Head Injuries and Helmet Laws in Australia and New Zealand
Victoria was the first Australian State to introduce bicycle helmet laws, on 1 July 1990. Over the next few
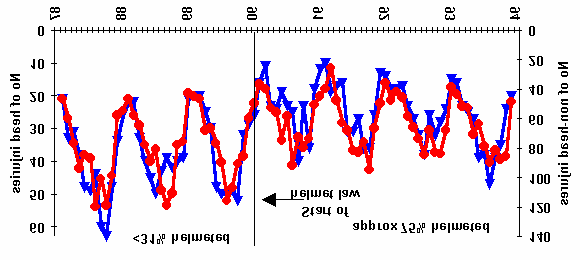
years, all other States passed similar legislation, because of threats by the Federal Government to reduce road funding if States failed to comply with a 10-point road safety program including bicycle helmet laws. New Zealand (NZ) also introduced a bicycle helmet law in January 1994.[1] [2] [3] [4] [5] Fig 1. Cyclists admitted to hospital in Victoria with/without head injuries 1) Did the laws work? (from Carr et al. 1995)[1]
The effect of the laws can be determined
by comparing injury rates before and after the laws were introduced.
a) Victoria. Fig1 shows numbers of
cyclists admitted to hospital with and without head injuries before and after the helmet law. Both head and non-head injuries fell substantially. As shown later (section 3), surveys revealed lots of people were put off cycling. Fewer cyclists should mean fewer injuries. But if helmets were effective, head injuries should have fallen by more
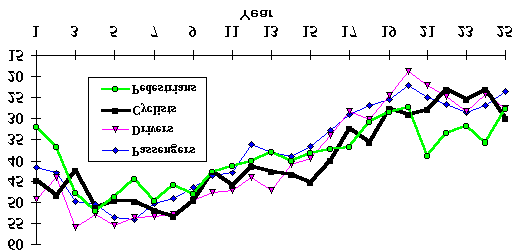
Fig 2. Percentages of NZ cyclists wearing helmets (%helmet)
than non-head injuries. Did they? Which line represents head injuries
& with head injury (%HI, from Robinson 2001)[2] Primary schoolchildren b) New Zealand. Fig 2 compares
head injury (%HI) rates of primary
helmet wearing (%HW) increased
from 43% to 92%. If compulsory wearing is beneficial, there should
%HI for accidents not involving motorvehicles
of adults compared to primary school children. Fig 2 shows there wasn't;
Fig 3. Percentage of hospital
What other explanation is there, except that
admissions with head injury, WA
helmets are less effective at preventing head
(from Hendrie et al. 1999)[3] c) Western Australia. Fig 3 shows
percentages of hospital admissions involving head injury for all road users. Helmet wearing at the start of the data series was virtually nil, increasing to about 39% of cyclists just before the law was enacted on 1 Jan 1992, when helmet wearing increased to over 80%. The most dominant feature in Fig 3 is the declining trend in %HI common to all road users. Re-searchers in Victoria found a similar trend, but mistakenly concluded
Fig 4. SA (from
helmets were remarkably effective. They didn’t bother to check that
Marshall &
the same trend was evident for pedestrians, so had nothing to do
White 1994)[4]
with helmets! If helmet laws are effective, it should be obvious from
Helmet law injuries (%)
the WA data when %HW increased from 39% to more than 80%. Can you tell which year it was? (Section 4 has more details.)
d) South Australia (SA, Fig 4) shows declining trends in hospital
admissions for concussion, but not other head/face injuries, and
again no obvious effect of a law that increased helmet wearing from
% Head injured 15 Other
40-90%. The decrease in concussions was noted and explained:
"it is understood that, since helmet wearing became compulsory, the head/face(%) Concussion (%) procedure for patients with a short episode of concussion has changed in that such patients are not now admitted routinely. [4] South Australia: year to end June Fig 5. NSW Head injury and helmet e) New South Wales (NSW, Fig 5) introduced a helmet law for children wearing %(HW) (adults in red, children
6 months after the law for adults. Numbers of cyclists admitted to hospital
<16 in black, from Robinson 1996) [5]
for head and other injuries were provided by NSW Health (see Robinson
1996).[5] As in other states, the dominant feature is a declining trend in
helmet law
%HI for both adults and children, with very little additional effect from the
substantial increases in helmet wearing due to the law.
Summary of head injury data
The data in Figs 1-5 show large increases in helmet wearing, but no
% Head injured adult %HI adult helmet law
major change in %HI, over and above the general trends. These trends
may relate to new diagnostic techniques (e.g. CAT scans), changes in
admission policies (as in SA), and safer roads (leading to lower impact
Year to end June
speeds in collisions, reducing the risk of head injury[6]).
Fig 6. All road fatalities in NSW by year Thus it seems impossible to conclude from %HI data that helmet laws have any large or significant benefit. 2) Successful road safety measures introduced
Not all road safety measures show almost undetectable
responses. Road fatalities fell immediately, and remained at 1100 a lower level, when random breath testing was introduced in 1000
NSW (Fig 6). Some measures – e.g. those encouraging responsible driving – seem remarkably effective.
In Victoria, campaigns against speeding and drink-driving were
introduced about the same time as the bicycle helmet law. A
Fig 7 Pedestrian fatalities, Victoria
medical journal reported that accident costs were reduced by an
estimated £100M for an outlay of £2.5M.[7] Fig 7 shows the fall in pedestrian fatalities. Other states also introduced road safety
campaigns about the same time as their helmet laws. Fig 8 shows all road casualties in SA in relation to the timing of the helmet law.
Figs 7 and 8 demonstrate why we must take care when claiming
benefits of helmet laws. Cyclists are likely to benefit just as much as pedestrians from campaigns to reduce speeding and drink-driving.
