Equoterapianet.com.br
& 2003 International Spinal Cord Society All rights reserved 1362-4393/03 $25.00
The short-term e’¼Ćect of hippotherapy on spasticity in patients with spinalcord injury
HE Lechner*,1, S Feldhaus2, L Gudmundsen2, D Hegemann2, D Michel2, GA Za┬©ch2 and H Knecht1
1Institute for Clinical Research, Swiss Paraplegic Centre, Nottwil, Switzerland; 2Swiss Paraplegic Centre,Nottwil, Switzerland
Study design: Assessment of spasticity before and after hippotherapy treatment.
Objective: To evaluate the short-term e’¼Ćect ofhippotherapy on spasticity ofspinal cord injuredpatients (SCIs).
Setting: Swiss Paraplegic Centre, Nottwil.
Methods: 32 patients with spinal cord injury with various degrees ofspasticity had repeatedsessions (mean 11) ofHippotherapy-Ks. Spasticity ofthe lower extremities was scoredaccording to the Ashworth Scale.
Results: In primary rehabilitation patients Ashworth values after hippotherapy weresigni’¼ücantly lower than before (WilcoxonŌĆÖs signed-rank test: Po0.001). Highest improvementswere observed in SCIs with very high spasticity. No signi’¼ücant di’¼Ćerence between short-terme’¼Ćect in paraplegic and short-term e’¼Ćect in tetraplegic subjects was found.
Conclusions: Hippotherapy signi’¼ücantly reduces spasticity oflower extremities in SCIs.
Spinal Cord (2003) 41, 502ŌĆō505. doi:10.1038/sj.sc.3101492
Keywords: hippotherapy; muscle spasticity; spinal cord injuries; rehabilitation; treatment
Spasticity is known as an accompanying phenomenon of
spasticity are even more scarce. Unlike therapeutic
spinal cord injuries and was de’¼üned by Lance1 as an
horseback riding, which teaches riding skills to indivi-
increased re’¼éex activity, as well as a velocity-dependent
duals with disabilities, hippotherapy is a neurophysio-
increase in muscle tone elicited by passive stretching.
logical treatment that uses the movement ofthe horse.
Not every patient su’¼Ćering from spasticity necessarily
The hypothesis is that the rhythmical side ’¼éexion and
requires treatment. However, depending on the severity
extension ofthe patientŌĆÖs trunk combined with trunk
ofspasticity it may interfere with activities ofdaily life.
torsion have a bene’¼ücial e’¼Ćect on spasticity. The
In the Stockholm spinal cord injury study,2 for example,
working mechanism ofhippotherapy on spasticity may
more than 41% ofsubjects with spastic paralysis
be complex. According to neurophysiological standards,
reported excessive spasticity associated with additional
an inhibition ofthe spasticity is achieved through the
functional impairment and/or pain, and 2/3 of the
saddle position in hip ’¼éexion ŌĆō abduction ŌĆō external
subjects with spastic paralysis took medication to treat
rotation as well as through rhythmical and three-
their spasticity.3 What other possibilities besides medi-
dimensional equine movements communicated to the
cation are there to reduce high muscle tone?
patientsŌĆÖ pelvis and trunk.6,7 A further impact on
For several years hippotherapy has been used in
spasticity is also attributed to the psychosomatical
rehabilitation ofspinal cord injured patients (SCIs) and
e’¼Ćects.5 According to Strauss8 hippotherapy gains its
positive e’¼Ćects on spasticity have been reported.4,5
unique e’¼Ćect through a neural facilitation, sensorimotor
Unfortunately, only few studies assessing the e’¼Ćect of
stimulation and psychosomatic in’¼éuence.
