(luteal phase defect, LH disorders, prolactin disorders, thyroid disorders, diabetes mellitus)
Systemic endocrine disorders are associated with a miscarriage rate of 29%. Except for diabetes mellitus, endocrine disorders are mainly responsible for first-semester miscarriages. This is due to the fact that foetal development until weeks 8-9 of pregnancy depends on the sufficiency of hormones in mother’s body and mainly progesterone levels.
After this period, placenta that is the main biological laboratory for the foetus, has developed and operates productively. Placenta works as a factory producing various substances, hormones included, making the foetus independent from its mother. The foetus now only needs and exploits its mother in order to receive structural elements that will help it grow until the end of pregnancy and as soon it is born its liver becomes its biological laboratory. Before a pregnancy starts or the soonest possible after it has started, hyperthyroidism, hypothyroidism and diabetes mellitus need to be regulated, as the woman must have normal glucose values and normal thyroid function (has to be euthyroid). Blood sugar tests include measuring blood glucose, glycosylated hemoglobin and blood glucose curve that has to appear normal. In case diabetes mellitus cannot be regulated with appropriate diet, insulin treatment is required.
If antithyroglobulin antibodies are present, maybe anti-ovarian antibodies are also present, resulting in a lack of progesterone for the first critical semester of pregnancy. Thyroid replacement treatment will be necessary only if there are signs of clinical hypothyroidism.
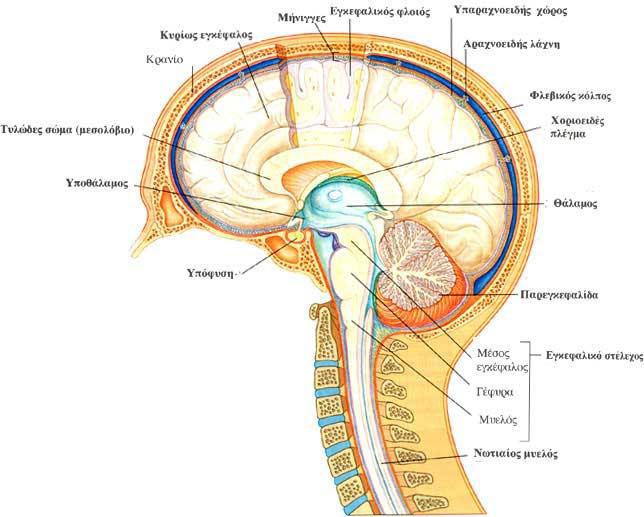
Hyperprolactinemia is also a usual cause. Prolactine is a hormone produced in the pituitary gland. Pituitary gland is at the base of the brain and resembles a nut hanging from its stem (pituitary stalk). It is an hormone acting in multiple ways, with the main one being production of milk from the mammary glands. Clinical manifestations include a reduction of the second half of a woman’s cycle or drops of blood several days before period or both. Hyperprolactinemia is also observed in women with polycystic ovarian syndrome. It can be treated with appropriate medication and in case of a pituitary microadenoma, medication will be necessary for the whole pregnancy period.
Corpus luteum deficiency is also one of the common findings in recurrent miscarriages examination. (Low progesterone levels during day 21 of the cycle (in a 28-days cycle) may provide for the diagnosis). Progesterone is given as treatment. During pregnancy, progesterone treatment continues until week 8 or week 10 the latest. Progesterone administration after week 10 is meaningless, as then placenta starts producing all necessary elements. According to references, progesterone administration in recurrent miscarriages seems to reduce their rate by 40%. High rates of recurrent miscarriages are observed in women with polycystic ovarian syndrome. High rates of androgens seem to interfere with normal development of endometrium that is necessary for the implantation and development of the fertilised ovum (egg).
