Microsoft word - chapter 3 - the options for achieving weight loss
Prof. Paul O’Brien 2006. All rights reserved.
THE OPTIONS FOR ACHIEVING WEIGHT LOSS
• We must continue to seek preventive measures but they are not
• The general expectations of what should be achieved and what need
to be avoided should be established before looking at the different
• Always begin with the simple and safe and move to the more complex
• Non-surgical options are not yet effective enough for treating obesity
• The surgical options are all effective but vary in risk and change to
We have seen that obesity is a major problem and that weight loss is the most powerful therapy we have in healthcare today. It is now time to look at the ways available for achieving this weight loss. Prevention First, we must mention prevention. This has to be the most important aim to seek. With a problem so common, there is no way that we can ever treat all those who are or will become obese. We must try to prevent the problem arising in the first place. It has to be our first commitment, particularly to our children and adolescents. We talk about primary prevention and secondary prevention. By primary prevention we mean avoiding the obesity ever occurring. By secondary prevention, we mean prevention of the diseases that can arise from the obesity, even if we have not been able to prevent the obesity itself from occurring. Unfortunately, at this stage, we are not very good at primary prevention. We have no successful programs that can be applied across our community and prevent the problem of obesity occurring. We have lots of good ideas, plenty of theories and hypotheses. We have some pilot studies that may show promise. But, to date, we have no proven, predictable way that is acceptable to the community and effective in preventing weight gain.
This is not all that surprising. We live in a culture, reinforced by powerful commercial forces, that promotes eating and physical inactivity. To address this established culture will take a strong political will and a multidisciplinary approach. That has not yet happened. We need to continue to look for good pathways to prevention but they are not yet visible. Not only is the problem of obesity still a problem, it is in fact getting worse. The numbers are increasing. We are losing ground. We are visibly failing to prevent the problem. We have not yet even started to overcome this challenge. We are a little better at secondary prevention. If you develop type 2 diabetes, we can help you control your blood sugar levels and so prevent some of the complications of the disease. If your blood pressure is too high or the fats in the blood are too high, we can give you medicines that help control these problems and thereby reduce the chance of stroke or heart attack. However, this is a compromise. You still have the disease and you are just reducing some of its harmful effects but not taking it away, not curing it. Far better to get rid of the disease altogether. With significant and durable weight loss, type 2 diabetes can go away, blood pressure can return to normal levels and the fats in the blood can return to normal. Most of the obesity related diseases are either cured or markedly improved with weight loss. Naturally this is our preferred approach, so let us look at methods for achieving weight loss and, in doing so I believe it will become clear why the LAP BAND is our preferred option for those who have failed the simpler methods. Weight Loss Options Before looking at each of the options for reducing weight we should establish some general expectations of what we want to achieve and at what cost. We can then look at each option and measure its effect against these expectations. What should be required for all the treatment options: 1. Safety. Beyond all else we must try to avoid hurting people. Everything has possible side effects and complications. These need to be minimal. The method you select to lose weight is a choice you make. It is the balance between the good – the effectiveness - and the bad – the risks and the
costs. The good should always far exceed the bad. 2. Effectiveness. It should be effective in achieving substantial weight loss. If you are overweight, a small weight loss might suffice to solve your problem. If you are obese (BMI > 30) you are more likely to need a substantial weight loss to solve you problems. Depending on your initial weight, a loss of 45 – 260 lb(20 to 120 kg) might be needed, depending on your initial BMI. Certainly 5 -10 kg is not going to be enough. Along with the weight loss, you should check that there is good evidence of health benefits and better quality of life. 3. Durability. There is no particular value in short term weight loss. There may even be harm. Losing weight, even quite substantial amounts of weight, is not so hard. Most of my patients have done it many times before they have come to see me. The real challenge is to keep that weight off for a long time. We therefore should look not only at the amount of weight a treatment can achieve but also we should look for evidence that the effect lasts. 4. Minimal side effects. Being obese is unpleasant but you don’t want to swap one type of unpleasantness for another. If a treatment creates its own problems, such as the oily incontinence from orlistat or the smelly diarrhoea from bilio pancreatic diversion, it is not much fun. Check beforehand as to what are the possible side effects of each treatment. 5. Controllable/adjustable. This is true for lifestyle methods where you can control the amount you eat or the exercise you do. There is some flexibility with doses of drugs used for weight loss. For all surgical procedures, except the LAP BAND, you do not have this ability. In the future there will be more options which are adjustable but not at this stage. Once the surgeon has left the operating room after a gastric bypass, there is nothing that can be done to vary the restriction created. If it’s too tight, bad luck. If it’s too loose, too bad. If it is just right, it may slowly alter over time and you or you doctor cannot take it back to where it was without difficult surgery. Having control is very important. Good weight loss programs center on a partnership between you and your doctor or other health professional. You