hippotherapy on spasticity have been conducted, and
We felt that there is a need for a study assessing the
most ofthe existing literature is not in the English
e’¼Ćect ofhippotherapy on spasticity ofSCIs and to
language. Studies that aim at explaining the mechanisms
report the result in the English language. We have tested
underlying the positive e’¼Ćect ofhippotherapy on
the short-term e’¼Ćect ofhippotherapy onto the increasedmuscle tone ofthe lower extremities in 32 SCIs asfollows: the physiotherapist in charge rated the spasti-
*Correspondence: HE Lechner, Institute for Clinical Research, SwissParaplegic Centre, Nottwil 6207, Switzerland
city ofthe patients directly prior to and af
Effect of hippotherapy on spasticity in SCIHE Lechner et al
hippotherapy treatment according to the Ashworth
On average each patient was tested prior and after 11(range: 5ŌĆō24) hippotherapy sessions. The treatmentswere performed according the concept of Hippotherapy-
Ks (HTK).11 The subject sat on a sheepskin (withoutsaddle), while the horse (Icelander) was led at walking
pace by a skilled equestrian. The physiotherapist walked
From June 1996 to November 1997 and from June 1999
beside the horse facilitating postural responses and
to May 2001 all patients with various degrees of
repositioning the patient ifnecessary. Some patients
spasticity were tested by the physiotherapists prior to
with high lesions needed a second physiotherapist sitting
and after hippotherapy treatment. Measurements were
on the horseback behind them for stabilisation. One
taken from 32 SCIs. The age ranged between 16 and 72
years (mean 37), four of the patients were female, 30subjects were inpatients in primary rehabilitation (timeafter injury between 1 and 18 months, mean 5), and two
were outpatients (4 and 6 years after injury). Levels of
Rating of spasticity was done directly before and after
the spinal cord injury were between C4 and T12 and
the hippotherapy session in the riding hall. The patient
between A and D according to the ŌĆśASIA Impairment
was lying on an examining table in supine position while
ScaleŌĆÖ10 (Table 1). Informed consent of all patients was
eight movement directions were rated: hip ’¼éexion and
obtained according to the Helsinki protocol.
extension, abduction and adduction, knee ’¼éexion and
Effect of hippotherapy on spasticity in SCI
extension, as well as ankle dorsi- and plantar’¼éexion. Thephysiotherapist moved the limb in the directions asquickly as possible. The knees and the ankles weremeasured with extended hips, while the lower legsdangling o’¼Ć the end ofthe testing bed. Each directionwas repeated three to ’¼üve times. She rated the elicitedspasticity according to the Ashworth Scale between 1and 5 (Ashworth-value, ASV) (Table 2). The ASV oftheeight movement directions ofboth sides were recordedas a sum of16 scores ranging from a minimum of16 to amaximum of80.
Testing was performed prior to and after the HTK
treatment by the same physiotherapist. Seven di’¼Ćerentphysiotherapists performed the overall testing of the 32patients. All seven physiotherapists were instructed onthe testing by the same person and met on a regularbasis to exchange testing experiences and to check inter-and intrarater reliability.
Scatterplot ofthe 32 subjects: means ofsums of
For each patient and examination sums ofthe ASV
ASV before versus sums of ASV after HTK treatment. The 451
from all directions on both sides were calculated (2 Â 8
line indicates values ofno change. All measured values show
movement directions, minimum score ┬╝ 16, maximum
smaller sums of ASV after than before HTK treatment. Note:
score ┬╝ 80). Means and standard deviations were
score of16 signi’¼ües a patient with no spasticity
calculated ofthe repeated HTK treatments f
patient. The existence ofa statistical di’¼Ćerence between
the ASV before and after HTK treatment was assessed
(X10.0) was observed in six patients with severe
by performing WilcoxonŌĆÖs signed-rank test. Statistical
before-session spasticity (ASV over 38).
signi’¼ücance12 was set at the 5% level.
There was no signi’¼ücant di’¼Ćerence between short-term
e’¼Ćect in paraplegic subjects and the short-term e’¼Ćect
in tetraplegic subjects (WilcoxonŌĆÖs signed rank test:P ┬╝ 0.4). The mean ofall di’¼Ćerences between before- and
A total of351 hippotherapy treatments were performed
after-session values for paraplegic subjects (n ┬╝ 18) was
and 327 ofthese sessions (93%) lead to a lower ASV
├Ć3.4 (SD72.2) and for all tetraplegic subjects (n ┬╝ 14) it
immediately after as compared than before the sessions.
was ├Ć2.8 (SD71.0). There was no longitudinal e’¼Ćect
In all, 20 sessions (6%) did not lead to a change in the
(downward trend overall sessions in each patient) and
ASV score; these sessions were completed by 10 patients
the variance within the before-session values in each
with low ASV (p24) prior to treatment. In only two
single patient ranged from 0.81 to 77.4 (SD70.9ŌĆō78.8).
patients with very low ASV (p18) an increase ofthe
Also, there was no detectable trend ofthe before- and
value was measured twice in each patient (1%).
after-session di’¼Ćerences (data not shown).