1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002
Some proponents of helmet laws have shown the equivalent of
Fig 8 All road casualties in South Australia
Fig 7 and 8 for cyclists, without explaining that similar benefits
(from Marshall & White 1994)[4]
were enjoyed by other road users. The Cochrane Review of Thompson et al. fails to mention the fall in non-head injuries in
Victoria (Fig 1), and dismisses the much safer road conditions (Fig 7), leading to the impression that the entire 40% fall in head cyclists’ head injuries was due to increased helmet wearing.[8]
Summary of injury data
Despite the lack of obvious change in %HI in response to
increased helmet wearing from legislation (Figs 1-5), proponents of helmet laws have claimed the laws were effective. They usually fail to mention important aspects of the data, such as the similar trends in %HI for all road users (Fig 3), that non-head injuries fell by almost as much as head injuries (Fig 1), or the large reductions in the amount of cycling (see next section).
Table 1. Number of cyclists counted (N) and wearing 3) Effect on numbers of cyclists, health and helmets (NH) in Melbourne, Victoria, pre-law (May 1990) the environment and in years 1 and 2 of the helmet laws (May 1991 and
Australian and NZ helmet laws are enforced. In
1992; from Finch et al. 1993)[9]
Victoria, about 20,000 cyclists are fined every year
1st law year 2nd law year
for not wearing a helmet. Some cyclists have even
gone to jail for non-payment of helmet-law fines.
Does the threat of a fine encourage cyclists to wear
helmets, or just discourage cyclists who don’t like
Table 1 shows the results of a large, compre-
hensive survey in Melbourne, using the same
*Counts in May 1992 were inflated by a bicycle rally passing through one
observation periods at 64 sites, in similar weather
site (451 cyclists counted at this site in 1992; 72 in 1991). Excluding the site with the rally, a total of 27% fewer cyclists were counted in 1992 than 1990.
Table 2. Counts of child cyclists in NSW before and in the first 2 years of the bicycle helmet law (from Walker, 1992; Smith & Milthorpe 1993).[10,11] 1991(Pre law) 1st law yr (1991) 2nd law yr (1992)
cycling rather than encourage helmet wearing. Compared with before the law, School gates
comprehensive survey of child cyclists at 122 sites covering Sydney, regional and rural areas of NSW. Before the law, 1910 children were observed wearing helmets. In the first and second years of the law 1019 and 569 more children were observed wearing helmets, but 2215 (36%) Fig 9. Numbers of cyclists (children and adults)
and 2658 (44%) fewer child cyclists were counted (Table 2).
counted at 25 sites in Sydney (Walker, 1996)[8]
This was not a transient decline. There is no evidence that
cycling “recovered”. Fig 9 shows a series of counts over 6
years at 25 sites in Sydney. Both adult and child cyclists were
counted.[12] There were four surveys in April and two in
October. More cyclists were observed in April than October,
perhaps because autumn weather may be more conducive to
cycling. However, by 1996, there were 48% fewer cyclists than
1991. This is in complete contrast to the situation before the
No. of cyclists counted
law, when, in the Sydney metropolitan area "cycling increased significantly (+250%) in the 1980s".[13]
Before helmet laws, cycling was increasing. Australian census data show cycling to work increased by
47%, from 1.11% (1976) to 1.63% (1986). There is no reason to believe this trend wouldn’t have continued without the laws. Indeed, the average proportion cycling to work in states without enforced helmet laws increased in 1991, contrasting with the average decline for other states. By 1996 when all states had enforced laws, only 1.19% of journeys to work were by bike, with a similar proportion in 2001. People often cited helmet laws as a reason for not cycling. The equivalent of 64% of adult cyclists in Western Australia said they'd ride more except for the helmet law. In New South Wales, 51% of schoolchildren owning bikes, who hadn't cycled in the past week, cited helmet restrictions, substantially more than other reasons, including safety (18%) and parents (20%).
Proponents of helmet laws have argued that the above data are outdated and distorted by a reduction in
the legal driving age. This is untrue. In Victoria, teenagers who pass the driving test may drive unsupervised from age 18. This has not changed, though the minimum age for a learner permit was lowered from 17 to 16 in Victoria. Learners must be supervised at all times by a licensed driver, so it seems unlikely this caused any significant part of the 42% fall in children’s cycling, or the 29% fall in adult cycling in Melbourne. Moreo-ver, there was no change in NSW, yet, by the 2nd year of the helmet law, child cycle use had fallen by 44%.
Lack of exercise is a major health problem in most western societies. The New Scientist recently reported
that poor diet and physical inactivity may soon overtake tobacco as the leading cause of death http://www.newscientist.com/news/news.jsp?id=ns99994763
Other studies show the health benefits of cycling greatly exceed losses from accidents. UK researcher
Mayer Hillman estimated that 20 life years were gained from the health benefits of cycling (even without a helmet), for every year lost through accidents.[14] If bicycle helmet laws discourage cycling, as in Australia, our health will be worse, not better. If cycling for transport is discouraged, cars may be used instead, increasing vehicle pollution and greenhouse gas emissions. 3) Safety in Numbers
An interesting paradox is that countries with helmet laws (and therefore high helmet wearing rates) tend to
have higher injury rates per kilometre cycled than countries with low helmet-wearing rates. This again suggests that helmet laws are counter-productive. Helmet law promoters often try to dismiss these facts, but it is better to examine and understand the evidence, than ignore it.
