B R I T I S H J O U R N A L O F P S YC H I AT RY ( 2 0 0 7 ) , 1 9 1 ( s u p p l . 5 1 ) , s 9 6 ^ s 1 0 1 . d o i : 1 0 . 11 9 2 / b j p . 1 9 1 . 5 1 . s 9 6
medication in the previous 3 months; (f)change in dosage of any antidepressant
within 6 weeks, stimulant medication with-in 4 weeks, or mood stabiliser within 4
COPS are based on sub-threshold levelsof positive symptoms and operationally de-fine three prodromal
The prodromal phase of schizophrenic dis-
orders has been recognised since the 19th
century (Bleuler, 1911) and the possibility
detail elsewhere (Woods et al, 2001; Miller
to investigate methods to prevent progres-
et al, 2003a). Individuals were assessed to
dromal phase to frank psychosis (Falloon,
using the Structured Interview for Prodro-
mal Syndromes (SIPS; Miller et al, 1999).
Reliability of the COPS diagnosis of pos-
have focused on the acute treatment effects
on current symptoms (Woods et al, 2003).
using the SIPS (Miller et al, 2002, 2003a),
psychotic medication with limited liability
atic (Miller et al, 2003b), functionally im-
for weight gain (Marder et al, 2003), whose
paired (Miller et al, 2003b), cognitively
antipsychotics in that it is a partial agonist
treatment-seeking (Preda et al, 2002).
rather than a full antagonist at dopamine
overall goal of the present pilot study was
Participants were enrolled between October
the efficacy and safety of aripiprazole in
trial is registered with ClinicalTrials.gov
study at one site for 8 weeks, followed by
monthly follow-up visits to 52 weeks. Findings from the extension phase will be
assent with consent from a parent or guar-dian. Participants were included if they
were treatment-seeking out-patients of 13–
During the 1–2 weeks prior to beginning
40 years of age who met diagnostic criteria
for a possible prodromal syndrome. People
eligibility and neuropsychological examina-
reasons: (a) past or current DSM–IV criter-
ia (American Psychiatric Association, 1994)
for any lifetime psychotic disorder; (b) they
were judged clinically to have a psychiatric
ule. Initial doses were 5 mg/day aripipra-
disorder (e.g. mania, depression, attention-
zole; after 1 week, the dose was scheduled
deficit hyperactivity disorder) which could
for increase to 10 mg/day and after 2 weeks
to 15 mg/day, unless adverse effects dic-
tated a slower titration schedule. After the
as sequelae to drug or alcohol use; (d) alco-
there are a dearth of age-specific normative
data (our sample with test–retest data has a
a single daily dose unless there was a reason
mean age of 15.5 years, s.d.¼1.3), baseline
Spreen & Benton, 1969) test of phonemic
logical impairment similar to that observed
used to calculate the percentage adherence
managed initially by switching the timing
ministration of the Simpson–Angus Scale
by Spreen & Strauss (1998) and substan-
of the daily dose to bedtime or by dividing
(SAS; Simpson & Angus, 1970), the Barnes
tially better Trail-Making Part A and Part
B performances were reported for a healthy
by switching the timing of the daily dose
treat insomnia or agitation. Lorazepam or
adverse events (Systematic Assessment For
(EPS). Participants continued doses of anti-
cific inquiry method; Levine & Schooler,
depressant, mood stabiliser, or stimulant
1986), vital signs and weight. Treatment-
feeling medication was no longer needed.
were not permitted to begin or increase do-
cation and left the study primarily because
sage of these medications after consent.
of sedation after the first 10 mg dose, after
assessed at baseline and weekly thereafter.
having concluded that 5 mg was ineffective
ventions with supportive and psychoeduca-
For the present report, the time frame wasthe first 8 weeks after beginning study
Prescribed mean (s.d.) aripiprazole doses at
weeks 1, 2, 3, 4, 5, 6, 7 and 8 were 5 (0), 9(2), 11 (5), 11 (7), 11 (6), 13 (6), 14 (8), and
The primary efficacy measure for the analy-
measure was the SOPS total score. Analyses
sis of acute treatment was change over time
in the total score of the Scale of Prodromal
principle. All participants were included in
Symptoms (SOPS; Miller et al, 1999), a 19-
item scale with items scored 0–6. The inter-
30 mg/day (n¼1). Reported mean (s.d.) per-
rater reliability has been excellent (Miller et
likelihood-based repeated measures linear
al, 2003a). Factor analysis supports the val-
zole doses was 94 (13), 92 (22), 98 (4), 96
(8), 97 (7), 95 (10), 98 (5), and 94 (9) at
al, 2004b). Treatment response was defined
scores, using baseline scores as a covariate.
weeks 1, 2, 3, 4, 5, 6, 7 and 8 respectively.