Hippotherapy led to a substantial decrease ofmuscle
tone in the lower extremities ofthe 32 SCI patients. Thecalculated means ofall individual patients ranged from
17.6 to 53.3 prior to treatment and from 16.6 to 42 after
Our results show that hippotherapy causes an immediate
treatment (Table 1). Group scores after the treatment
reduction ofspasticity ofthe lower extremities ofSCI
were signi’¼ücantly lower than group scores before
patients. The ASV was signi’¼ücantly lower after the
treatment than before. The greatest before- and after-session di’¼Ćerences were measured in patients with very
Hippotherapy and its reducing e’¼Ćect on the muscle
tone was described earlier in connection with otherclinical entities associated with spasticity such as multi-
ple sclerosis (MS) and cerebral palsy (CP): in the ŌĆśSwiss
Slight increase in tone giving a ŌĆścatchŌĆÖ when the limb
StudyŌĆÖ by Kuenzle and Wuethrich13 including 255
patients with MS, relaxation and decrease in muscle
More marked increase in tone but limb easily ’¼éexed
tone was the most frequent e’¼Ćect of hippotherapy,
Considerable increase in tone ŌĆō passive movement
according to subjective records ofpatients, therapists
and treating doctors. However, these results were not
backed up by Ashworth Scale. In another study with
Effect of hippotherapy on spasticity in SCIHE Lechner et al
MS patients, a reduction in the muscle tone ofthe lower
valuable supplement to the conventional physiotherapy
extremities after hippotherapy was measured by electro-
approach in holistic rehabilitation ofSCIs.
Tarnow15 ascertained that children and teenagers with
a spastic quadriplegia had shown a clear improvement
We thank all the subjects who participated in the study and we
in their trunk ’¼éexibility and their functional ability after
gratefully acknowledge the ’¼ünancial support of the Swiss
treatment with hippotherapy. She attributed the results
to a decrease in muscle tone as a result ofthis treatment.
McGibbon et al16 described a standardised protocol ofhippotherapy treatment and documented its e’¼Ćect on
gait, energy expenditure, and gross motor function inchildren with spastic CP. Bertoti6 examined the e’¼Ćect of
1 Lance JW. Symposium synopsis. In: Feldman RG, Young
RR, Koulla WP (eds). Spasticity: Disordered Motor Control.
hippotherapy on the posture ofchildren with CP and
Yearbook Medical Publishers: Chicago 1980, pp 485ŌĆō494.
described improved posture because ofthe hippother-
2 Levi R, Hultling C, Nash MS, Seiger A. The Stockholm
apyŌĆÖs reducing e’¼Ćect on spasticity. Exner et al4 described
Spinal Cord Injury Study: 1. Medical problems in a
a ŌĆśclear suppression ofthe spasticityŌĆÖ with a ŌĆśremarkable
regional SCI population. Paraplegia 1995; 33: 308ŌĆō315.
duration ofe’¼ĆectŌĆÖ; however, the degree ofthe decrease
3 Skold C, Levi R, Ake S. Spasticity after traumatic spinal
in spasticity was not stated quantitatively.
cord injury: nature, severity and location. Arch Phys Med
In our study, the spasticity was rated according to the
ASV directly prior and after treatment in primary
4 Exner G, Engelmann A, Lange K, Wenck B. Grundlagen
rehabilitation patients. Our results represent a short-
und Wirkung der Hippotherapie im Konzept der umfas-
term e’¼Ćect ofhippotherapy. However, it would be
interesting to quantitatively evaluate the duration ofthe
5 Hegemann D, Za┬©ch G. Hippotherapie zur Behandlung der
e’¼Ćect as well as a possibly persisting e’¼Ćect in the context
Spastizita┬©t bei Para- und Tetraplegikern (German). In:
urther prospective study, since in the ŌĆśSwiss
Grueninger W (ed). Spinale Spastik. Ueberreuter Verlag:
StudyŌĆÖ13 in over 70% ofMS patients a bene’¼üt of2 days
6 Bertoti DB. E’¼Ćect oftherapeutic horseback riding on
Naturally, medication would have to be kept constant
posture in children with cerebral palsy. Phys Ther 1988;
ifchanges in the severity ofspasticity over a series of
hippotherapy sessions were to be investigated. This
7 Wuethrich R, Kuenzle U. Hippothe┬┤rapie chez des patients
would have to be conducted with chronic SCIs, as
atteints de scle┬┤rose en plaques. J Beige Med Phys Rehabil
during ’¼ürst rehabilitation there are many more con-
8 Strauss I. Hippotherapy: Neurophysiological Therapy on the
founding factors like psychological stress, bladder
Horse. Ontario Therapeutic Riding Association: Thornhill,
infections or bowel complications, changes of therapies
9 Ashworth B. Preliminary trial ofcarisoprodol in multiple
have an e’¼Ćect on muscle tone. To evidence a long-
sclerosis. Practitioner 1964; 192: 540ŌĆō542.
