Review article: amphetamines and related drugs of abuse
Emergency Medicine Australasia (2008) 20, 391–402 REVIEW ARTICLE
Review article: Amphetamines and relateddrugs of abuse
Shaun L Greene, Fergus Kerr and George BraitbergDepartment of Emergency Medicine, Austin Health and Victorian Poisons Information Service,Melbourne, Victoria, Australia
Abstract
Acute amphetamine toxicity is a relatively common clinical scenario facing the Australa-sian emergency medicine physician. Rates of use in Australasia are amongst the highest inthe world. Clinical effects are a consequence of peripheral and central adrenergic stimula-tion producing a sympathomimetic toxidrome and a spectrum of central nervous systemeffects. Assessment aims to detect the myriad of possible complications related to acuteamphetamine exposure and to institute interventions to limit associated morbidity andmortality. Meticulous supportive care aided by judicial use of benzodiazepines forms thecornerstone of management. Beta blockers are contraindicated in managing cardiovascularcomplications. Agitation and hyperthermia must be treated aggressively. Discharge ofnon-admitted patients from the emergency department should only occur once physiologi-cal parameters and mental state have returned to normal. All patients should receiveeducation regarding the dangers of amphetamine use. Key words: Introduction
An estimated half a million Australians used an
Amphetamine was first synthesized in Germany in
amphetamine-type stimulant during a 12-month period
1887. Plant-derived stimulant ephedra (ma huang) con-
in 2003–2004, making amphetamines the second
taining the alkaloids ephedrine and pseudoephridrine
most commonly used illicit drugs in Australia after
has been used in traditional Chinese medicine for over
cannabis.1,2 Amphetamines and related substances are
5000 years to treat asthma and the common cold.
widely abused in New Zealand;3 hence, amphetamine
Amphetamine was not used clinically until the 1920s
toxicity is a relatively common clinical scenario facing
following reduced availability of ephedrine, used to
the Australasian emergency medicine physician.
treat asthma. The discovery of dextroamphetamine and
Shaun Greene, Austin Health, 145 Studley Road, PO Box 5555, Heidelberg, Vic. 3084, Australia. Email: shaun.greene@austin.org.au or
Shaun L Greene, MBChB, MSc, Registrar in Emergency Medicine, Clinical Toxicologist; Fergus Kerr, MB BS, FACEM, MPH, Director EmergencyMedicine, Clinical Toxicologist; George Braitberg, MB BS, FACEM, FACMT Dip Epi Biostats, Professor of Emergency Medicine, Director ofEmergency Medicine, Clinical Toxicologist.
2008 The AuthorsJournal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
methamphetamine quickly followed. A nasal deconges-
sparse. A recent prospective 3-month study in Western
tant containing amphetamine was marketed in 1932.4
Australia found presentations related directly or casu-
Widespread abuse led the Food and Drug Administra-
ally to amphetamine use comprised 1.2% of all ED
tion (FDA) to ban amphetamine inhalers in 1959.5
presentations, with an associated admission rate of
Amphetamines were widely used as stimulants
39.7% and psychiatry service assessment in 37.2% of
during World War II, and for diverse clinical conditions,
cases.20 An Australasian Triage Scale of 1, 2 or 3 was
including shock, barbiturate overdose, encephalitis,
assigned to 66.7% of patients, indicating a high degree
obesity and postural hypotension. Over 10 billion
tablets containing amphetamines had been legally
manufactured by 1970; the majority were used illicitly.6,7
methamphetamine-related in Australia in 2005 (a rate
Following passage of the Controlled Substance Act in
of 5.9/million persons), a reduction from seventy-five
1970 in the USA, amphetamine abuse rates decreased.8
(6.6/million persons) in 2004.16 However, 26 deaths
However, the 1980s witnessed an explosion in clandes-
were classified as a direct result of methamphetamine
tine production of ‘designer’ amphetamines, the best
toxicity in 2005 compared with 17 in 2004.16 Although
methamphetamine deaths attract regular media atten-
(MDMA) and 3,4-methylenedioxyethamphetamine.9–11
tion, opioid-related deaths are far greater: 374 deaths
A later resurgence in methamphetamine abuse fol-
were reported in 2005 (32.5/million persons).16,21,22
lowed production of a high-purity formulation knownas ‘ice’.12,13 The 1990s rave scene brought widespreaduse of MDMA and methamphetamine in Europe,
Structure and pharmacology
North America and Australasia. Production of otherdrugs with similar chemical structures, including
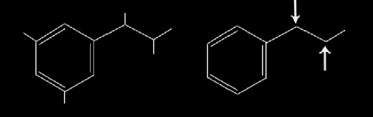
Amphetamines are derived from phenylethylamines;
1-benzylpiperazine (BZP), followed.1–3,14–18
structural similarities to adrenaline are illustratedin Figure 1. Phenylethylamines are primarily central
Epidemiology
nervous system (CNS) stimulants. Substitution of addi-tional chemical entities to ethyl chain carbon atoms
Although the estimated 620 000 amphetamine users in
(arrows in Fig. 1), aromatic ring and terminal amino
Oceania account for only 2.5% of total worldwide users
nitrogen produces variable clinical effects.
(estimated 24.8 million), this region has the highest total
Entry of amphetamines into the cell cytoplasm occurs
rate (2.9%) of use among 15- to 64-year-olds.14 MDMA
predominantly via neuronal monoamine re-uptake
use among Australasians is estimated at 3.0%, com-
transporters.23 Amphetamines also act as substrate for
pared with a global average of 0.2%.14 The Australian
these transporters, stimulating an exchange diffusion
2007 National Drug Strategy Household Survey of
25 000 Australians aged 14 years and over found that
transmitter release. Inhibition of cellular monoamine
2.3% reported use of amphetamine/methamphetamine
re-uptake therefore occurs via direct drug-monoamine
in the previous 12 months, a decrease from 3.2% in
competition for the re-uptake transporter, and trans-
2004 and 3.4% in 2001.1 Lifetime use of amphetamine/
porter stimulation to act as a reverse carrier.23 Am-
methamphetamine is higher among men (7.7%) versus
phetamines inhibit intracellular vesicular monoamine
women (4.9%).1 Lifetime use of amphetamine in NewZealand was reported at 9% in 2004.3
During 2006, 15% of New Zealanders aged 13–
45 years reported using legally available ‘party pills’,
containing BZP or trifluorophenylmethylpiperazine(TFMPP).17 Legislation was passed in April 2008,
classifying BZP as a restricted substance (C1).19
ED experience
Published information documenting amphetamine-
Figure 1.