For other measures we used t-test end-point
Schizophrenia (CDSS; Addington et al,1990), the Young Mania Rating Scale
(YMRS; Young et al, 1978), the Beck Anxi-
A total of 15 participants were enrolled.
ety Inventory (BAI; Beck et al, 1988), the
Demographic and treatment characteristics
at baseline are shown in Table 1. All were
and none also qualified for either of the
syndromes. All but two had never received
cluded tests of attention and working mem-
antipsychotic medication prior to partici-
pating. One participantt had received anti-
(CPT; Cornblatt et al, 1988), identical pairs
psychotic for 5 weeks 5 years earlier, and
version, letter number sequencing, N-back,
Trails A and B; Stroop Color Word Test for
before baseline, both for indications other
than psychosis. Scores for severity of illness
at baseline are shown in Table 2. Although
dose titration and prescribing anticholiner-
aripiprazole into the extension phase.
gic medication (2), slowing dose titration
and prescribing benzodiazepine (2) and pre-
then adding benzodiazepine (1). In the con-
working memory at the significant or trend
text of these management efforts, all parti-
three participants (20%) and anticholiner-
gic medication in 5 participants (33%).
number correct) but worsened on one other
akathisia remitted by the final evaluation
as a group on a test of executive function-
in six participants. Mean BAS total scores
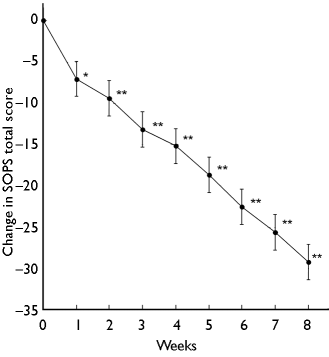
In the mixed-effects model, the effect of
end-point evaluation (Table 5). Four parti-
time for the SOPS total score change from
Scores on the remaining 15 tests of atten-
baseline was statistically significant (F
tion, working memory, executive function-
for akathisia at the 8-week evaluation.
SOPS total score was statistically signifi-
was observed for blood pressure (Table 5).
cant at each time point (Fig. 1). The LOCF
Pulse increased 6 beats per minute on aver-
analyses revealed that improvement on the
age. There were no significant differences
SOPS was statistically significant at end-
point for each of the positive, negative,
One participant discontinued aripiprazole
because of adverse events (sedation after 8
days). As determined by the SAFTEE, there
were few adverse events of more than mild
severity (Table 4). Complaints of adverse
and BAI scales, as well as significant func-
The principal finding of the present study
for only 8 days, at the final evaluation an
was that those meeting criteria for a schizo-
criteria (73%) at week 2 (n¼1), 3 (n¼2), 4
or greater severity was present in only one
(n¼1), 6 (n¼4), 7 (n¼1) and 8 (n¼2).
strated by increases from baseline on the
ever, are the small sample size and the use
course elected not to continue aripiprazole
of an uncontrolled, open-label design.
pression measures, was also more robust in
the open-label study of aripiprazole than
compared favourably with our previousexperience with olanzapine. Participants
whereas the aripiprazole mean weight gain
in this study was 1.2 kg (Table 5) despitebeing exposed to drug for a higher propor-tion of the 8 weeks. This degree of weight
prodromal for schizophrenia. Our findings
result of placebo effects or simply the pas-
can be compared with those from the acute
previous short-term studies of aripiprazole
but again one must allow for the different
study designs. Participants with established
problematic with aripiprazole than it had
schizophrenia improved less from baseline
rates of benztropine prescription. However,
expected two or three conversions without
dose titration or benzodiazepine prescrip-
whether this same effect of design occurs
tion, was effective in managing this adverse
effect, so that by the final evaluation the net
effect of treatment on akathisia ratings was
volunteering for a placebo-controlled study
relatively high in this short-term analysis
as measured by participant report at each
slightly more severely ill at baseline in the
visit. Adherence was similar to or higher
ledge to focus on an acute pharmacological
current sample according to the SOPS total
than with olanzapine in our masked study,
score, although GAF scores at baseline and
guidelines for initiation of aripiprazole inadolescents/children who weigh 50–70 kg(Findling et al, 2004).