A really important paper, published last year in the prestigious international journal, Injury Prevention, has
a very plausible explanation.[15] It reported that the risk per cyclist (and pedestrian) is lower when there are more cyclists (pedestrians). For 6 different datasets, a consistent relationship was found, comparing a) data from different countries, b) different cities and towns in the same country, and c) comparing injury rates and
Fig 10. Fatalities (1983-88) per 100 million
amounts of cycling in the same country over time.[15] This
km vs mean daily distance cycled
relationship, called the Growth Rule, shows that when
cycling doubles, injury rates per cyclist falls by an average
of 34%. Conversely, according to the Growth Rule, if
cycling halves the risk per cyclist will increase by 52%.[15]
‘Safety in Numbers’ is also true for Australia. The last
comprehensive dataset on cycle use was for 1985, but it shows a very strong relationship between distance cycled
Fatalities/100,000,000 km
in different Australian states and fatality rates per km
cycled (Fig 10). States with the most cycling (Australian
Mean distance cycled/person/day (km)
Capital Territory, Queensland and Western Australia) had
The Northern Territory (NT) was included in Fig 10 for
the lowest fatality rate per km cycled; those with the least
completeness, but, with population of about 160,000, is
cycling the highest fatality rate per km.[16]
too variable to be meaningful. The NT had 11 cyclist deaths from 1983-88, but other 6-year periods (e.g.
So what happened with the helmet laws? Did cyclists
1980-82 & 1989-91) had less than half that number
have higher injury rates, due to the fall in cycling with the law? As noted earlier, we must allow for the fact that helmet laws were introduced at the same time as road safety campaigns that reduced deaths and serious injuries to other road users (Figs 7 and 8). Safer roads should lead to fewer collisions with motor vehicles. Moreover, when collisions occur, impact speeds should be lower, reducing the risk of both death and serious head injury. In experiments designed to mimic pedestrians and cyclists hit by vehicles, lowering impact speed from 40 to 30 km/hr reduced maximum head acceleration by 39% (and head injury criterion by 66%), compared to 20-25% reductions in maximum acceleration of chest, pelvis and feet.[6]
We can allow for the safer roads by noting that pedestrian and cyclist injuries follow very similar trends.[5]
So, by comparing pedestrian and cyclist safety before and after the law, we can evaluate whether cyclist head injuries declined (compared to pedestrians) with increased helmet wearing, or whether the fall in cycling increased injury rates, because of reduced ‘Safety in Numbers’.
Table 3 shows that, in the two years before the law, deaths and serious head injuries (DSHI) represented
26.5% of all serious injuries (ASI) to cyclists in bike/motor vehicle collisions in Victoria. This fell by 1.7 per- centage points to 24.8% in the 2 years after the law. For pedestrians, the fall over the same period was actu- ally greater – 2.5 percentage points. Helmets are popularly believed to prevent death and serious head injury, yet the fall in %DSHI for Table 3. TAC (Transport Accident Commission) data for average numbers of deaths pedestrians was actually greater and serious head injuries (DSHI) and all serious injuries (ASI) per year in Victoria than that achieved for cyclists
in Numbers’ operated in reverse. 2 post-law yrs as % of 2 pre-law years 56.6
1DSHI as defined by TAC (skull fracture or brain injury excluding concussion).
pre-law numbers (Table 3), thanks to the road safety campaign already mentioned. Cyclist DSHI fell to 57% of pre-law numbers, but there were fewer cyclists – only 69% as many as before the law (Table 1). DSHI should therefore have fallen to (69% x 74%) = 52% of pre-law numbers for cyclists to enjoy the same injury reductions as pedestrians. The actual fall suggests that cyclists did not fare as well with the helmet law as they ought to have done without it. Increased injury rates following helmet laws was also noted for child cyclists in NSW.[5] This strongly suggests that helmet laws are counter-productive and may increase the risk of death and serious injury. As well as reduced ‘Safety in Numbers’, another possible factor is risk compensation; cyclists may take more risks, or motorists take less care when they encounter cyclists, because of the apparent protection of helmets. 4) Cost-benefit analyses
Any realistic estimate of the cost of helmet laws should include health and environmental costs of reduced
cycling, as well as any increases in injury rates from risk compensation or reduced ‘Safety in Numbers’. This has never been done; research into helmet laws has generally been funded by government agencies.
Nonetheless, the published cost-benefit analyses provide some very interesting information – that the risk
of head injury per cyclist is relatively small. For this reason alone, helmet laws cost the community money. For example, in New Zealand, adult cyclists spent NZ$5.9 million on helmets, but the most optimistic estimate was that the law saved NZ$0.17 million in treating head injuries (See Table 1 of http://www.cyclehelmets.org/papers/c2019.pdf)[17] Even this is debatable. Head injury data for NZ are shown in Fig 2. Helmet wearing of adults rose dramatically with the law, but not primary schoolchildren. Yet percent head injury (%HI) of both groups follow similar trends. In fact, %HI for primary schoolchildren actually
declined slightly more than adults. Thus, despite its $5.9 million price tag, the helmet law for adults may not have prevented any head injuries whatsoever.
Another cost-benefit analysis was carried out for Western Australia (WA) by Delia Hendrie, University of
WA. She estimated that the WA helmet law cost $21.6 million, including $20.2 million to purchase helmets.[3] As discussed earlier, %HI of cyclists followed similar trends to that of other road users (Fig 3). However, the graph has a very curious feature – a large increase in %HI of pedestrians (but not other road users) in year 21, a year before the helmet law. This seems to have been transient. By year 25, pedestrian %HI had fallen below that of cyclists. However, if, without the law, cyclists %HI were presumed to follow exactly the same trend as pedestrians (a highly contentious assumption!) the average difference over this period, about 20 to 44 head injuries per year, mostly of moderate severity, might (albeit unrealistically) be deemed an effect of the law. Depending on the model fitted and how costs of head injuries are calculated, net benefits, estimated in this unrealistic way, range from -$15.1 million (i.e. the law still cost $15.1 million more than an unrealistically optimistic estimate of what it saved) to $2 million. Thus, as in New Zealand, and especially if estimates of lost benefits from reduced cycling are included in the costs of the law, the WA helmet law cost far more than any realistic estimate of its benefit. 5) What causes Brain Injury?