Chemical structure of adrenaline and phenylethy-
related ED attendances globally and in Australasia is
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
transporter 2, reducing vesicular monoamine storage
mixed with other pharmacologically active ingredients,
and increasing cytoplasmic monoamine concentra-
including ephridrine, cocaine and heroin. Amphet-
tions.24 Ultimately, acute toxicity is produced by
amines used for medicinal purposes can be abused:
excessive extracellular noradrenaline, dopamine and
methylphenidate used to treat ADHD and the anti-
serotonin. The most obvious clinical manifestation
obesity drug phentermine (Adipex-p, fastin).
is the alpha- and beta-adrenergic receptor-mediatedsympathomimetic toxidrome.
Amphetamines are lipophilic weak bases, have large
Clinical effects
volumes of distribution and are not readily metabolizedby monoamine oxidase or catechol-O-methyl trans-
Amphetamines produce a wide range of clinical effects
ferase.25 As a group, amphetamines generally have good
via modulation of peripheral and central catecholamine
bioavailability, moderate to long durations of action
neurotransmitter function. The typical clinical picture
(half-lives 2.5–30 h), and are not amenable to extracor-
is one of adrenergic system overdrive producing a
poreal elimination methods. Long half-lives can lead to
sympathomimetic toxidrome of tachycardia, tachyp-
accumulation following repetitive dosing (associated
noea, diaphoresis, hypertension, hyperthermia, mydria-
with binge use).26 Routes of elimination vary, but are
sis, hyperreflexia, tremor and a wide range of CNS
predominantly a combination of hepatic biotransforma-
states (hyperarousal, agitation, paranoia, hallucinations,
tion and urine pH-dependent renal excretion.25,26
dis-inhibition, seizures and coma).9,28–30
Hyperthermia, hepatotoxicity and electrolyte abnor-
malities are possible following amphetamine use.9,29,31
Manufacture
Serotonergic amphetamines can produce clinical mani-festations of serotonin toxicity.9,30,31 Clinical manifesta-
tions of acute and chronic amphetamine toxicities are
pharmaceutical, industrial and agricultural products
available to the public. Other derivatives, includingMDMA, are more difficult to synthesize. Home produc-tion methods are easily found with the aid of an Internet
Selected amphetamines
Methamphetamine is produced through reduction of
Characteristics of the commonly abused amphetamines
ephredrine or pseudoephedrine.27 Illicit methamphet-
are summarized in Tables 2–4. Associated slang names
amine production is not without risk. Corrosive injuries,
dermal and inhalation burns, and chemical explosionscan occur.5,27
Methamphetamine
Methamphetamine is often mixed or ‘cut’ with other
substances, including caffeine or talc, to add bulk,
Improved production methods produce methamphet-
improving profit margin. Amphetamines are often
amine in the dextro-isomer form that is 80–90% pure.13
Clinical manifestations of amphetamine toxicity
Tachycardia, hypertension, aortic dissection, arrhythmias, vasospasm, acute coronary syndrome,
hypotension (late sign), acute cardiomyopathy
Agitation, paranoia, euphoria, hallucinations, bruxism, hyperreflexia, intracerebral haemorrhage,
choreoathetoid movements, anorexia, hyperthermia, seizures, coma
Mydriasis, diaphoresis, tremor, tachypnoea
Hepatitis, nausea, vomiting, diarrhoea, gastrointestinal ischaemia
Hyponatraemia (dilutional/SIADH), acidosis
Behavioural/psychiatric illness, cardiomyopathy, cardiac valve disease, pulmonary hypertension, vasculitis
ARDS, Adult respiratory distress syndrome; SIADH, syndrome inappropriate anti diuretic hormone.
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
Predominant sympathomimetic actions, greater peripheral sympathomimetic effects than
VD 3–5 L/kg, 20% plasma protein bound, hepatic metabolism, 30% renal elimination, 10–13 h,
Powder or tablet. Ingested, injected, vaporized (smoked), insufflated (snorted), taken
Euphoria, hyper-stimulation, increased stamina and sexual drive, decreased appetite
Predominant sympathomimetic actions, most potent cardiovascular effects of all amphetamines, greater central
VD 3–7 L/kg, hepatic metabolism, 40–50% renal elimination, half-life 8–12 h, active metabolites – amphetamine,
Powder, tablet, crystal, liquid. Ingested, injected, vaporized (smoked), insufflated (snorted), taken sublingually
Euphoria, increased stamina, energy, concentration and sexual drive, decreased appetite
Bruxism, agitation, paranoia, formication, violent behaviour, high-risk sexual activity
Properties of 3,4-methylenedioxymethamphetamine5,11,27,33
Potent serotonergic agent, less sympathomimetic effects than amphetamine/methamphetamine
35% hepatic metabolism subject to CYP2D6 genetic polymorphism, 65% renal elimination,
half-life 7–9 h, active metabolite 3,4-methylenedioxyamphetamine
Colourful tablets most common, 50–200 mg per dose
‘enactogen’ – euphoria, inner peace, social facilitation, ‘heightens sexuality and expands
consciousness’, mild hallucinogenic effects
Bruxism, hyperthermia, ataxia, confusion, hyponatraemia (SIADH), hepatitis, muscular rigidity,
rhabdomyolysis, DIC, renal failure, hypotension, serotonin syndrome, chronic mood/memorydisturbances
3,4-Methylenedioxymethamphetamine (love drug), 3,4-Methylenedioxyethamphetamine (Eve)
SIADH, syndrome inappropriate anti-diuretic hormone; DIC, disseminated intravascular coagulation.