both need to be able to exercise some control of the treatment to optimize the effect. Without doubt, the adjustability of the LAP BAND is its greatest single asset. It allows that control over your level of satiety to be exercised. 6. Reversibility We can easily stop a diet or a course of drug treatment. We can remove an intragastric balloon. For surgical procedures, the LAP BAND is the only one that is easily reversible. Reversibility is almost as important as the adjustability for two reasons. First, we all are sceptical. We worry that something promised may not turn out just so. You do not want to be trapped into something that may not turn out to be what you expected. With the LAP BAND, you are not trapped in a permanent state. It can be removed easily and everything goes back to normal. Not so with other surgical procedures. They are there for life. The second reason to look for reversibility is that we can only look into the future so far. At the moment there is nothing better than the LAP BAND in view. However, in 20 years time, maybe even 15 years, there could be a dramatically better treatment discovered. You don’t want to be locked into something that is well passed its use-by date. You want to be able to choose the best current option. 7. Low reoperation/ revision rate Naturally you would like to have one procedure and that will be all. Unfortunately this does not always happen. Something may change or leak or block or break may lead to the need for additional procedures. There is a maintenance requirement for each of the surgical procedures. You need to be aware how likely it is and how complex and risky is the revision. 8. Minimally invasive If you are going to have surgery, you will want to have as little trauma and changes to your gut as possible. Look for the procedure that interferes with the tissues the least. Ask about what is done for each procedure. Are organs or parts of them removed? Are segments of the gut closed off or redirected? Is there joining of one part of the gut to another? Remember leaks from these joins are the major cause of deaths in the surgical patients.
We are now going to review the options available. It is important to be committed to solve your problem of obesity but to look for the simple and safe options which are effective before moving to the more complex and risky. The list of desirable features above should help you find the right option. We will return to this list after we have looked at the different treatment options to see where each is strong and weak. Keep this list of criteria in mind as we take each of the treatment options and see what it has to offer. The chart of this list and their relation to the different treatment options is at the end of chapter 4.
1. Lifestyle:
Less food and plenty of activity. This solution is simple to prescribe yet very difficult to achieve sustainable outcomes. Across the world and across generations a healthy lifestyle through good eating and exercise practices has been constantly promoted; yet the problem of obesity is not just continuing but increasing. A recent comprehensive review of all the high quality scientific studies of the options for weight control found that there is no evidence of a durable effect from any current lifestyle intervention methods. Lifestyle change has also been used as an approach to preventing obesity. As we are failing to prevent it, we must have less hope of curing it once it is established. The results are therefore not surprising. Almost everyone can lose some weight. The challenge is to lose enough weight to make a difference and, more importantly, to keep it off. Weight loss for one or two years is not much help to your health. You need to lose weight permanently. Very few will lose weight by lifestyle change alone and be able to keep that weight off for even 5 years. The commercial weight loss centres have made fortunes by promising excellent weight loss through various twists on the “lifestyle” methods and their constant advertisements always show the classic “before and after” pictures. Invariably, the “after” picture is after months. They do not show the “after” pictures at 5 years. One particular form of dietary therapy which can have a powerful effect in the short term is the Very Low Calorie Diet (VLCD). The best known form of
VLCD is called Optifast. This involves taking three sachets of a specially formulated powder each day and almost no other food. Each sachet is made up into a liquid meal with water. You are allowed a small amount of vegetable at night as the only additional intake. If you follow the rules completely you will be receiving between 500 and 600 calories per day and you may lose 15 – 30 kg over a 3 month period. It is not recommended that you continue beyond 3 months and it is uncommon to succeed so well with a second course later on. The good weight loss should be seen as being short term. VLCD provides perhaps our best method for achieving a significant weight loss quickly without resorting to weight loss surgery. There can be reasons why this is a good idea. A common one is as a preparation for a surgical procedure such as a knee or hip operation. We frequently use VLCD in some patients as a preparation for the LAP BAND procedure. As it is not continued permanently, you cannot be expected to achieve a medium or long term weight loss with VLCD.