Grupo Rangel renova certificação de qualidade CARGONEWS Pesquisa de notícias OK Grupo Rangel renova certificação de qualidade A SGS Portugal renovou recentemente a certificação do Sistema de Gestão de Qualidade às empresas Rangel Transitários, Rangel Expresso-FedEx e Eduardo Rangel Despachante Oficial, garantindo a conformidade dos seus processos internos e As renovações a
Gatorade Sports Science 60 Institute ® CAFFEINE AND EXERCISE PERFORMANCE Terry E. Graham, Ph.D. Lawrence L. Spriet, Ph.D. Department of Human Biology & Nutritional Sciences Member, GSSI Sports Medicine Review Board Department of Human Biology & Nutritional Sciences KEY POINTS 1. Recent, well-controlled studies have established that moderate doses of caffei
 HORMONAL FACTORS
HORMONAL FACTORS 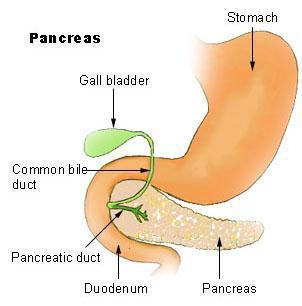
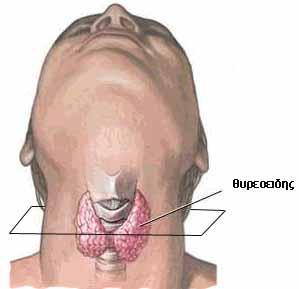 After this period, placenta that is the main biological laboratory for the foetus, has developed and operates productively. Placenta works as a factory producing various substances, hormones included, making the foetus independent from its mother. The foetus now only needs and exploits its mother in order to receive structural elements that will help it grow until the end of pregnancy and as soon it is born its liver becomes its biological laboratory. Before a pregnancy starts or the soonest possible after it has started, hyperthyroidism, hypothyroidism and diabetes mellitus need to be regulated, as the woman must have normal glucose values and normal thyroid function (has to be euthyroid). Blood sugar tests include measuring blood glucose, glycosylated hemoglobin and blood glucose curve that has to appear normal. In case diabetes mellitus cannot be regulated with appropriate diet, insulin treatment is required.
If antithyroglobulin antibodies are present, maybe anti-ovarian antibodies are also present, resulting in a lack of progesterone for the first critical semester of pregnancy. Thyroid replacement treatment will be necessary only if there are signs of clinical hypothyroidism.
After this period, placenta that is the main biological laboratory for the foetus, has developed and operates productively. Placenta works as a factory producing various substances, hormones included, making the foetus independent from its mother. The foetus now only needs and exploits its mother in order to receive structural elements that will help it grow until the end of pregnancy and as soon it is born its liver becomes its biological laboratory. Before a pregnancy starts or the soonest possible after it has started, hyperthyroidism, hypothyroidism and diabetes mellitus need to be regulated, as the woman must have normal glucose values and normal thyroid function (has to be euthyroid). Blood sugar tests include measuring blood glucose, glycosylated hemoglobin and blood glucose curve that has to appear normal. In case diabetes mellitus cannot be regulated with appropriate diet, insulin treatment is required.
If antithyroglobulin antibodies are present, maybe anti-ovarian antibodies are also present, resulting in a lack of progesterone for the first critical semester of pregnancy. Thyroid replacement treatment will be necessary only if there are signs of clinical hypothyroidism.
 Hyperprolactinemia is also a usual cause. Prolactine is a hormone produced in the pituitary gland. Pituitary gland is at the base of the brain and resembles a nut hanging from its stem (pituitary stalk). It is an hormone acting in multiple ways, with the main one being production of milk from the mammary glands. Clinical manifestations include a reduction of the second half of a woman’s cycle or drops of blood several days before period or both. Hyperprolactinemia is also observed in women with polycystic ovarian syndrome. It can be treated with appropriate medication and in case of a pituitary microadenoma, medication will be necessary for the whole pregnancy period.
Corpus luteum deficiency is also one of the common findings in recurrent miscarriages examination. (Low progesterone levels during day 21 of the cycle (in a 28-days cycle) may provide for the diagnosis). Progesterone is given as treatment. During pregnancy, progesterone treatment continues until week 8 or week 10 the latest. Progesterone administration after week 10 is meaningless, as then placenta starts producing all necessary elements. According to references, progesterone administration in recurrent miscarriages seems to reduce their rate by 40%. High rates of recurrent miscarriages are observed in women with polycystic ovarian syndrome. High rates of androgens seem to interfere with normal development of endometrium that is necessary for the implantation and development of the fertilised ovum (egg).
Hyperprolactinemia is also a usual cause. Prolactine is a hormone produced in the pituitary gland. Pituitary gland is at the base of the brain and resembles a nut hanging from its stem (pituitary stalk). It is an hormone acting in multiple ways, with the main one being production of milk from the mammary glands. Clinical manifestations include a reduction of the second half of a woman’s cycle or drops of blood several days before period or both. Hyperprolactinemia is also observed in women with polycystic ovarian syndrome. It can be treated with appropriate medication and in case of a pituitary microadenoma, medication will be necessary for the whole pregnancy period.
Corpus luteum deficiency is also one of the common findings in recurrent miscarriages examination. (Low progesterone levels during day 21 of the cycle (in a 28-days cycle) may provide for the diagnosis). Progesterone is given as treatment. During pregnancy, progesterone treatment continues until week 8 or week 10 the latest. Progesterone administration after week 10 is meaningless, as then placenta starts producing all necessary elements. According to references, progesterone administration in recurrent miscarriages seems to reduce their rate by 40%. High rates of recurrent miscarriages are observed in women with polycystic ovarian syndrome. High rates of androgens seem to interfere with normal development of endometrium that is necessary for the implantation and development of the fertilised ovum (egg).