Experimental evidence shows that brain damage is caused mainly by rotation. Rotational forces can
shear the brain’s neuronal connections, a condition known as diffuse axonal injury (DAI). In one experiment 12 squirrel monkeys were subjected to linear accelerations with peak levels 665-1230 g, and 13 primarily to rotational accelerations in the range of 348 to 1025 g.[18] Contact phenomena were minimised by the design of the apparatus. None of the monkeys receiving linear acceleration was concussed, but all 13 receiving rotational acceleration suffered concussion, and the group had a high incidence of brain injuries such as subdural haematoma, subarachnoid haemorrhage and intracerebral petechial haemorrhage.
There is little reliable evidence whether bicycle helmets reduce, or increase, the risk of rotational injury.
No-shell helmets may stick on pavement and increase the risk of rotating the head. The Australian NHMRC (National Health and Medical Research Council) discussed football helmets (which may have some similarity with bike helmets), stating: "The use of helmets increases the size and mass of the head. This may result in an increase in brain injury by a number of mechanisms. Blows that would have been glancing become more solid and thus transmit increased rotational force to the brain. These forces result in shearing stresses on neurones which may result in concussion and other forms of brain injury."[19]
Does this happen in real life? In a paper, "Cycling: your health, the public’s health and the planet’s
health", Public Health Physician, Dr Ashley Bloomfield wrote: "The earliest murmurings that I heard against helmets were from a neurosurgeon who I worked for in 1994. He claimed that cycle helmets were turning what would have been focal head injuries, perhaps with an associated skull fracture, into much more debilitating global head injuries. We had a couple of examples on the ward at the time, and it was a bit worrying. However, I wasn’t too convinced as I figured that the injuries that would previously have been focal head injuries may well have been resulting in death, so the neurosurgeon was never actually seeing them. Instead, they were making their way straight to the pathologist."[20] (seehttp://www.cycle-helmets.com/bloomfield.pdf)
However, the comparison of pre- and post-helmet law statistics for pedestrians and cyclists in Victoria
(Table 3), suggests that helmets prevent few, if any deaths or serious head injuries (DSHI). In fact, DSHI to cyclists, as a proportion of all serious or fatal injuries to cyclists (%DSHI), fell by (marginally) less than the same statistic for pedestrians. More importantly, the risk of death or serious head injury per cyclist actually increased compared to what would have been predicted without the law.
Thus, there is some worrying evidence that helmets might increase the risk of rotational injuries. This may
explain the increase in DSHI, compared to what would have been expected without the law. Other factors such as risk compensation and reduced ‘Safety in Numbers’ may also be important. Available data are insufficient to draw any firm conclusions. One problem is that diffuse axonal injury (DAI) is very hard to see on CAT scans, so many cases may be missed.
In motorcyclists, the serious brain damage from rotational injuries (despite, presumably, wearing traditional
helmets) was noted by physician Dr Ken Phillips. He was so concerned he decided to try and improve matters. Dr Phillips observed that the scalp provides the brain with protection against rotational forces because it is elastic, compressible and moves around the skull without friction. To mimic this process, the 'Phillips helmet' has an outer shell of polyethylene that moves independently of the inner cushion - see http://www.phillipshelmets.co.uk/PHL%20frame.htm. Unfortunately, no helmet manufacturer was interested, so Dr Phillips started his own company to make and market them.
6) The final paradox
The evidence reported here indicates that helmet laws are not effective and may even increase the risk of
injury per cyclist. The many reasons for this include: risk compensation, reduced safety in numbers, failure to
wear helmets correctly and the fact that helmets probably offer little protection against the most debilitating type of brain injury – rotational injuries.
So why is so much effort expended promoting helmet laws? One source of confusion is that case-control
studies comparing cyclists choosing to wear helmets with helmetless cyclists usually show that helmet wearers have a lower %HI. But why? Is this because helmets offer some benefit, or that cyclists choosing to wear helmets are more cautious, have different riding styles and get into less serious accidents? Studies show that cyclists who chose to wear helmets are more likely to obey traffic signs, wear high visibility clothing, have higher socioeconomic status, use lights at night, ride in parks, playgrounds, or on bicycle paths, rather than city streets, (in the US) be white rather than other races, and (for children) tend to ride with other children or adults, rather than alone.[5] One US study also found that helmet wearers had much less serious non-head injuries, as well as head injuries.
Although case-control studies try to control for these differences (known as confounding factors), it is
virtually impossible to record and control for all differences between wearers and non-wearers. This problem was discussed in a series of papers in the International Journal of Epidemiology (IJE) in June 2004, after a similar paradox was noted for hormone replacement therapy (HRT).[21]
In 1991, a review of the best quality observational studies concluded that HRT reduced the risk of coro-
nary heart disease by 50%, and that ‘overall, the bulk of the evidence strongly supports a protective effect of estrogens that is unlikely to be explained by confounding factors’.[22] Yet when randomized control trials were carried out, the exact opposite was found – that HRT increased the risk of coronary heart disease by 29%. Just as cyclists who choose to wear helmets tend to be more cautious and have higher socioeconomic status, women choosing HRT also tend to have higher socioeconomic status. Results from the observational studies had, in fact, suggested the possibility of bias from confounding; HRT was apparently equally protective against accidental and violent deaths as it was against cardiovascular disease deaths in one observational study.[22]
Can similar checks for bias be applied to case-control studies of helmet efficacy? In the most widely citied
study, most (86%) of the community controls were children under 15.[23] 21.1% wore helmets when they fell of their bikes, compared to 5.9% of 202 children given emergency room treatment in Seattle for non-head injuries. The odds ratio for helmets preventing head injury (HI) was calculated by comparing the 143 HI children (‘cases’) with the community controls.[23] In exactly the same way, children treated for injuries to other parts of the body can be considered ‘cases’. This produces an odds ratio of 0.23, indicating that helmets prevent 77% of injuries to other parts of the body! This suggests, as was found for the HRT observational studies, that much of the estimated benefits could be artifacts of confounding.