2. Drug Therapy:
We do not yet have drugs that are truly effective for treating obesity. There are two drugs currently available for long term use for achieving and maintaining weight loss – orlistat ( sold as Xenical) and sibutramine (sold as Meridia or Reductil). Both are able to contribute to the treatment of overweight but neither has proven to be sufficiently powerful to be reliable for treating obesity. Long term efficacy is poor and long term safety is unknown. If all the clinical trials of these drugs are combined we find that the average weight loss after one year of orlistat is about 7 lb (3 kg) and for sibutramine 10 lb (4.5 kg). For those with obesity, who must lose more than 50 lb (20 kg) or more, these results are just not good enough. New drugs appear on the horizon frequently and some of these do get into clinical practice. The latest to attract serious interest is rimonabant. In a recent clinical trial this drug produced an average weight loss of 15 lb (6.6 kg) at 12 months. Still not enough to cure obsity but of real potential for the overweight. It will probably appear on the market in 2007 and will give the community a high expectation for a while.
Most of my patients have tried some of the drug therapies before considering the LAP BAND. Anything may be worth a try if the problems of obesity can be overcome. However it is best not to expect too much. They are not that good. Further they are usually expensive, they may have unpleasant or even serious side effects and the thought of taking one of these drugs every day for years and years in order to get a few pounds of weight off is just not acceptable to most people, especially when so little weight loss is achieved. We definitely need better drugs for obesity. No doubt they will come. We may one day find a pill that truly takes away your appetite or increases the wasting of energy. There will be some gene therapy that makes you thin forever. The pharmaceutical companies are working very hard to find such drugs or treatments. Given that there is nothing which is dramatically good on the horizon and that it would take 5 – 10 years from development to market, we probably should do not anticipate success in the next 15 years and possibly not in the next 20 years. If however, in the meantime, you have gone ahead with a LAP BAND, you can at least be comforted that, if some magical new therapy does arise which works superbly and has minimal side effects, you can have the band removed as a day procedure, the stomach can return to normal and you can start on the new “magical” treatment. The LAP BAND is fully reversible. Not so if you have had a gastric bypass. This is very difficult procedure to reverse as the stomach has been divided completely and the intestines have been dramatically rearranged. For most of these patients, there can be no going back.
3. Endoscopic Procedures:
Endoscopic procedures are those where a gastroscope, a long flexible tube of light fibres, optical fibres and other channels, is passed through the mouth, down the oesophagus and into the stomach. These procedures have not yet established a role in the treatment of obesity but there is plenty of effort seeking an effective method.
Intra-gastric balloons are the only endoscopic method which is currently in clinical practice around the world. With this method, an empty balloon is passed through the mouth into the stomach. It is then filled with about half a litre of saline and thereby creates a large mass in the stomach. The idea is that you feel full and do not eat so much. After 6 months, the balloon must be removed as it may rupture and cause a blockage further down the gut. The intra-gastric balloons had a period of enthusiastic usage in the 1980s until carefully performed clinical trials showed them to be ineffective. A new version of the intra-gastric balloon, the BioEnterics Intragastric Balloon, commonly known as the BIB, has been developed with the proposal that it overcomes all the weaknesses of the earlier balloons. It is being used extensively in Europe, Mexico and South America. It is approved for clinical use in Australia but not yet in the USA. In the clinical reports available the BIB appears to work but has yet to demonstrate effectiveness in high quality clinical trials. It can be left in place for only 6 months, during which time there may be a weight loss of 35 lb (15 kg) or more. The lost weight is likely to return after its removal. Nevertheless, it does appear to make a difference, it does not involve an operation and it is reversible. There is a high level of research activity seeking other ways of achieving weight loss by methods involving endoscopic techniques. These include ways of suturing or stapling the stomach through the endoscope to simulate what is done in some surgical procedures. It is likely that some of these will appears soon and they will be publicized as the ultimate solution. It is even more likely that their benefit will in fact be modest and short term. We just have to wait and see what happens. 4. Weight Loss (Bariatric) Surgery: The surgical treatment of obesity is called bariatric surgery after the Greek words, baros = weight and iatrikos = the art of healing. This is the most rapidly growing area of surgical practice in the Western world today. This reflects the ability of bariatric surgical procedures to provide a
solution to an otherwise insoluble problem and the evolution of safer, less invasive and more conservative forms of procedures. Today there are three procedures in use: gastric bypass, biliopancreatic diversion and laparoscopic adjustable gastric banding, as shown in these figures.