Slang names of commonly abused amphetamines and piperazines
Amp, Bennies, Black beauties, Browns, Cranks, Fives, Goey, Hearts, Louee, Speed, Uppers,
Solid – Meth, Speed, Whiz, Fast, Base, Pure, Point, P, Rabbit, Tail, WaxLiquid – Red Speed, Liquid red, Leopard’s blood, Ox bloodCrystal – Ice, d-meth, Glass, Crystal, Batu, Shabu
Adam, Bart Simpson, Clarity, Disco biscuits Essence, E, Ecstasy, Love drug, Red and black,
Bliss, BNZ, Bolts, Charge, Exodus, Frenzy, Goodstuff, Grins, Herbal Ecstasy, Herbal party
pills, Jumps, Kandy, Legal ecstasy, Legal E, Legal X, Nemesis, Red hearts, Sliver bullet
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
Crystal methamphetamine is the hydrochloride salt
Gee et al. documented 80 BZP presentations to a
of methamphetamine. Heating and inhaling crystal-
major New Zealand urban ED over a 6-month period
line methamphetamine fumes (or ‘chasing the white
in 2005.18 Fifteen (19%) suffered generalized seizures,
dragon’) is the most rapid method of obtaining a ‘high’.34
two had status epilepticus and severe respiratory and
Methamphetamine hydrochloride is dissolvable in
metabolic acidosis. Common adverse effects (>15%
water and can be injected or ingested as a liquid. Meth-
of patients) included palpitations, vomiting, collapse,
amphetamine powder is readily absorbed across mucus
membranes and can be snorted, ingested or insertedrectally. Powder can be injected, as a ‘dry shot’.32
Assessment and management
drive and dis-inhibition. Widespread use in the gaycommunity in the USA has increased rates of HIV
Immediate management
seroconversion and transmission of other sexuallytransmitted diseases.35,36
Airway, breathing and circulation are initial priorities. Significant agitation, hyperthermia, cardiovascular, neu-rological or respiratory compromise mandates triage to a
Substituted amphetamines
resuscitation area, and immediate assessment and treat-
MDMA and related amphetamines with additions to
ment. Patients with altered conscious state require a
the aromatic ring structure are known as substituted
bedside blood sugar level determination. Cardiac arrest
amphetamines. Clinically, they are characterized by
is treated using advanced life support protocols. Poten-
enhanced hallucinogenic properties and potent CNS
tial hyperkalaemia caused by muscle damage and acido-
sis should be considered early during resuscitation.
Para-methoxyamphetamine is a powerful halluci-
nogen and sympathomimetic, associated with intra-cerebral haemorrhage, hyperthermia and death.39
Assessment
2,5-Dimethoxy-4-methylamphetamine is a potent hal-lucinogen with narrow therapeutic index, produc-
ing perceptual distortions and euphoria.40 4-Bromo-
2,5-dimethoxyamphetamine is an extremely potent
(as reported by the patient), method, quantity and
time of exposure. Knowledge of place of exposure is
effects, and is commonly used as a preparation on
important. Patients who have been in crowded clubs
impregnated paper, similar to Lysergic acid diethyla-
with high ambient temperatures are at increased risk
mide (LSD). 4-Bromo-2,5-dimethoxyamphetamine pro-
duces severe arterial spasm. One limb amputation has
Complaints of chest pain, palpitations, dizziness,
been reported.41 4-Bromo-2,5-dimethoxyphenethylamine
headache, focal neurological changes and visual distur-
(2CB, MFT), a popular rave drug known as ‘nexus’,
bance suggest significant toxicity and require rapid
produces relaxation, euphoria and altered perception.42
Relevant history following amphetamine exposure
Piperazines
Presumed identity, route, time and quantity of amphetamine
BZP and TFMPP are members of the piperazine family
and therefore not strictly amphetamines. Related chemi-
Presence of chest pain, palpitations, headache, focal neurological
cal structures cause similar clinical effects, so that even
regular amphetamine users are often unable to differen-
Coingestants including ethanol and other stimulant drugs
tiate between them.43 BZP inhibits re-uptake of dopam-
Quantity of water and other fluids ingested
ine and serotonin and stimulates peripheral alpha-2
Use of any CYP2D6 inhibitors (including SSRI, MAOI)
receptors, but exhibits lower potency than amphet-
Coexisting cardiac, respiratory or neurological disease
amine.44,45 TFMPP is more serotonergic and produces
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
Co-ingestants, including mononamine oxidase inhi-
Clinical signs indicating significant amphetamine
bitors, tricyclic antidepressants and other stimulant
drugs, are synergistic.50 Cocaine is a hepatic microsomal
CYP2D6 enzyme inhibitor and may reduce amphet-
amine (particularly MDMA) metabolism.51 A history of
fluid intake, including ethanol and water, is relevant.
Excessive fluid intake in an attempt to avoid dehydra-
Medicinal drug use is important; CYP2D6 inhibi-
tors, including the protease inhibitor ritonavir, some
Coronary artery spasm and related sequelaeAutonomic instability and other major disturbance of
selective serotonin re-uptake inhibitors, quinidine, imi-
pramine and thioridazine, may prolong amphetaminetoxicity by reducing hepatic metabolism.53
Patients with underlying seizure disorders or cardio-
• Electrolytes and renal function to exclude secondary
respiratory disease will be less tolerant of amphetamine
metabolic abnormalities, including hyponatraemia
toxicity. The prevalence of CYP2D6 poor-metabolizer
phenotype is 3–10% among Caucasians; these individu-
• Creatinine kinase to look for rhabdomyolysis
als might be more susceptible to amphetamines metabo-
• Coagulation screen to exclude disseminated intravas-
Young patients presenting to the ED with anxiety,
• Liver function tests looking for hepatitis
psychosis, agitation, seizures, supra-ventricular tachy-
• Arterial blood gas analysis to detect inadequate res-
cardias, stroke, hypertension, non-cardiogenic pulmo-
piratory function, a metabolic acidosis secondary to
nary oedema, pulmonary hypertension, vasculitis
seizures, dehydration or inadequate tissue perfusion,
and cardiomyopathy should be asked about ampheta-
or a respiratory alkalosis secondary to direct amphet-
• Serial cardiac enzymes to assess possible acute coro-
Examination
• Electrocardiogram (serial) to assess for possible acute
coronary syndrome/dysrhythmias, or underlying
Examination will typically reveal signs of sympatho-
mimetic overdrive as summarized in Table 1. Some
• A chest X-ray looking for evidence of aortic dis-
patients will be clinically well and a focused examina-
section, pneumothorax, pulmonary aspiration or pos-
tion directed at their presenting complaint will be
• An abdominal X-ray if there is suspicion of ingested
After airway, breathing and circulation assess-
ment, patients with significant amphetamine toxicity
• Computerized tomography of the brain to look for
(particularly those with altered conscious state) require
evidence of stroke or cerebral oedema (a normal com-
a more structured examination. Toxicity may be present
puted tomography brain scan does not exclude these
in multiple organ systems and examination should
diagnoses) or possible trauma-related injury
seek to detect signs of life-threatening neurological,
• Coronary artery angiography to assess possible
cardiovascular, autonomic and metabolic disturbances
amphetamine-induced coronary artery vasospasm or
• Echocardiography looking for cardiomyopathy
Investigations
Urine drug amphetamine screens have poor sensitiv-
ity and should not be a routine component of assess-
Investigations should be determined by specific find-
ment. A positive urine amphetamine drug screen does
ings on initial history and examination, and overall
not definitively indicate that current illness is secondary
seriousness of clinical toxicity. Investigations may
to amphetamine toxicity.5,56,57 Amphetamines used
days before ED presentation can produce positive urine
• Bedside blood sugar level to exclude hypoglycaemia
results.5 Cold preparations containing substances with
similar structures can produce false positive results.56,57
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
Some amphetamines, including MDMA, are not reliably
of aspiration during subsequent seizures or vomiting.58
Patients with severe toxicity who are intubated might
Serum amphetamine concentrations are not available
benefit from one dose of AC via a nasogastric tube.