Another indicator of potential confounding was that surveys at the same time as the widely-cited Seattle
study found that 3.2% of 4501 child cyclists riding round Seattle wore helmets.[24] This is not significantly different from the 2.1% and 5.9% helmet wearing (%HW) of children with head and non-head injuries. However, all three are completely different from the 21.1% HW of the community controls (p < 0.001). We might therefore conclude that helmet wearers are nearly 7 times more likely to fall off their bikes than non-wearers, suggesting that risk compensation is far more important than any possible benefits of helmets. However, this may also be an artifact of confounding. Community controls were members of a Group Healthcare Cooperative that may have promoted helmet wearing to members. Children might also be persuaded to wear helmets when they are more likely to fall off their bikes, e.g. when learning to ride. Thus we may conclude it is very difficult to fully adjust for confounders in observational studies of helmet efficacy.
The best estimates of the benefits of helmets laws are those based on what actually happens when such laws are introduced. As shown in Figs 2-5, even though other road safety measures achieved large reductions in injury rates (Figs 6-8), there were no major changes in cyclists %HI when helmet laws were introduced. In contrast, the large fall in non-head injuries (Fig 1) suggests the laws discouraged cycling. 7) Conclusions
Comparisons of pre- and post-law injury data (Figs 1-5) show that there is little benefit to either cyclists or
the community from passing laws forcing cyclists to wear helmets. Rather than encouraging cyclists to wear helmets, the laws appear to have discouraged cycling, resulting in reduced health and fitness, but very little change in %HI. If the money spent on helmets had been used for other measures e.g. improving accident blackspots for cyclists, the benefits would have much been greater.
More importantly, risks per cyclist seem to have increased, compared to what would have been expected
without the law, implying that helmet laws are counter-productive. Possible explanations include risk compensation, reduced ‘Safety in Numbers’ and that brain damage is predominantly due to rotational injury.
Helmets undoubtedly help prevent minor wounds to the head, but are not designed to cope with the forces
that may occur in bike/motor vehicle collisions. There is little reliable experimental evidence whether bicycle
helmets reduce, or increase, the risk of rotational brain injury. However, as a precaution, cyclists choosing to wear helmets may wish to consider new designs such as the ‘Phillips’ helmet.
In contrast to the little or no obvious change in %HI with bicycle helmet laws, injury statistics following
measures to reduce speeding and drink driving (Figs 6-8) show considerable benefit. The vast majority of fatal and very serious head injuries to cyclists result from bike/motor vehicle collisions. The most effective way to reduce injuries to cyclists and all other road users is therefore to reduce the risk of bike/motor vehicle collisions.
As well as enforcing appropriate speed limits, controlling drink-driving and encouraging cyclists to use
lights at night and ride on the correct side of the road, cycling becomes safer when more people cycle. The best option to improve overall safety, improve our health and fitness and benefit the environment is therefore a package of measures to encourage cycling and make the roads safer, while allowing cyclists to chose whether of not they wish to wear helmets.
Dr Dorothy L Robinson, Snr Statistician, Cycle-Safe, Armidale, NSW 2351. Email: drobinso@mendel.une.edu.au
References and sources of data
The data shown have been compiled over many years from many sources. Data on injuries to cyclists and
pedestrians in Victoria (Table 3) were kindly provided by the Victorian Transport Accident Commission. The appendix provides more details on how head injuries are classified. Fatality data (Figs 6 and 7) were obtained from the ATSB website (www.atsb.gov.au). Other data were obtained from the following published papers and reports.
1. Carr D, Skalova M, Cameron M. Evaluation of the bicycle helmet law in Victoria during its first four years: Rpt 76
Monash Univ Acc Res Centre Melbourne, 1995.
2. Robinson DL. Changes in head injury with the New Zealand bicycle helmet law. Accid Anal Prev 2001;33(5):687-91. 3. Hendrie D, Legge M, Rosman D, Kirov C. An economic evaluation of the mandatory bicycle helmet legislation in
Western Australia: http://www.officeofroadsafety.wa.gov.au/Facts/papers/bicycle_helmet_legislation.html (accessed October 2004), 1999.
4. Marshall J, White M. Evaluation of the compulsory helmet wearing legislation for bicyclists in South Australia Report
8/94: South Australian Department of Transport Walkerville South Australia, 1994.
5. Robinson DL. Head injuries and bicycle helmet laws. Accid Anal Prev 1996;28:463-475. 6. Janssen EG, Wismans JSHM. Experimental and mathematical simulation of pedestrian-vehicle and cyclist-vehicle
accidents. Proceedings of the 10th International Technical Conference on Experimental Safety Vehicles. Oxford, July 1985.
7. Powles JW, Gifford S. Health of nations: lessons from Victoria, Australia. BMJ 1993;306:125-7. 8. Thompson D, Rivara F, Thompson R. Helmets for preventing head and facial injuries in bicyclists (Cochrane Review):
In: The Cochrane Library, Issue 3, 2003. Oxford: Update Software., 2003.
9. Finch C, Heiman L, Neiger D. Bicycle use and helmet wearing rates in Melbourne, 1987 to 1992: the influence of the
helmet wearing law. Melbourne: Rpt 45, Monash Univ Acc Res Centre, 1993.
10. Walker M. Law compliance among cyclists in New South Wales, April 1992. A third survey.: Road and Traffic
Authority Network Efficiency Strategy Branch, July 1992.
11. Smith N, Milthorpe F. An observational survey of law compliance and helmet wearing by bicyclists in New South
Wales - 1993.: Roads and Traffic Authority, 1993.
12. Walker M. Bicycling in Sydney: law compliance and attitudes to road safety. Velo Australis; 1996; Fremantle,
13. Webber R. Cycling in Europe. In: Shepherd R, editor. Ausbike 92. Proceedings of a national bicycle conferences, Melbourne, Australia. Melbourne: Bicycle Federation of Australia, March, 1992.