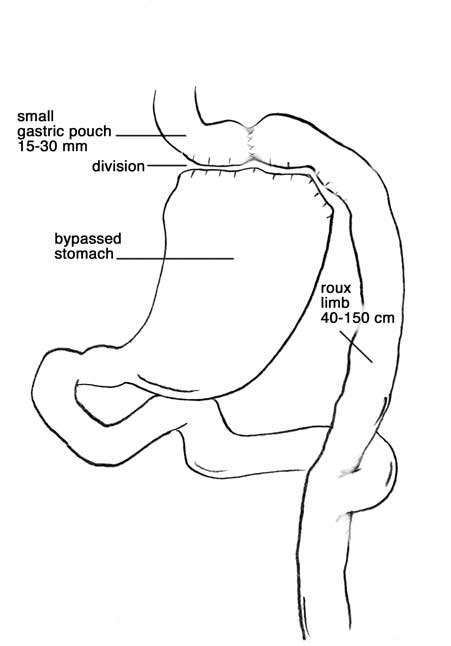
1. Gastric Bypass This operation was introduced more than 35 years ago and is still a good procedure. However it does require major manipulation of the gut. It is most commonly used in the USA and about half of the operations are performed by the traditional open surgical approach with a long incision in the abdomen and half are performed laparoscopically (key hole surgery). It is a form of gastric or stomach stapling as a stapling device is used to cut and separate a small piece of the top of the stomach from the rest of the stomach. The top part will be the new stomach and the rest will be closed off and not accessible any more. The upper part of the small intestine is then divided completely, again with the stapling device. One of the divided ends is then attached to the new stomach to allow the food enter the rest of the gut. The other end is joined to the small intestine further downstream so that the digestive juices from the liver, gall bladder, duodenum and pancreas can get back into the digestive pathway. The diagram shows the end result of these multiple changes. 2. Biliopancreatic Diversion This procedure aims to reduce the size of the stomach to resttrict intake and also prevent absorption of the food by diverting it from the digestive enzymes of the gut. Although it can be done laparoscopically, it is generally performed through an abdominal incision to reduce the risks. About half to three quarters of the stomach is removed completely. The small intestine is then divided and reconnected in such a way that the food goes one way (the
alimentary limb) and the digestive enzymes go another way ( the biliopancreatic limb – BPL). Most of the enzymes are reabsorbed before they do anything. The rest meet the food in the last 2 feet (50 cm) of the small intestine to permit some absorption.
3. Lap Band Lap Band placement is far more gentle and safe than the preceding operations. It is essentially always done laparoscopically (key hole surgery) and it involves very little handling or dissection of the tissues. Nothing is cut
or stapled or removed or redirected. There is a brief video cartoon of the operation on the DVD to show what happens. The LAP BAND is placed across the very top of the stomach. There is almost no stomach above the band. With minimal dissection a pathway is made across the back of the top of the stomach, the band is placed along that pathway, closed and fixed into that position by suturing some of the stomach wall across the front of the band. The tubing is then connected to an access port which is placed under the skin of the abdominal wall.