in time to influence acute management and should not
Although relatively rare in Australia, the possibility
be routinely requested. Amphetamine and other stimu-
of amphetamine leakage from packets within the gas-
lant drug toxicity is initially a clinical diagnosis. Early
trointestinal tract ingested by ‘body packers’ should be
management of amphetamine, cocaine and piperazine
considered in cases of severe ongoing clinical amphet-
toxicity is identical and biochemical identification is
amine toxicity. Simple digital examination of oral and
seldom required during ED management. Serum
rectal cavities early during management might detect a
amphetamine concentrations are indicated in medico-
leaking packet, preventing ongoing exposure.
legal circumstances, including suspected child abuse. Enhanced elimination Differential diagnosis
Amphetamines are weak bases.5,27 Urine acidification,
while theoretically enhancing amphetamine elimination,
system stimulation might mimic amphetamine toxi-
is contraindicated because it will potentiate adverse
city and, therefore, the differential diagnosis is wide
effects of rhabdomyolysis (increased myoglobin preci-
pitation in acidic urine) and worsen any metabolicacidosis.59 Haemoperfusion, haemodialysis and haemo-filtration are ineffective.5,27
General management
Meticulous supportive care is essential. Rapid correction
Specific management
of hypoxia, hypotension, hyperthermia, acid-base andmetabolic abnormalities, and raised intracranial pres-
Treatments for amphetamine-associated toxicity are
sure will reduce associated morbidity and mortality. Decontamination Agitation
The role of activated charcoal (AC) in managing
amphetamine toxicity is limited for the majority of
aggressively. Associated sympathomimetic overdrive
patients. Although AC potentially decreases amphet-
increases risk of hypertension, hyperthermia, acidosis,
amine absorption if administered within 1 h of inges-
rhabdomyolysis and malignant dysrhythmias. Rapid
tion, most patients don’t present within this time frame.
control of agitation minimizes these complications and
AC has not been shown to alter clinical outcome.58
allows safe, controlled patient assessment.
Potential benefits of AC (adult dose 50 g orally or via a
Agitated patients should be cared for in a quiet
nasogastric tube) need to be weighed against dangers
environment, which still allows provision of criticalcare. Initially, patients may require physical restraint,
Differential diagnosis of amphetamine toxicity
but only to facilitate rapid pharmacological sedation. Ideally, pharmacological agents are administered
intravenously, allowing titration to clinical effect and
achieving rapid onset of action. Obtaining i.v. access
might be technically difficult or unsafe; initial i.m.
administration will facilitate eventual i.v. access.
Benzodiazepines are first-line agents for controll-
ing agitation.60–63 By facilitating gamma-aminobutyric
acid (GABA) receptor-mediated CNS inhibition, benzo-
diazepines are indirect antagonists of amphetamine-
stimulated sympathomimetic agitation, reducing CNS
stimulation, heart rate, blood pressure and muscle
monoamine-oxidase inhibitor; LSD, lysergic acid diethylamide.
activity. Benzodiazepines should be administered in
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
Specific interventions for non-cardiovascular related
Table 10.
Specific interventions for cardiovascular related
Midazolam – 5–10 mg i.m. initially if i.v. access
Agitation associated with paranoia/hallucinations
Droperidol – 2–5 mg i.v. (beware seizures, hypotension)
Dysrhythmias (avoid moderate to long acting beta-blockers)
Benzodiazepines if associated with CNS overstimulation
Sedation with airway control using thiopentone/propofol
Verapamil – 5 mg i.v. (beware of hypotension)
Computed tomography brain scan in cases of incomplete
Decreased conscious level (remember hyponatraemia)
Hyponatraemia (beware central pontine myelinolysis)
A butyrophenone is appropriate in patients with
delirium or hallucinations and normal cardiovascular
Fluid restrict in non-dehydrated patients
Cautious administration of 3% saline in severe symptomatic
cases (sodium concentration <115 mmol/L) – seek advice
Seizures and reduced conscious state
Benzodiazepines – diazepam or clonazepam bolusesActive cooling measures – ice packs or baths
Amphetamine-induced seizures are generally short-
lived and respond to benzodiazepines.5,27 Phenobar-
5HT2 antagonist – cyproheptadine 12 mg orally or via a
bitone is a second-line agent. Unresponsive seizures
should be treated with general anaesthetic sedation
using thiopentone, propofol or midazolam. Pheny-
toin’s sodium channel-blocking properties and the
Urinary alkalinization (beware increased amphetamine
cardiotoxic properties of the i.v. preparation’s dilu-
ent (propylene glycol) can theoretically precipitatedysrhythmias.5,27
incremental boluses, titrated to clinical effect. Large
Hypertension, vasospasm and tachycardia can lead
doses are often required. Diazepam as an initial 5-mg
to intracerebral or subarachnoid haemorrhage, and cere-
dose, followed by 2.5- to 5-mg boluses every 2–5 min,
bral ischaemia or infarction. Any patient with reduced
can be given intravenously. Intramuscular midazolam
consciousness state or one who does not rapidly recover
is a good initial choice in patients with no i.v. access.
neurologically following a seizure requires intracranial
Antipsychotics, including droperidol, haloperidol and
imaging. Patients with hyponatraemia can present with
olanzapine lower seizure threshold, can induce hypoten-
seizures and reduced conscious state.
sion and dysrhythmias, impair heat dissipation, gener-ally have slower onset times and are not recommended
Movement disorders
as first-line agents for treatment of stimulant drug-induced agitation.61 Despite these concerns, there is little
Repetitive movement disorders, including teeth grind-
published evidence to support them. Antipsychotics
ing (bruxism, commonly seen with MDMA) and chore-
may therefore be used cautiously as second-line agents.
oathetoid movements, are caused by dopaminergic
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
stimulation of the nigrostriatal area, and usually settle
Amphetamine-induced hyperthermia must be treated
with observation. Oral or i.v. benzodiazepines are often
aggressively. Large i.v. doses of benzodiazepines
administered incrementally will control agitation andreduce muscle activity.69 Dehydration must be corrected
Hypertension
with i.v. crystalloid. Ice baths or placing ice packs inthe groin and axilla are effective methods of external
Hypertension can be severe, leading to intracranial
cooling. Neuromuscular paralysis and ventilatory
haemorrhage or seizures. In the presence of CNS stimu-
support should be instituted early in patients not
lation, benzodiazepines are first-line agents, used to
reduce sympathomimetic overdrive.5,27 Further control
Clinical evidence for the effectiveness of dantrolene in
of blood pressure should be achieved using alpha-
treating amphetamine-induced hyperthermia is sparse.