14. Hillman M. Cycle helmets the case for and against: Policy Studies Institute London 1993, 1993. 15. Jacobsen PL. Safety in numbers: more walkers and bicyclists, safer walking and bicycling. Inj Prev 2003;9(3):205-9. 16. Robinson DL. Safety in Numbers in Australia: more walkers and bicyclists, safer walking and bicycling. Health Promotion Journal of Australia 2005;(In press).
17. Taylor M, Scuffham P. New Zealand bicycle helmet law-do the costs outweigh the benefits? Injury Prevention
18. Gennarelli TA, Thibault LE, Ommaya AK. Pathophysiological Responses to Rotational and Translational
Accelerations of the Head, SAE Paper No. 720970. 16th Stapp Car Crash Conf.; 1972. Society of Automotive Engineers, 1972.
19. National Health and Medical Research Council. Football injuries of the head and neck: Australian Government
Publishing Service, GPO Box 84, Canberra, ACT 2601, Australia., 1994.
20. Bloomfield A. Cycling: your health, the public’s health and the planet’s health. Making Cycling Viable New Zealand
Cycling Symposium; 2000; Palmerston North 14-15 July 2000.
21. Petitti D. Commentary: hormone replacement therapy and coronary heart disease: four lessons. Int J Epidemiol
22. Lawlor DA, Davey Smith G, Ebrahim S. Commentary: The hormone replacement-coronary heart disease
conundrum: is this the death of observational epidemiology? Int. J. Epidemiol. 2004;33(3):464-467.
23. Thompson RS, Rivara FP, Thompson DC. A case-control study of the effectiveness of bicycle safety helmets. N
24. DiGuisseppi CG, Rivara FP, Koepsell TD. Bicycle helmet use by children. Evaluation of a community-wide helmet
25. Cameron M, Newstead S, Vulcan P, Finch C. Effects of the compulsory bicycle helmet wearing law in Victoria during
its first three years. Proc. Austral. Pedest & Bicyclist Safety & Travel Workshop; 1994.
26. Cameron M, Vulcan A, Finch C, Newstead S. Mandatory bicycle helmet use following a decade of helmet promotion
in Victoria, Australia - An evaluation. Acc Anal Prev 1994;26:325-37.
27. Povey LJ, Frith WJ, Graham PG. Cycle helmet effectiveness in New Zealand. Accid Anal Prev 1999;31(6):763-70.
Appendix: other published analyses and description of head injuries A1. Other published analyses of head injury data
The data in Figs 1-5 show that, in contrast to the large benefits from campaigns against speeding and drink-driving
(Fig 6-8), there was no obvious change in %HI from bicycle helmet laws. Indeed, the large reduction in non-head injuries (Fig 1) suggests the main effect of the laws was to discourage cycling, rather than protect against head injury. Despite this, proponents of helmet laws claim they are effective; they advise cyclists that wearing a helmet may save their lives. This divergence of opinion is discussed by reviewing research frequently cited by advocates of such laws.
One widely-cited report is: Carr et al. (Monash Univ Accident Research Centre (MUARC), 1995)[1]. It notes (as is
obvious in Fig 1) that numbers of head injuries fell by 40% after the helmet law in Victoria. The authors explained they could not tell from their analysis whether this was because fewer people cycled after the law, or because helmet wearing increased. So why analyze numbers of head injuries? MUARC’s analysis of the first 3 years of helmet law data found that %HI was no different to that predicted from pre-law trends.[25] Might we speculate the main reason for focussing on numbers (rather than percentages) of head injuries was a desire to justify the helmet law?
Another widely-cited publication was MUARC’s analysis of the first 2 years of helmet-law data: "(TAC) insurance claims from bicyclists killed or admitted to hospital after sustaining a head injury decreased by 48% and 70% in the first and second years after the law, respectively. Analysis of the injury data also showed a 23% and 28% reduction in the number of bicyclists killed or admitted to hospital who did not sustain head injuries in the first and second post-law years, respectively."[26]
Fig 1 shows all cyclist hospital admissions, irrespective of whether the cyclist fell off the bike, or was hit by a fast
moving motor vehicle. Although risk compensation might also be important, we may hypothesize that the dominant influence on numbers of non-motor-vehicle injuries is the amount of cycling. The observational surveys (Table 1), and the fall in numbers of non-head injuries (Fig 1), strongly suggest the main effect of the law was to discourage cycling. Thus the most likely cause of the 40% reduction in head injuries was that the law discouraged cycling.
In contrast, insurance claims for injuries in motor vehicle accidents also depend on other factors, including driver
behaviour and vehicle travelling speeds. This was demonstrated by the 42% in pedestrian deaths from1989 to 1990 (Fig 7). Table 3 compares deaths and serious head injuries (as a percentage of all serious injuries, %DSHI) of pedestrians and cyclists in motor-vehicle accidents. The fall %DSHI of pedestrians was actually greater than for cyclists. Indeed, the risk of DSHI per cyclist appears to have increased relative to that for pedestrians.
MUARC didn’t use pedestrians as a control and didn’t explain that numbers of pedestrians with concussion fell by
29% and 75% in the first and second years of the helmet law. This reduction for pedestrians is almost as impressive as the 48% and 70% falls in head injuries of cyclists over the same period, compared to 23% and 28% falls in other injuries. It implies that helmets were not the main cause. One refereed paper set the record straight by comparing all head injuries, including concussion, of pedestrians and cyclists, showing both followed almost identical trends.[5]
Section 3 uses the alternative approach of considering only deaths and injuries serious enough to warrant admission
to hospital. Table 3 was based on TAC’s classification of serious head injury, i.e. skull fracture (ICD-9 codes 800, 801, 803, 804) and brain injuries (codes 851-854), but not or wounds to the head or concussion with no other sign of brain injury. This contrasts with MUARC’s definition of "bicyclists killed or admitted to hospital after sustaining a head injury", which included concussion and wounds to the head or ears, even if the main reason for admission was a serious injury to another part of the body.[26]
Table 3 shows the risk of death and serious head injury (as defined by TAC) increased relative to that for
pedestrians. We may therefore conclude that the widely-quoted claims of 48% and 70% reduction in cyclist head injuries were mainly due either to changes in admission procedures and improved road safety conditions (resulting in 29% and 75% reductions in numbers of concussions to pedestrians). Cyclists admitted to hospital for treatment of serious injuries to other parts of the body may also have had fewer head wounds. Most people wear helmets because they hope to be protected against death and serious head injury. Despite the claims of helmet law proponents, TAC data suggest that the helmet laws in Victoria actually increased the risk of DSHI relative to the amount of cycling.