itudinal e’¼Ćect ofhippotherapy on spasticity, we just
10 Maynard FMJ et al. International standards for neurolo-
started a blinded long-time prospective study on chronic
gical and functional classi’¼ücation of spinal cord injury.
SCIs with stable antispastic medication, who are at least
American Spinal Injury Association. Spinal Cord 1997;
Regarding the rating ofmuscle tone with the Ash-
11 Kuenzle U. Hippotherapie auf den Grundlagen der Funktio-
worth Scale, it needs to be mentioned that it is clearly a
nellen Bewegungslehre Klein-Vogelbach. Hippotherapie-K:Theorie, Praktische Anwendung Wirksamkeitsnachweis.
subjective method. Additionally, the physiotherapist
Springer-Verlag: Berlin Heidelberg, 2000.
conducting the measurement was not blinded to the
12 Sheskin DJ. Handbook of Parametric and Nonparametric
treatment and ratings may have been in’¼éuenced by
Statistical Procedures. 2nd edn. Chapman & Hall/CRC
13 Kuenzle U, Wuethrich R. Schweizerische Studie u┬©ber die
Wirksamkeit der Hippotherapie K bei Multiple-Sklerose-
Patienten. In: Kuenzle U (ed). Hippotherapie auf denGrundlagen der Funktionellen Bewegungslehre Klein-Vogel-
We show that hippotherapy has an alleviating short-
bach. Springer-Verlag: Berlin, Heidelberg 2000, pp 359ŌĆō381.
term e’¼Ćect on spasticity ofthe lower extremities in SCI
14 Weber A. Hippotherapie bei Multiple-Sklerose-Kranken.
patients. In 32 patients such an e’¼Ćect could be shown
with the help ofthe Ashworth Scale. There was a
15 Tarnow A. Hippotherapeutische Behandlungsergebnisse ŌĆō
signi’¼ücant di’¼Ćerence between the spasticity before and
(German). Oe’¼Ć Gesundh Wesen 1979; 41: 201ŌĆō205.
16 McGibbon NH, Andrade CK, Widener G, Cintas HL.
Further studies regarding the duration ofthe e’¼Ćect
E’¼Ćect ofan equine-movement therapy program on gait,
are necessary and will be performed with blinded
energy expenditure, and motor function in children with
assessment ofspasticity reduction, comparing it with
spastic cerebral palsy: a pilot study. DevMed Child Neurol
other interventions. In summary, hippotherapy is a
Source: http://www.equoterapianet.com.br/Fisioterapia/the_short-term_effect_of_hippotherapy_on_spasticity.pdf
Welcome to Maternal/Child/Psych Nursing! The purpose of the 20-point quiz is to review previous math skills and prepare the student for math skills needed during the 201 clinical rotations. The math questions on the quiz will be VERY similar to the following examples. Please spend time reviewing your math before the quiz is given during the first week of the semester. There are 20 questions
INFORMACION PARA PRESCRIBIR AMPLIA Nombre Comercial: ANUAR ASF┬« Nombre Gen├®rico: CABERGOLINA Forma Farmac├®utica y Formulaci├│n: Comprimidos. Cabergolina. 0.5 mg Excipiente cbpŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”ŌĆ”. 1 comprimido Indicaciones Terap├®uticas: Inhibidor de la secreci├│n de prolactina (PRL), Agonista dopamin├®rgico. ANUAR ASF┬
A |
B |
C |
D |
E |
F |
G |
H |
I |
J |
K |
L |
M |
N |
O |
P |
Q |
R |
S |
T |
U |
V |
W |
X |
Y |
Z |
0-9 |
 & 2003 International Spinal Cord Society All rights reserved 1362-4393/03 $25.00
The short-term e’¼Ćect of hippotherapy on spasticity in patients with spinalcord injury
HE Lechner*,1, S Feldhaus2, L Gudmundsen2, D Hegemann2, D Michel2, GA Za┬©ch2 and H Knecht1
1Institute for Clinical Research, Swiss Paraplegic Centre, Nottwil, Switzerland; 2Swiss Paraplegic Centre,Nottwil, Switzerland
Study design: Assessment of spasticity before and after hippotherapy treatment.