adrenergic receptor antagonists (oral prazosin or i.v.
phentolamine), glyceryl trinitrate (GTN) or nitroprus-
muscle contraction, has no CNS effect and may worsen
side. Beta-blockers are contraindicated as blockade of
amphetamine-induced hyperthermia.70 Dantrolene offers
beta2-receptors (mediating skeletal muscle vasodilation)
no theoretical advantage in this scenario over neuromus-
can produce unopposed alpha-receptor stimulation and
Chlorpromazine and the 5HT2a antagonist cypro-
heptadine appear efficacious in treating serotonin tox-
Dysrhythmias
icity,71 although evidence for both is limited to casereports.72 These drugs should be considered in cases of
Prehospital deaths are most likely secondary to malig-
amphetamine-related refractory hyperthermia. Cypro-
nant dysrhythmias.33 Isolated sinus tachycardia seldom
heptadine is administered orally (12 mg, then 8 mg
requires treatment, but will respond to benzodiazepines
every 8 hours for 24 hours, via a nasogastric tube in
if associated with a sympathomimetic toxidrome. Cor-
unconscious patients). Chlorpromazine can be admin-
rection of hypoxia, acidosis and metabolic abnormali-
istered as an i.v. infusion (12.5- to 25-mg initial infu-
ties minimizes risk of conduction abnormalities and
sion over 1 h), but can cause hypotension. One animal
improves efficacy of anti-dysrhythmic drugs.
study has shown beneficial effects of carvedilol
Supraventricular tachycardia should be managed
(alpha1-receptor and beta1,2,3-receptor antagonist) in
using conventional therapies, including adenosine,
treating MDMA-induced hyperthermia.68 Carvedilol
verapamil and electrical cardioversion. If a beta-
and olanzepine (5-HT2A and alpha1-receptor antago-
blocker is necessary, esmolol should be considered
nist) might be used routinely in the future, but are not
to minimize risk of uncontrolled hypertension.5,27
Ventricular dysrhythmias are managed using standardprotocols. Hyponatraemia Hyperthermia
Patients presenting with altered conscious state orseizures following amphetamine exposure may have
Hyperthermia has been associated with amphetamine-
related deaths, particularly MDMA.9,30,33 Hyperthermia
prompts many users to ingest large quantities of water,
is more likely following MDMA ingestion in crowded,
producing dilutional hyponatraemia.52 MDMA-induced
noisy environments with high ambient tempera-
symdrome of inappropriate anti-diuretic hormore
tures.47–49,63 MDMA-induced hyperthermia is often asso-
(SIADH) may interfere with compensatory mechanisms
ciated with clinical features of serotonin toxicity.9,30,33
Mechanisms underlying substituted amphetamine-
Hyponatraemia should be excluded early (via venous
induced hyperthermia are complex; however, serotonin
or arterial blood gas analysis if necessary) in patients
and noradrenaline neurotransmitter interaction with
with altered conscious state or seizures, preventing
5HT2a and beta3-receptors within vasculature and
inappropriate fluid therapy and worsening hypona-
brown adipose tissue appear to contribute.64–67 Animal
traemia. Mild to moderate hyponatraemia in a non-
studies demonstrate that beta3-receptor and alpha1-
dehydrated patient should resolve with fluid restriction.
Patients who do require i.v. fluids should receive
normal saline. Hypotonic fluid therapy will worsen
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
hyponatraemia. Hyponatraemia should be corrected
Chronic amphetamine abuse
over a similar time frame to which it occurred, but not ata total rate greater than 0.5 mmol/L/h during a 24-h
There has been considerable debate about long-term
effects of amphetamine and substituted amphetamines.
Severe hyponatraemia (<115 mmol/L) with coexist-
Animal and some human data have shown that long-
ing seizures or evidence of possible cerebral oedema
term exposure to MDMA is toxic to serotonergic neu-
should be treated cautiously with 3% saline to increase
rones.75,76 This datum has been postulated to support the
serum to a concentration where seizures terminate, but
notion that long-term MDMA abuse might be associated
not to a concentration above 120 mmol/L. In general
with chronic depression as a result of changes in CNS
an increase of Na of 4–6 mmol/L is enough to halt pro-
gression of symptoms in severe hyponatraemia. Sodium required to obtain a concentration of 120 mmo/L = (120 - sodium concentration) ¥ 0.6 ¥ weight (kg).
Alternatively, X mL/kg of 3% saline will raise thesodium by X mmol/L. Rapid correction of sodium
Amphetamine abuse in Australia and New Zealand is
should only be undertaken if clinically necessary and
common. Patients present to ED with varying degrees
can produce central pontine myelinolysis.
of amphetamine-related toxicity and secondary compli-cations. Agitation and hyperthermia are treated aggres-sively, initially with i.v. benzodiazepines. Beta-blockers
Rhabdomyolysis
must be avoided in treating hypertension and dysrhyth-mias because of unopposed alpha-receptor stimulation
MDMA increases muscle motor activity, reduces muscle
and potential worsening toxicity. Focal neurological
cell ATP stores and impairs muscle cell energy produc-
signs, seizures without rapid neurological recovery and
tion, potentially producing rhabdomyolysis.74 Rhab-
reduced conscious level require intracranial imaging.
domyolysis should be treated with i.v. fluid therapy to
Hyponatraemia should be considered in cases of altered
ensure a urine output of >2 mL/kg/h. Agitation and
conscious state or seizures and corrected cautiously to
hyperthermia should be treated aggressively to limit
avoid secondary complication. Secondary metabolic
further muscle damage. Although urinary alkalinization
complications and rhabdomyolysis must be excluded.
might be beneficial in treating rhabdomyolysis, it willinhibit amphetamine elimination and prolong toxicity.5
Competing interests
George Braitberg is a section (toxicology) editor forEmergency Medicine Australasia. Disposition
Patients discharged from the ED following treatment ofamphetamine toxicity should have a normal consciousstate, temperature and cardiovascular status. Those at
References
risk of rhabdomyolysis (prolonged physical activity,high temperature or period of decreased conscious state
Australian Institute of Health and Welfare, Canberra. 2007
with possible tissue compression) should have creati-
National Drug Strategy Household Survey. April 2008. [Cited
nine kinase and renal function checked. Patients with
31 May 2008.] Available from URL: publications/index.cfm/title/10579
severe toxicity require admission to a critical care bed.