A2. Other published analyses of the amount of cycling
The abstract of MUARC publication claiming 48% and 70% reductions in head injuries also stated: “Surveys in Melbourne also indicated a 36% reduction in bicycle use by children during the first year of the law and an estimated increase in adult use of 44%”
Yet the survey data (Table 1) show 29% fewer adults were counted in May 1991 than May 1990. So why did
MUARC claim that adult cycling increased by an estimated 44%? MUARC estimated cycle use from the time cyclists took to ride through marked areas. However, in 1990, adult cyclists were counted, but not timed. This should not preclude adult cycle use from being estimated, because numbers counted and estimates of cycle use are strongly
correlated. For example, the first post-law survey found a decline in cycle use by teenagers of 44%, little different from the 48% drop in numbers counted. This implies that the 29% decline in number of adults counted is a valid and reasonable estimate of the change in adult cycle use.
But instead of reporting this direct estimate, MUARC ignored the number of adults counted in 1990, and estimated
the effect of the law by comparing adult cycle use in 1991 with a much earlier survey (1987/99) at a different time of year. This is a totally invalid because (as can be seen in Figure 1) cycle use has a marked seasonal variation. If the same “trick” of ignoring data from1990 had been carried out for teenagers, MUARC could have claimed the law reduced teenage cycle use by a mere 8%, instead of the 44% actually observed!
The decisions taken by MUARC to base their final analysis on numbers of head injuries, rather than percentages,
and ignore numbers of adult cyclists counted in 1990, created considerable confusion about the effects of helmet laws. Governments may have wished the laws to be considered successful. However, readers of the original reports would understand the data were open to other interpretations. Unfortunately, summary reports by proponents of helmet laws in other countries often omitted all-important details, leading to the false impression that the laws were remarkably successful. Figs 1-5, showing the original data, demonstrate that this was not the case. Readers should inspect the graphs, in conjunction with details about how the data were compiled (below), and make up their own minds.
Mistakes in relation to HRT were discussed in the International Journal of Epidemiology. Four important lessons had
to be learned: 1) do not turn a blind eye to contradiction, 2) do not be seduced by mechanism, 3) suspend belief and 4) maintain skepticism.[21] Bicycle helmet researchers, who use same methods, need to learn the same lessons. Helmet law promoters believe helmets work; the mechanism (they absorb energy) is seductive. Cyclists who doubt the benefits may be less likely to wear helmets. So promoters ignore contradictory evidence about risk compensation, causes of brain injury and that increased wearing from 30-40% to 75-90% following helmet laws produced no large or obvious response in %HI.
Helmet laws promoters also cite data showing generally declining trends in %HI coinciding with increasing trends in
helmet wearing. But Fig 3 shows declining trends commonly affect all road users. It is therefore impossible to separate effects of long-term trends from gradual changes in helmet wearing as a result of education, or non-enforced laws.
The Australian and New Zealand data are unique in that they produced very large, rapid, increases in helmet wearing
– 40 or 50 percentage points. Yet there was no obvious response in %HI, but large reductions in the amount of cycling, (Figs 1-5, Tables 1-3). This provides strong, compelling evidence that helmet laws do not work, refuting the claims of those who wish to compel all cyclists to wear helmets.
A3. Classification of head injury data (Figs 1-5, Table 3)
As shown in the acknowledgments, Figs 1-5 were complied from other publications, using other people’s
classification of head injury. The example for Victoria (Appendix A1) showed that different classifications may reveal different effects. No effect of the helmet law was detectable in comparison with pedestrians, but larger trends in %HI were evident when concussion (with no other sign of brain injury) was included. The definitions of head injury for Figs 1-5 and Table 3 are therefore listed below to enhance understanding of the data.
Source and Description (ICD9 codes) for head injures (HI) and other injuries (OI)
Fig 1. Victoria (Vic)
HI = any hospital admission with skull or facial fracture (800-803.9), concussion or intracranial
injury (850-854.1), open wound of ear (872-872.9) or open wound to head (873.0, 873.1, 837.8, 873.9). OI = other admission
Fig 2. New Zealand
HI = admissions with skull or facial fracture (800–804.99), intracranial injury or concussion (850–
855.99); OI = admission with limb fracture (810–829.99); excludes admissions for collisions involving motor vehiclesFig 3. Western Australia
HI = hospital admission with skull or facial fracture (800-804), concussion or intracranial injury
(850-854), 873.0-873.1 (open wound to head), 900 (injury to blood vessels of head or neck) and 950-951 (injury to optic or other cranial nerves); OI = all other admissions.
Fig 4. South Australia (SA)
HI = hospital admission with principal diagnosis of skull fracture (800-802; 802.4-804.06),
intracranial injury (851-854.16), 870-871.9, 873-873.39, 873.42-873.52), with concussion (850) tabulated separately. OI = other admissions.
Fig 5. New South Wales
HI = hospital admissions with head injury (NSW Health classification); OI = admission with other
injury. Cyclists with both head and other injuries were included in both categories.
Table 3. Victoria; Death or
DSHI = no-fault insurance claim for cyclists or pedestrians in collisions with motor vehicles for
death or serious head injury (skull fracture (800,801,803,804) or intracranial injury (851-854)).
OSI = other claim for serious injury likely to result in hospital admission.