Which procedure is the most common? There is significant variation in the preferred procedure between countries, often reflecting local regulatory and insurance factors. In the USA, gastric bypass is still the most common option. The LAP BAND did not become available in the USA until 2001 and many insurance groups still are trying to avoid offering this option to their participants. However
the number of LAP BANDs placed is increasing rapidly and is expected to become much more common than the bypass for the reasons I give below. In Australia, the LAP BAND is the procedure of choice for more than 90% of people, with gastric bypass making up most of the rest. The biliopancreatic diversion is an uncommon procedure everywhere because of the risks and the concerns about the effect that the long term lack of key nutrients will have on the body. In many countries it is not used at all. THE HISTORY OF THE BARIATRIC PROCEDURES
The surgical treatment of obesity has evolved over a period of more than 50
years. It can be divided into three periods
THE FIRST PERIOD 1950S – 1970S - SMALL BOWEL BYPASS
The first era began in the 1950s and was the era of the small bowel bypass.
There are various ways in which this operation was performed. Each method
however shared the common principal of bypassing the normal absorptive
capacity of the gut. You could eat quite a lot but you wouldn’t absorb it into
the body. Instead you would have diarrhoea. They were generally effective
in achieving weight loss but they had a number of serious side effects which
A new form of bypass has been introduced in the 1970s It is called bilio-
pancreatic diversion, commonly abbreviated as BPD. It is a complex
procedure involving removal of much of the stomach and bypassing much of
the gut. There is a variation of the BPD, known as the duodenal switch. It
differs in only a minor way by changing the way most of the stomach is
removed to retain the lower part of the stomach. It is not clear that there
is any important difference between the two procedures. The BPD generally
achieves good weight loss but at the cost of significant symptoms and a
serious risk of malnutrition. It can be done as an open operation or,
sometimes, laparoscopically. It has the highest likelihood of death
associated with the surgery of all the bariatric procedures
THE SECOND PERIOD 1960S - PRESENT ~ STOMACH STAPLING – GASTRIC
The second era was the era of the stomach stapling and this became popular
from the 1970s. Again there were a number of different ways of
performing the operation but they also achieved their effect through two
common features. Firstly, they created a small upper stomach so that you
could only eat a small amount of food at any one time before you felt
comfortably full. Secondly, they each delayed the emptying of the food
from that small upper stomach into the rest of the gut in some way so that
the feeling of fullness stayed with you after the meal and you were not
inclined to eat between meals. The most common form of stomach stapling
At their best, gastric bypass and the other stomach stapling procedures
were very good. They would enable a good weight loss without too many side
effects. However, they were not at their best often enough. The real
dilemma with the stomach stapling was to create a new stomach which was
exactly right on the day of operation and remained exactly right for the
rest of the patient’s life. This challenge is obviously too difficult. The body
will always be changing, particularly stretching, in response to pressure.
Sometimes the settings were too tight initially and there would be severe
vomiting. At other times the settings were too loose and there was
insufficient weight loss. Most commonly, the settings were about right at
the time of operation, but changed over subsequent months and years so
that, with stretching or with breakdown of the staple line, there would be a
return towards a normal stomach and the weight reducing effect would be
lost. The best weight loss after gastric bypass is in the first year. Generally,
if you have not lost enough weight by then, you are not going to lose any
more. The weight starts to come back on again after the second or third
year. Because there is no ability to adjust the settings after the operation,
the weight regain is not able to be controlled. It is very difficult for us to
be sure about how durable the weight loss is after gastric bypass because
more than half the people who have the operation are lost to follow up by 5
years and so we cannot measure their weight. For those that are still being
seen, it is most commonly reported that they have lost between 50 and 60%
of their excess weight. If we assume the ones who are missing have done
less well, the usual reason why people stop coming to follow up, the weight
loss is probably well under 50% of excess weight at 10 years. This is not as
good as I have been able to achieve with the LAP BAND.
Stomach stapling is a big operation with real risk of major complications and
approximately 1% of people die from these complications. It causes major
change in the gut and is essentially irreversible. The most common form of
stomach stapling now used is the Roux-en-Y gastric bypass. This can be
done as an open operation or laparoscopically. It is a complex procedure
which involves dividing the very top of the stomach completely so that only a
very small pouch is left. This is connected to some small bowel in a manner
which allows limited bypass of the small bowel. There is no opportunity for
adjustment after the operation. Another form of gastric stapling that is
being more commonly used at some centres is the sleeve gastrectomy in
which most of the stomach is removed and discarded and a thin tube is left,
with the hope that it will not expand in the years to come. Our previous
experience strongly suggests that hope will not be realised.