Australian Institute of Health and Welfare, Canberra. Statistics
Those with moderate toxicity requiring a period of
on drug use in Australia 2006. April 2007. [Cited 13 Aug 2007.]
observation or those with associated psychiatric illness
will require admission to an observation, general
medical or psychiatry bed depending on local protocols.
Wilkins C, Sweetsur P, Casswell S. Recent population trends
Patient education regarding dangers of amphetamine
in amphetamine use in New Zealand: comparisons of findingsfrom national household drug surveying in 1998, 2001, and 2003.
use should be a part of general management. In particu-
Med. J. N. Z. 2006;119: 1–10.
lar, the commonly held misconceptions ‘amphetamines
Anderson RJ, Reed WG, Hillis LD. History, epidemiology, and
do not cause harm unless contaminated’ and ‘are a safe
medical complications of nasal inhaler abuse. Clin. Toxicol. 1982;
alternative to cocaine’ should be addressed. 19: 95–107.
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
Chiang WK. Amphetamines. In: Goldfrank LR ed. Goldfrank’s
24. Brown JM, Hanson GR, Fleckenstein AE. Methamphetamine
Toxicological Emergencies, 7th edn. New York: McGraw-Hill,
rapidly descreases vesicular dopamine uptake. J. Neurochem.
2000; 74: 2221–3.
Blum K. Central nervous system stimulants. In: Blum K ed.
25. Cho AK, Wright J. Pathways of metabolism of amphetamine. LifeHandbook of Arousable Drugs. New York: Gardner, 1984; 305–47. Sci. 1978; 22: 363–71.
Karch SB. Synthetic stimulants. In: Karch SB ed. The Pathology
26. Baselt RC. Disposition of Drugs and Toxic Chemicals in Man, 6th
of Drug Abuse. Boca Raton: CRC Press, 1993; 165–234.
edn. Foster City, California: Chemical Toxicology Institute, 2000.
Klatt EC, Montgomery S, Nemiki T, Noguchi T. Misrepresenta-
27. McKinney E, Palmer RB. Amphetamines and Derivatives. In:
tion of stimulant street drugs: a decade of experience in an
Brent JB, Wallace KL, Burkhart KK, Phillips SD, Donovan JW, eds.
analysis program. J. Toxicol. Clin. Toxicol. 1986; 24: 441–50. Critical Care Toxicology. Philadelphia: Elsevier, 2005; 761–76.
Henry JA, Jerrreys KJ, Dawling S. Toxicity and deaths from
28. Dowling GP, McDonough ET, Bost RO. ‘Eve’, ‘ecstasy’. A report
3,4-methylenedioxymethamphetamine (‘ecstasy’). Lancet 1992;
of five deaths associated with MDEA and MDMA. JAMA 1987;
340: 384–7. 257: 1615–17.
10. Jerrad DA. Designer drugs – a current perspective. J. Emerg.
29. Derlet RW, Rice P, Horowitz BZ, Lord RV. Amphetamine
Med. 1990; 8: 733–41.
toxicity. Experience with 127 cases. J. Emerg. Med. 1989; 7:
11. Randal T. Ecstasy-fuelled ‘rave’ parties become dances of death
for English youths. JAMA 1992; 268: 1505–6.
30. Greene SL, Dargan PI, O’Connor N, Jones AL, Keins M. Multiple
12. Cho AK. Ice. A new dosage form of an old drug. Science 1990;
toxicity from 3,4-methylenedioxymethamphetamine (‘ecstasy’). 249: 631–4. Am. J. Emerg. Med. 2003; 21: 121–4.
13. Derlet RW, Heischober B. Methamphetamine. Stimulant of the
31. Gowing LR, Henry-Edwards SM, Irvine RJ, Ali RL. The health
1990s? West J. Med. 1990, 2006; 153: 625–8.
effects of ecstasy: a literature review. Drug Alcohol Rev. 2002; 21: 53–63.
14. United Nations Office on Drugs and Crime. 2007 World DrugReport. [Cited 15 Aug 2007.] Available from URL:
32. Matsumoto T, Kamijo A, Miyakawa T, Endo K, Yabana T,
unodc.org/pdf/research/wdr07/WDR_2007.pdf
Kishimoto H, Okudaira K, Iseki E, Sakai T, Kosaka K. Metham-phetamine in Japan: the consequences of methamphetamine
15. Australian Crime Commission. Illicit Drug Data Report 2004–05.
abuse as a function of route of administration. Addiction 2002;
Canberra: ACC, 2006. [Cited 13 Aug 2007.] Available from URL:
97: 809–17.
33. Hall Ap Henry JA. Acute toxic effects of ‘Ecstasy’ (MDMA) and
related compounds: overview of pathophysiology and clinical
16. Degenhardt L, Roxburgh A. 2005 Cocaine and Methamphet-
management. Br. J. Anaesth. 2006; 96: 678–85. amine Related Drug-Deaths in Australia. Sydney: The NationalDrug and Alcohol Research Centre University of New South
34. Rawson RA, Condon TP. Why do we need an Addiction supple-
Wales, 2007. [Cited 13 Aug 2007.] Available from URL:
ment focused on methamphetamine? Addiction 2007; 102: 1–4.
35. Danta M, Brown D, Bhagani S et al. Recent epidemic of acute
17. Wilkins C, Girling M, Sweetsur P, Huckle T, Huakau J. Legal
hepatitis C virus in HIV-positive men who have sex with men
Party Pill Use in New Zealand. Auckland: Centre for Social and
linked to high-risk sexual behaviours. AIDS 2007; 21: 983–91.
Health Outcomes research and Evaluation (SHORE), Massey
36. Gonzales R, Marinelli-Casey P, Shoptaw S, Ang A, Rawson RA.
University, 2007. [Cited 13 Aug 2007.] Available from URL:
Hepatitis C virus infection among methamphetamine-dependant
individuals in outpatient treatment. J. Subst. Abuse Treat. 2006;
18. Gee P, Richardson S, Woltersdorf W, Moore G. Toxic effects of
31: 195–202.
BZP-based party pills in humans: a prospective study in
37. Callaway CW, Johnson MP, Gold LH, Nicols DE, Geyer MA.
Christchurch, New Zealand. Med. J. N. Z. 2005; 118: 1–10.
Amphetamine derivatives induce locomotor hyperactivity by
19. New Zealand Government. Misuse of Drugs (Classification
acting as indirect serotonin agonists. Psychopharmacology (Berl)of BZP) Amendment Bill. [Cited 31 May 2007.] Available from
1991; 104: 293–301.
38. De Souza EB, Webster CL. Effects of MDMA and MDA on brain
serotonin neurons: evidence from neurochemical and autoradio-
graphic studies. NIDA Res. Monogr. 1989; 94: 196–222.
