, glycemic load, and risk of
tion of insulin-mediated glucose disposal in 490 healthy nondiabetic
NIDDM in men. Diabetes Care 20:545–550, 1997
volunteers. Diabetes Care 23:171–175, 2000
27. Food and Agriculture Organization of the United Nations, World Health
45. Arnett DK, Evans GW, Riley WA: Arterial stiffness: a new cardiovascular
Organization: Carbohydrates in Human Nutrition: Report of a Joint
risk factor? Am J Epidemiol 140:669 – 682, 1994
FAO/WHO Expert Consultation. Rome, Food and Agriculture Organiza-
46. Parks EJ, Hellerstein MK: Carbohydrate-induced hypertriacylglycerolemia:
tion, 1998 (FAO Food and Nutrition Paper 66)
historical perspective and review of biological mechanisms. Am J Clin
28. Howard BV, Wylie-Rosett J: Sugar and cardiovascular disease: a statement
for healthcare professionals from the committee on nutrition of the
47. Bantle JP, Raatz SK, Thomas W, Georgopoulos A: Effects of dietary
council on nutrition, physical activity, and metabolism of the American
fructose on plasma lipids in healthy subjects. Am J Clin Nutr 72:1128 –
Heart Association. Circulation 106:523–527, 2002
29. Department of Health: Choosing Health? Choosing a Better Diet. A
48. Frayn KN, Kingman SM: Dietary sugars and lipid metabolism in humans. Consultation on Priorities for a Food and Health Action Plan. London,
Am J Clin Nutr 62 (Suppl. 1):250S–261S, 1995
49. Harvey Anderson G, Woodhead D: Consumption of sugars and the regula-
30. Scholfield WN: Predicting basal metabolic rate, new standards and review
tion of short-term satiety and food intake. Am J Clin Nutr 78 (Suppl.):
of previous work. Hum Nutr Clin Nutr 39(Suppl. 1):5– 41, 1985
31. Hunter SJ, Boyd AC, O’Harte FP, McKillop AM, Wiggam MI, Mooney MH,
50. Ludwig DS, Peterson KE, Gortmaker SL: Relation between consumption of
McCluskey JT, Lindsay JR, Ennis CN, Gamble R, Sheridan B, Barnett CR,
sugar-sweetened drinks and childhood obesity: a prospective, observa-
McNulty H, Bell PM, Flatt PR: Demonstration of glycated insulin in human
tional analysis. Lancet 357:505–508, 2001
Babette Bensoussan, The MindShifts Groupand Craig Fleisher, University of Windsor Since writing our book Strategic and structure analysis truly tweaked management’s Competitive Analysis – Methods and Techniques for attention. Porter’s approach was the first popular Analyzing Business Competition , we have often beenforay into using industrial economic theory as anasked to identify t
Arthritis & Rheumatology Clinics of KansasPATIENT EDUCATION SYSTEMIC LUPUS ERYTHEMATOSUS Introduction: There is perhaps no rheumatic disease that evokes so much fear and confusion among both patients and health care providers as SLE. Difficult to diagnose, evaluate, and manage, SLE is an illness that may result in a wide variety of complications, ranging from bothersome arthritis, ras
 R.N.A. BLACK AND ASSOCIATES
R.N.A. BLACK AND ASSOCIATES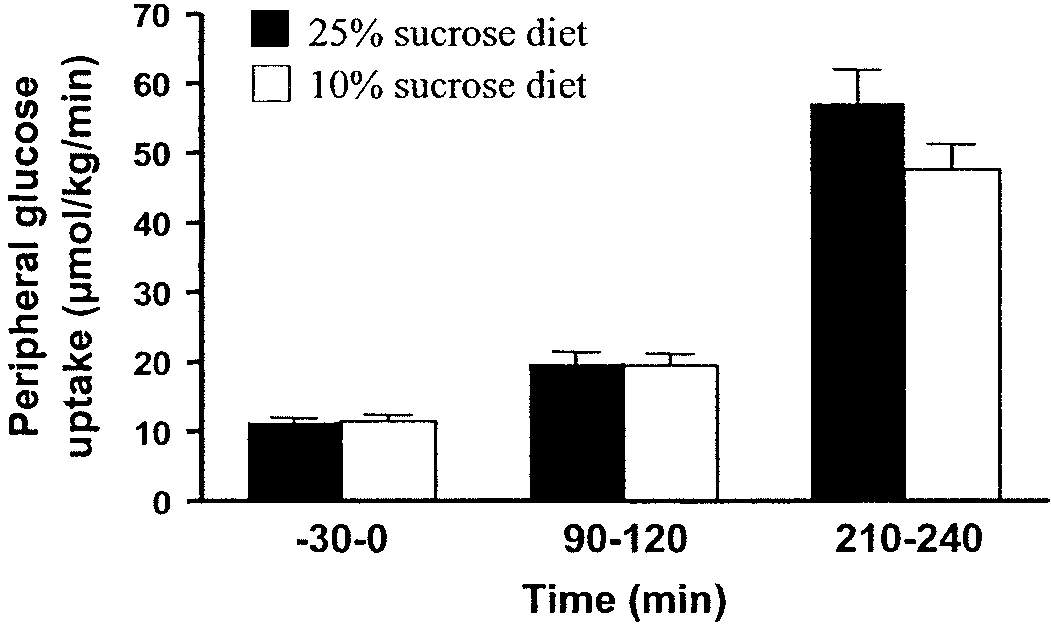 SUCROSE, INSULIN RESISTANCE, AND VASCULAR RISK
SUCROSE, INSULIN RESISTANCE, AND VASCULAR RISK