Most classifications included all head injuries: skull and facial fractures, intracranial injuries, concussion and wounds
to the head. As discussed in Section 5, the most debilitating brain injuries may be caused by rotations, for which helmets might not offer any protection. However, helmets undoubtedly prevent wounds to the head, so some effect of increased helmet wearing could be expected when head wounds are included – Figs 1 (Vic), 3 (WA) and presumably 5 (NSW), but not Fig 2 (NZ). Fig 4 (SA) used principle diagnosis, so a decrease in minor wounds to the head of cyclists admitted to hospital for other reasons may not be apparent.
For WA, Fig 3 shows data from 1971-95, classified by Hendrie et al.,[3] for cyclists, pedestrians and motor vehicle
occupants. An alternative classification, only for cyclists, from 1981-95, based on principle diagnosis, was also published – see http://www.health.wa.gov.au/publications/pubhealth/app15.htm. Data for skull fractures and intracranial injuries were very highly correlated (r=0.98) with the cyclist data in Fig 3. A much better insight into the full picture is provided by Fig 3, because it also shows the same statistics for other road users.
Suzanne Somers, one of America's most beloved personalities, has a diverse career that has taken her from actress and stage entertainer, tosuccessful entrepreneur and writer to yet another role as an ardent advocate for healthy living. In her latest bestseller, Breakthrough: Eight steps toWellness, Suzanne interviewed healthcare professionals about developments in wellness and longevity. She br
Donnerstag, 8. November, 09:00 Uhr Gottesdienst mit Eucharistiemit Pfr. Franz SaboHl. Messe für Georg Schnell-Litzler, Josef Schnell-Mauri, Mario Karrer-Heizmann, Marie und Werner Giger-Allemann, Wilhelm und Lina Dietler mit Rita, Willy und LinaAnschliessend Donnschtigskaffi Sonntag, 11. November, 10:00 Uhr Gottesdienst mit Eucharistiemit Pfr. Franz SaboEs singt der Chor „Les Souvenirs“
 Head Injuries and Helmet Laws in Australia and New Zealand
Head Injuries and Helmet Laws in Australia and New Zealand 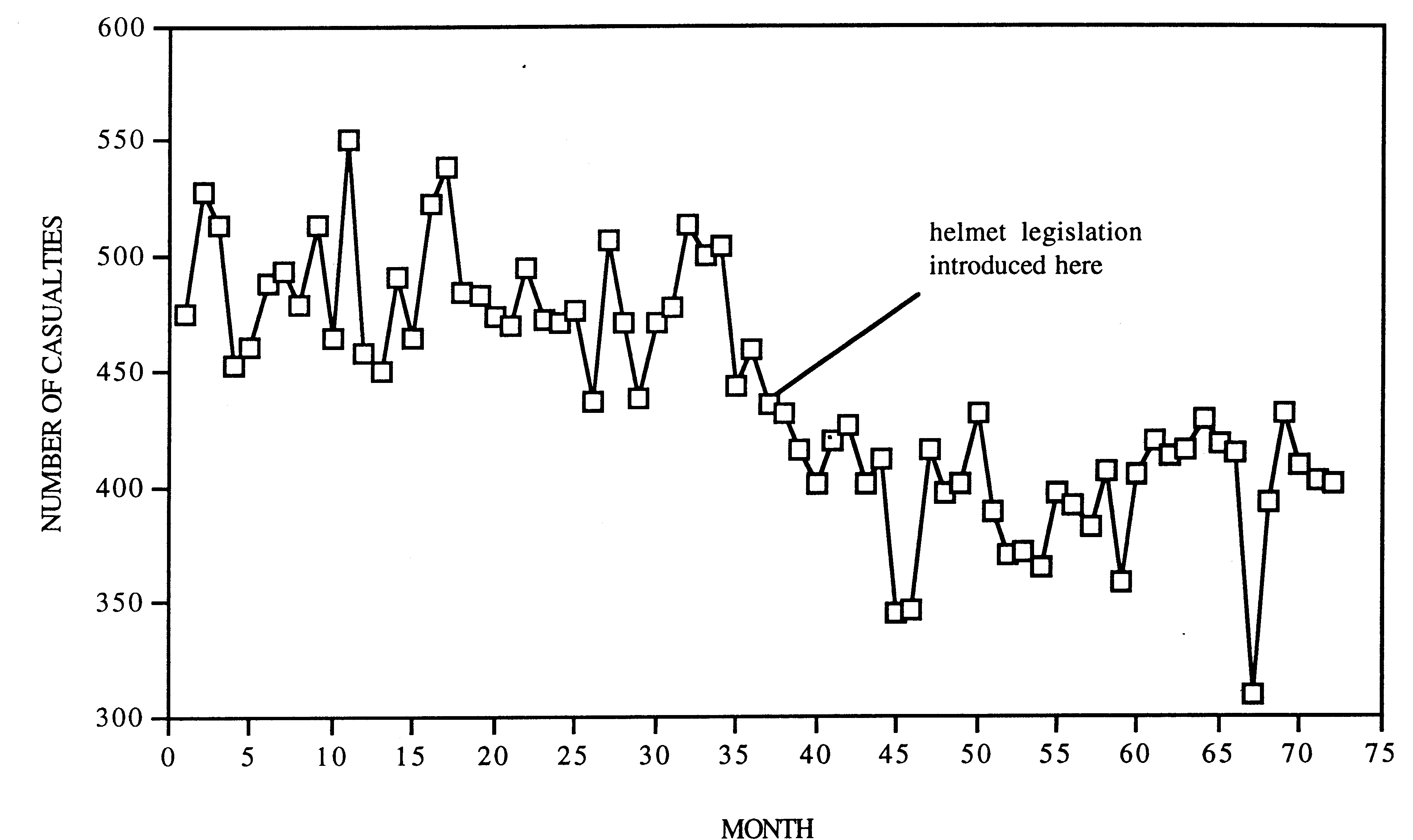 Fig 5. NSW Head injury and helmet
Fig 5. NSW Head injury and helmet