20. Gray FD, Fatovich DM, McCoubrie DL, Daly FF. Amphetamine-
39. Byward RW, Gilbert J, James R, Lokan RJ. Amphetamine deriva-
related presentations to an inner-city Emergency Department:
tive fatalities in South Australia – is ‘Ecstasy’ the culprit? Am. J.
a prospective evaluation. Med. J. Aust. 2007; 186: 336–9. Forensic Med. Pathol. 1998; 19: 261–5.
21. Williams R. Methamphetamine use on the rise. ABC News Bul-
40. Synder SH, Faillace L, Hollister L. 2,5-Dimethoxy-4-methyl-
amphetamine (STP). A new hallucinogenic drug. Science 1967;
22. Munro I. The Ice Age. The Age Newspaper 2007 24 Feb. Avail-
158: 669–70.
41. Bowen JS, Davis GB, Kearney TE, Bardin J. Diffuse vascular
spasm associated with 4-bromo-2,5-dimethoxyamphetamine
23. Fleckenstein AE, Volz TJ, Riddle EL, Gibb JW and Hanson GR.
ingestion. JAMA 1983; 249: 1477–9.
New insights into the mechanism of action of amphetamines.
42. De Boer D, Gijzels MJ, Bosman IJ, Maes RA. More data about the
Annu. Rev. Pharmacol. Toxicol. 2007; 47: 681–98.
psychoactive drug 2C-B. J. Anal. Toxicol. 1999; 23: 227–8.
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
43. Campbell H, Cline W, Evans M, Lloyd J, Peck AW. Comparison of
60. Solursh LP, Clement WR. Use of diazepam in hallucinogenic drug
the effects of dexamphetamine and 1-benzylpiperazine in former
crises. JAMA 1968; 205: 644–5.
addicts. Eur J. Clin. Pharmacol. 1973; 6: 170–6.
61. Whelan KR, Dargan PI, Jones AL, O’Connor N. Atypical antip-
44. Magyar K, Fekete MI, Tekes K, Torok TL. The action of trelibet,
sychotics not recommended for control of agitation in the emer-
a new antidepressant agent on [3H] noradrenaline release from
gency department. Emerg Med. J. 2004; 21: 649.
rabit pulmonary artery. Eur. J. Pharmacol. 1986; 130: 219–27.
62. Derlet RW, Albertson TE, Rice PE. Antagonism of cocaine,
45. Baumann MH, Clarke RD, Budzynski AG, Partilla JS, Blough BE,
Rothman RB. Effects of ‘Legal X’ piperazine analogs on dopam-
Biochem. Behav. 1990; 36: 745–9.
ine and serotonin release in rat brain. Ann. N. Y. Acad. Sci. 2004;
63. Freedman RR, Johanson CE, Tancer ME. Thermoregulatory
1025: 189–97.
46. Schechter MD. Use of TFMPP stimulus properties as a model
humans. Physchopharmacology (Berl) 2005; 183: 248–56.
of 5-HT1B receptor activation. Pharmacol. Biochem. Behav. 1988;
64. Gudelsky GA, Koeing JI, Meltzer HY. Thermoregulatory
31: 239–42.
responses to serotonin (5HT) stimulation in the rat. Evidence for
47. Hoehn R, Lasagna L. Effects of aggregation and temperature
opposing roles of 5-HT2 and 5HT1A receptors. Neuropharmacol-
on amphetamine toxicity in mice. Pyschopharmacolgia 1960; 12: ogy 1986; 25: 1307–13.
65. Blessing WW, Seaman B. 5-hydroxytryptamine (2A) receptors
48. Fantegrossi WE, Godlewski T, Karabenick RL, Stephens JM,
regulate sympathetic nerves constricting the cutaneous vascular
Ullrich T, Rice KC, Woods JH. Pharmacological characterization
beds in rabbits and rats. Neuroscience 2003; 117: 939–48.
of the effects of 3,4-methylenedioxymethamphetamine (‘ecstasy’)
66. Ootsuka Y, Blessing WW. Thermogenesis in brown adipose
and its enantiomers on lethality, core temperature, and locomotor
tissue: increase by 5-HT2A receptor activation and decrease by
activity in singly housed and crowded mice. Psychopharmacology
5-HT1A receptor activation in conscious rates. Neurosci. Lett.(Berl) 2003; 166: 202–11.
2006; 395: 170–4.
49. Gesi M, Ferrucci M, Giusiani M et al. Loud noise enhances nigros-
67. Zhao J, Cannon B, Nedegaard J. Alpha1-adrenergic stimulation
triatal dopamine toxicity induced by MDMA in mice. Microsc.
potentiates the thermogenic action of beta3-adrenoreceoptor-
Res. Tech. 2004; 64: 297–303.
generated cAMP in brown fat cells. J. Biol. Chem. 1997; 272:
50. Smilkstein MJ, Smolinske SC, Rumack BH. A case of MAO
inhibitor/MDMA interaction: agony after ecstasy. Clin. Toxicol. J.
68. Sprague JE, Moze P, Caden D, Rusyniak DE, Holmes C,
Toxicol. 1987; 25: 149–59.
Goldstein DS, Mills EM. Carvedilol reverses hyperther-
51. Shen H, He MM, Lui H, Wrighton SA, Wang L, Guo B, Li C.
Comparative metabolic capabilities and inhibitory profiles of
methylenedioxymethamphetamine (MDMA, ecstasy) in an
CYP2D6.1, CYP2D6.10, and CYP2D6.17. Drug Metab. Dispos.
animal model. Crit. Care Med. 2005; 33: 1311–16.
2007; 35: 1292–300.
69. Nisijima K, Shioda K, Yoshino T, Takano K, Kato S. Diazepam
and chlormethiazole attenuate the development of hyperthermia
in an animal model of the serotonin syndrome. Neurochem. Int.
methylenedioxymethamphetamine (MDMA, ‘ecstasy’) ingestion.
2003; 43: 155–64. QJM 2002; 95: 431–7.
70. Rusyniak DE, Banks ML, Mills EM, Sprague JE. Dantrolene use
53. de la Torre R, Fare M, Roset PN, Pizarro N, Abanades S, Segura
M, Segura J, Cami J. Human pharmacology of MDMA. pharma-
hyperthermia. Anesthesiology 2004; 101: 263.
cokinetics, metabolism, and disposition. Ther. Drug Monit. 2004;
71. Nisijima K, Yoshino T, Yui K, Katoh S. Potent serotonin (5HT2A)
26: 137–44.
receptor antagonists completely prevent the development of
54. Anderson T, Flockhart DA, Goldstein DB et al. Drug metabolis-
hyperthermia in an animal model of the serotonin syndrome.
ing enzymes: evidence for clinical utility of pharmacogenomic
Neurochem. Int. 2003; 43: 155–64.
tests. Clin. Pharmacol. Ther. 2005; 78: 559–81.