& 2003 International Spinal Cord Society All rights reserved 1362-4393/03 $25.00
The short-term e’¼Ćect of hippotherapy on spasticity in patients with spinalcord injury
HE Lechner*,1, S Feldhaus2, L Gudmundsen2, D Hegemann2, D Michel2, GA Za┬©ch2 and H Knecht1
1Institute for Clinical Research, Swiss Paraplegic Centre, Nottwil, Switzerland; 2Swiss Paraplegic Centre,Nottwil, Switzerland
Study design: Assessment of spasticity before and after hippotherapy treatment. Effect of hippotherapy on spasticity in SCIHE Lechner et al
hippotherapy treatment according to the Ashworth
On average each patient was tested prior and after 11(range: 5ŌĆō24) hippotherapy sessions. The treatmentswere performed according the concept of Hippotherapy-
Ks (HTK).11 The subject sat on a sheepskin (withoutsaddle), while the horse (Icelander) was led at walking
pace by a skilled equestrian. The physiotherapist walked
From June 1996 to November 1997 and from June 1999
beside the horse facilitating postural responses and
to May 2001 all patients with various degrees of
repositioning the patient ifnecessary. Some patients
spasticity were tested by the physiotherapists prior to
with high lesions needed a second physiotherapist sitting
and after hippotherapy treatment. Measurements were
on the horseback behind them for stabilisation. One
taken from 32 SCIs. The age ranged between 16 and 72
years (mean 37), four of the patients were female, 30subjects were inpatients in primary rehabilitation (timeafter injury between 1 and 18 months, mean 5), and two
were outpatients (4 and 6 years after injury). Levels of
Rating of spasticity was done directly before and after
the spinal cord injury were between C4 and T12 and
the hippotherapy session in the riding hall. The patient
between A and D according to the ŌĆśASIA Impairment
was lying on an examining table in supine position while
ScaleŌĆÖ10 (Table 1). Informed consent of all patients was
eight movement directions were rated: hip ’¼éexion and
obtained according to the Helsinki protocol.
Effect of hippotherapy on spasticity in SCIHE Lechner et al
hippotherapy treatment according to the Ashworth
On average each patient was tested prior and after 11(range: 5ŌĆō24) hippotherapy sessions. The treatmentswere performed according the concept of Hippotherapy-
Ks (HTK).11 The subject sat on a sheepskin (withoutsaddle), while the horse (Icelander) was led at walking
pace by a skilled equestrian. The physiotherapist walked
From June 1996 to November 1997 and from June 1999
beside the horse facilitating postural responses and
to May 2001 all patients with various degrees of
repositioning the patient ifnecessary. Some patients