Our current findings are relevant to discus-
sions of the ethics of intervention research
primarily focused on preventing the devel-
certainly an important goal, ethical issues
are raised because some participants will
be false-positives who have no personal op-portunity to benefit if benefit is defined so-
lely as prevention. The current data suggest
that people carrying a risk of progression topsychosis can receive not only the possi-bility of a preventive benefit but also a
treatment benefit ‘on average’ from inter-
adherence (Woods et al, 2003). As for most
studying prodromal v. chronic illness, or,
vention. The prospect of treatment benefit
studies, surreptitious non-adherence cannot
our use of a counterbalanced alternate form
on average is generally considered sufficient
be excluded. Future studies should continue
for the repeat verbal learning list, which
to justify exposure to some treatment risk
to assess adherence in this population.
in other illnesses. Thus the current data
measurement of new verbal learning by fa-
strengthen the argument that intervention
little consistent effect of aripiprazole over
miliarity with the word list carried over
8 weeks. Among the 20 results reported, a
from the baseline testing (practice effect;
few tests did show improvement, but others
Hawkins & Wexler, 1999; Hawkins et al,
showed a decline, with most suggesting lit-
2004c). In the previous study (Kern et al,
people who meet prodrome criteria benefit
2006) aripiprazole-treated participants im-
when prescribed aripiprazole, the present
proved but not significantly on an executive
results contribute to what is only the begin-
appeared to be little consistency in direc-
ning of the process of establishing a stand-
to ours with WCST perseverative errors.
size in our study was small and we had no
power to detect possible real effects; on
control group, placebo or otherwise. Future
placebo-controlled studies with more parti-
pected on the basis of prior test exposure.
cipants are needed before recommendations
can responsibly be made regarding routine
aripiprazole in the current study. Although
treatment. The present findings suggest that
aripiprazole is a promising candidate for
patients meeting prodrome criteria can be
examinations before and 8 weeks after ran-
are lower than those used in chronic schizo-
dom assignment to aripiprazole or olanza-
been used at too low a dose, especially in
the first month (McGlashan et al, 2006).
fluency and trail-making tasks. Our failure
In the present study we employed a recom-
mended fixed dose titration by the end of
measures could relate to our small sample
the second week to 15 mg/day, the minimal
or to our participants being less impaired
consistently effective aripiprazole dose for
and having less room to improve. Aripipra-
zole-treated participants improved signifi-
cantly in the previous study (Kern et al,
2006) on a verbal learning factor on which
schedule. The 15 mg/day dose was also that
loaded a test similar to our AVLT but with-
out use of alternative forms. Our failure to
schizophrenia (Brown et al, 2003). Initial
Elana Hayasaka, Our Bodies Ourselves (Boston, Massachusetts, USA) Korea Womenlink Forum on Biotechnology and Women’s Rights Thank you for inviting me to represent my organization at this forum. Building on the presentations of my colleagues, who have discussed many of the ethical, political, and moral concerns surrounding the practice of egg extraction, I will focus on the health risks to wom
Jeff Liker, Toyota Way, Sven Jirby 2005-11-29 Jeffrey Liker om THE TOYOTA WAY Jeffrey Liker är professor i industriell teknik vid University of Michigan, Ann Arbor. Han har studerat Toyotas produktionssystem i 20 år och publicerade år 2004 en best-seller: The Toyota Way. I denna beskriver han 14 principer som ligger till grund för Toyotas produktionsfilosofi, The Toyota Way. Den 14 nove
 there are a dearth of age-specific normative
data (our sample with test–retest data has a
a single daily dose unless there was a reason
mean age of 15.5 years, s.d.¼1.3), baseline
Spreen & Benton, 1969) test of phonemic
logical impairment similar to that observed
used to calculate the percentage adherence
managed initially by switching the timing
ministration of the Simpson–Angus Scale
by Spreen & Strauss (1998) and substan-
of the daily dose to bedtime or by dividing
(SAS; Simpson & Angus, 1970), the Barnes
tially better Trail-Making Part A and Part
B performances were reported for a healthy
by switching the timing of the daily dose
treat insomnia or agitation. Lorazepam or
adverse events (Systematic Assessment For
(EPS). Participants continued doses of anti-
cific inquiry method; Levine & Schooler,
depressant, mood stabiliser, or stimulant
1986), vital signs and weight. Treatment-
feeling medication was no longer needed.
there are a dearth of age-specific normative
data (our sample with test–retest data has a
a single daily dose unless there was a reason
mean age of 15.5 years, s.d.¼1.3), baseline
Spreen & Benton, 1969) test of phonemic
logical impairment similar to that observed
used to calculate the percentage adherence
managed initially by switching the timing
ministration of the Simpson–Angus Scale
by Spreen & Strauss (1998) and substan-
of the daily dose to bedtime or by dividing
(SAS; Simpson & Angus, 1970), the Barnes
tially better Trail-Making Part A and Part
B performances were reported for a healthy
by switching the timing of the daily dose
treat insomnia or agitation. Lorazepam or
adverse events (Systematic Assessment For
(EPS). Participants continued doses of anti-
cific inquiry method; Levine & Schooler,
depressant, mood stabiliser, or stimulant
1986), vital signs and weight. Treatment-
feeling medication was no longer needed.