72. Gillman PK. The serotonin syndrome and its treatment.
55. Wilkinson GR. Drug metabolism and variability among patients
J. Psychopharmacol. 1999; 13: 100–9.
in drug response. NEJM 2005; 352: 2211–21.
73. Henry JA, Fallon JK, Kicman AT, Hutt AJ, Cowan DA, Forsling
56. Cody JT, Schwarzhoff R. Fluorescence polarization immunoassay
M. Low-dose MDMA (‘ecstasy’) induces vasopressin secretion.
of amphetamine, methamphetamine, and illicit amphetamine
Lancet 1998; 351: 1784.
analogues. J. Anal. Toxicol. 1993; 17: 23–33.
74. Curry SC, Chang D, Connor D. Drug and toxin-induced-
57. DiNicoula J, Jones R, Levine B, Smith ML. Evaluation of six
rhabdomyolysis. Ann. Emerg. Med. 1989; 18: 1068–84.
commercial amphetamine and methamphetamine immunoassays
75. Ricaurte GA, Yuan J, McCann UD. 3,4-methylenedioxy-
for cross-reactivity to phenylpropanolamine and ephedrine in
methamphetamine (‘ecstasy’)-induced serotonin neurotoxicity:
urine. J. Anal. Toxicol. 1992; 16: 211–13.
studies in animals. Neuropsychobiology 2000; 42: 5–10.
58. Chyka PA, Seger D, Krenzelok EP, Vale JA. American Academy
76. McCann UD, Eligulashvili V, Ricaurte GA. 3,4-methylenedioxy-
of Clinical Toxicology; European Association of Poisons Centres
methamphetamine (‘ecstasy’)-induced serotonin neurotoxicity:
and Clinical Toxicologists. Position paper: single dose activated
clinical studies. Neuropsychobiology 2000; 42: 11–16.
charcoal. Clin. Toxicol. 2005; 43: 61–87.
77. Ricaurte GA, McCann UD. Assessing long-term effects of MDMA
59. Cury SC, Chand D, Connor D. Drug and toxin induced rhabdomy-
(Ecstasy). Lancet 2001; 358: 1831–2.
olysis. Ann. Emerg Med. 1989; 18: 1068–84.
Journal compilation 2008 Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine
Welcome Thank you for choosing Texas Health Presbyterian Hospital Kaufman for outpatient surgery. Our goal is to make your experience at our facility a positive one. Sometimes, medical tests and procedures can make you a little uneasy, but we want you to know you can feel comfortable here. We believe when patients have a good idea of what to expect, typically, the overall experience is be
FDA REQUIRED READING Blood Donor Education Materials MAKING YOUR BLOOD DONATION SAFE Thank you for coming in today! This information sheet explains how YOU can help us make the donation process safe for yourself and patients who might receive your blood. PLEASE READ THIS INFORMATION BEFORE YOU DONATE! If you have any questions now or anytime during the screening process
 methamphetamine quickly followed. A nasal deconges-
sparse. A recent prospective 3-month study in Western
tant containing amphetamine was marketed in 1932.4
Australia found presentations related directly or casu-
Widespread abuse led the Food and Drug Administra-
ally to amphetamine use comprised 1.2% of all ED
tion (FDA) to ban amphetamine inhalers in 1959.5
presentations, with an associated admission rate of
Amphetamines were widely used as stimulants
39.7% and psychiatry service assessment in 37.2% of
during World War II, and for diverse clinical conditions,
cases.20 An Australasian Triage Scale of 1, 2 or 3 was
including shock, barbiturate overdose, encephalitis,
assigned to 66.7% of patients, indicating a high degree
obesity and postural hypotension. Over 10 billion
tablets containing amphetamines had been legally
manufactured by 1970; the majority were used illicitly.6,7
methamphetamine-related in Australia in 2005 (a rate
Following passage of the Controlled Substance Act in
of 5.9/million persons), a reduction from seventy-five
1970 in the USA, amphetamine abuse rates decreased.8
(6.6/million persons) in 2004.16 However, 26 deaths
However, the 1980s witnessed an explosion in clandes-
were classified as a direct result of methamphetamine
tine production of ‘designer’ amphetamines, the best
toxicity in 2005 compared with 17 in 2004.16 Although
methamphetamine deaths attract regular media atten-
(MDMA) and 3,4-methylenedioxyethamphetamine.9–11
tion, opioid-related deaths are far greater: 374 deaths
A later resurgence in methamphetamine abuse fol-
were reported in 2005 (32.5/million persons).16,21,22
lowed production of a high-purity formulation knownas ‘ice’.12,13 The 1990s rave scene brought widespreaduse of MDMA and methamphetamine in Europe,
Structure and pharmacology
methamphetamine quickly followed. A nasal deconges-
sparse. A recent prospective 3-month study in Western
tant containing amphetamine was marketed in 1932.4
Australia found presentations related directly or casu-
Widespread abuse led the Food and Drug Administra-
ally to amphetamine use comprised 1.2% of all ED
tion (FDA) to ban amphetamine inhalers in 1959.5
presentations, with an associated admission rate of
Amphetamines were widely used as stimulants
39.7% and psychiatry service assessment in 37.2% of
during World War II, and for diverse clinical conditions,
cases.20 An Australasian Triage Scale of 1, 2 or 3 was
including shock, barbiturate overdose, encephalitis,
assigned to 66.7% of patients, indicating a high degree
obesity and postural hypotension. Over 10 billion
tablets containing amphetamines had been legally
manufactured by 1970; the majority were used illicitly.6,7
methamphetamine-related in Australia in 2005 (a rate
Following passage of the Controlled Substance Act in
of 5.9/million persons), a reduction from seventy-five
1970 in the USA, amphetamine abuse rates decreased.8
(6.6/million persons) in 2004.16 However, 26 deaths
However, the 1980s witnessed an explosion in clandes-
were classified as a direct result of methamphetamine
tine production of ‘designer’ amphetamines, the best
toxicity in 2005 compared with 17 in 2004.16 Although
methamphetamine deaths attract regular media atten-
(MDMA) and 3,4-methylenedioxyethamphetamine.9–11
tion, opioid-related deaths are far greater: 374 deaths
A later resurgence in methamphetamine abuse fol-
were reported in 2005 (32.5/million persons).16,21,22
lowed production of a high-purity formulation knownas ‘ice’.12,13 The 1990s rave scene brought widespreaduse of MDMA and methamphetamine in Europe,
Structure and pharmacology