spasticity were tested by the physiotherapists prior to
with high lesions needed a second physiotherapist sitting
and after hippotherapy treatment. Measurements were
on the horseback behind them for stabilisation. One
taken from 32 SCIs. The age ranged between 16 and 72
years (mean 37), four of the patients were female, 30subjects were inpatients in primary rehabilitation (timeafter injury between 1 and 18 months, mean 5), and two
were outpatients (4 and 6 years after injury). Levels of
Rating of spasticity was done directly before and after
the spinal cord injury were between C4 and T12 and
the hippotherapy session in the riding hall. The patient
between A and D according to the ŌĆśASIA Impairment
was lying on an examining table in supine position while
ScaleŌĆÖ10 (Table 1). Informed consent of all patients was
eight movement directions were rated: hip ’¼éexion and
obtained according to the Helsinki protocol.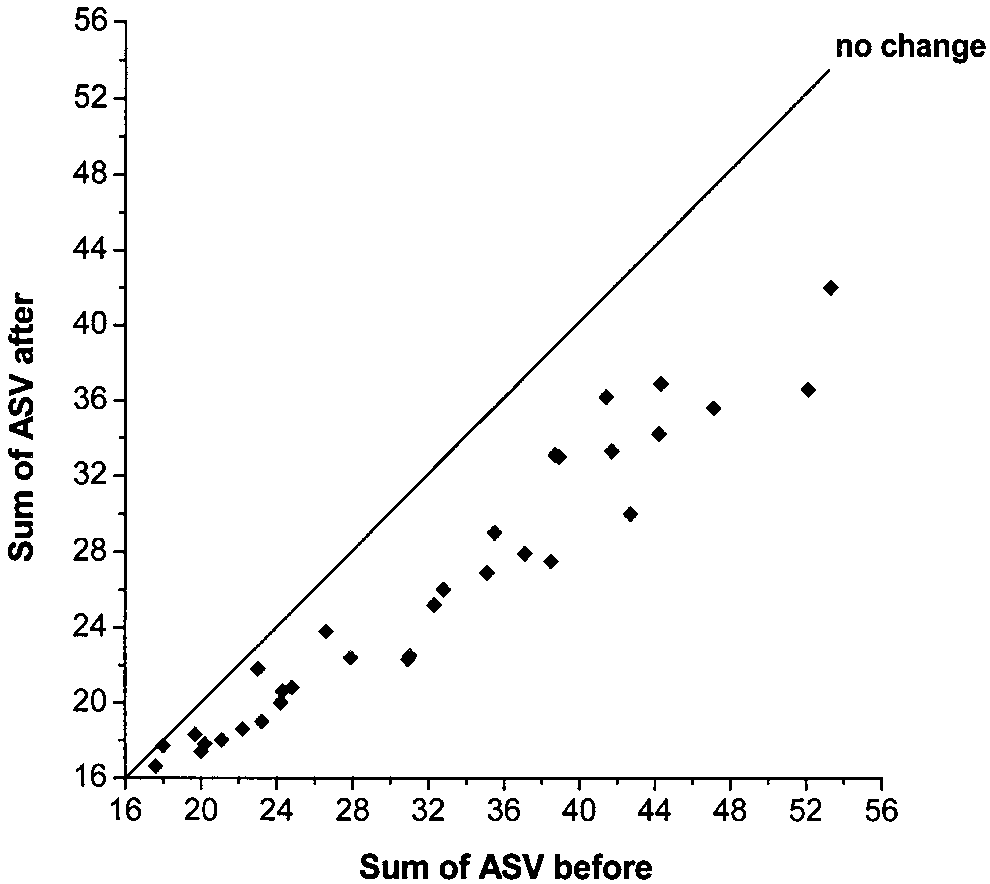
 Effect of hippotherapy on spasticity in SCI
extension, as well as ankle dorsi- and plantar’¼éexion. Thephysiotherapist moved the limb in the directions asquickly as possible. The knees and the ankles weremeasured with extended hips, while the lower legsdangling o’¼Ć the end ofthe testing bed. Each directionwas repeated three to ’¼üve times. She rated the elicitedspasticity according to the Ashworth Scale between 1and 5 (Ashworth-value, ASV) (Table 2). The ASV oftheeight movement directions ofboth sides were recordedas a sum of16 scores ranging from a minimum of16 to amaximum of80.
Effect of hippotherapy on spasticity in SCI
extension, as well as ankle dorsi- and plantar’¼éexion. Thephysiotherapist moved the limb in the directions asquickly as possible. The knees and the ankles weremeasured with extended hips, while the lower legsdangling o’¼Ć the end ofthe testing bed. Each directionwas repeated three to ’¼üve times. She rated the elicitedspasticity according to the Ashworth Scale between 1and 5 (Ashworth-value, ASV) (Table 2). The ASV oftheeight movement directions ofboth sides were recordedas a sum of16 scores ranging from a minimum of16 to amaximum of80. Effect of hippotherapy on spasticity in SCIHE Lechner et al
MS patients, a reduction in the muscle tone ofthe lower
valuable supplement to the conventional physiotherapy
extremities after hippotherapy was measured by electro-
approach in holistic rehabilitation ofSCIs.
Effect of hippotherapy on spasticity in SCIHE Lechner et al
MS patients, a reduction in the muscle tone ofthe lower
valuable supplement to the conventional physiotherapy
extremities after hippotherapy was measured by electro-
approach in holistic rehabilitation ofSCIs.