Although stomach stapling has been an acceptable option for some people, it
has proved to be unacceptable to the vast majority of those in the
community who are obese, either because of its risks and invasiveness or
because of the difficulties in retaining the correct settings over a long
period. It can be estimated that only one of every two hundred people who
have severe obesity would agree to a bypass or other form of stomach
stapling. The other 199 either have accepted their problem of obesity or are
looking for a more acceptable alternative.
The third era is the result of efforts to find an acceptable alternative to
THE THIRD PERIOD 1990S - NOW ~ THE LAP BAND
The LAP BAND procedure has been developed to retain the good things that
we have learned from stomach stapling, but to overcome the problems which
made stomach stapling generally unacceptable. The key features of LAP
BAND that have led to its acceptance are its safety, minimal invasiveness,
adjustability, reversibility and overall effectiveness. In my own practice, I
used gastric bypass for many years prior to the LAP BAND becoming
available, but since 1993 I have no longer offered this option for the first
treatment of obesity as it is clearly more dangerous, with greater likelihood
of deaths or complications, it is not adjustable or reversible and it is no
more effective in the medium term than the LAP BAND.
In chapter 4, I will look at all the good features of the LAP BAND and
discuss what are reasonable expectations with regard to weight loss. I will
also look at its problems and unfavourable features. And then I will describe
the type of people who would be best treated with the LAP BAND. From this
you will be able to see if this may be a suitable procedure for you.
_______________________________________________________________ _______________________________________________________________ DP World Chair for Entrepreneurship and Innovation, Said Business School, University of Oxford, August 2010 to the present. The formal inaugural address has been viewed by nearly 2,000 people: http://www.youtube.com/watch?v=x_SHdzf4LWI&feature=youtu.be Duties focus
 2. Biliopancreatic Diversion
2. Biliopancreatic Diversion 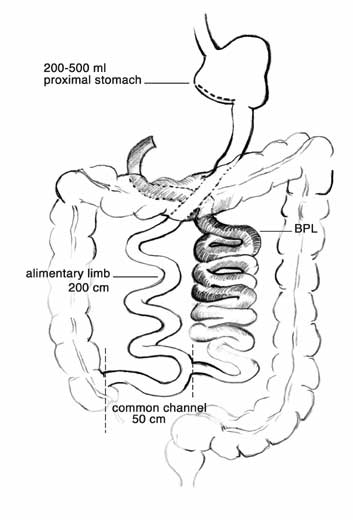 alimentary limb) and the digestive enzymes go another way ( the biliopancreatic limb – BPL). Most of the enzymes are reabsorbed before they do anything. The rest meet the food in the last 2 feet (50 cm) of the small intestine to permit some absorption.
3. Lap Band
alimentary limb) and the digestive enzymes go another way ( the biliopancreatic limb – BPL). Most of the enzymes are reabsorbed before they do anything. The rest meet the food in the last 2 feet (50 cm) of the small intestine to permit some absorption.
3. Lap Band 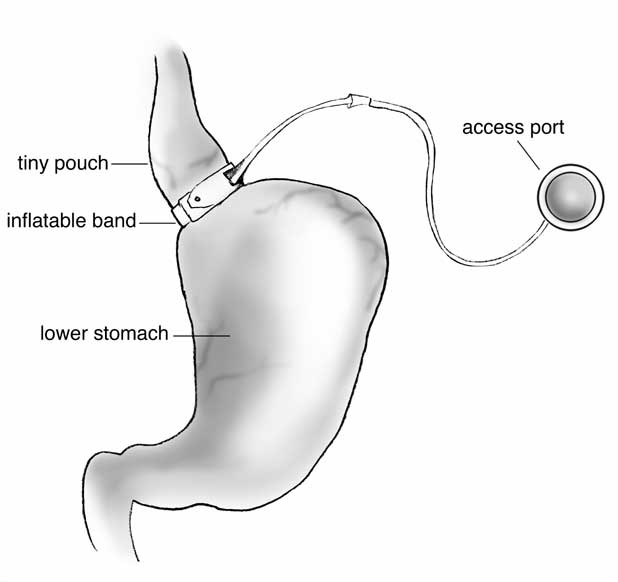 or stapled or removed or redirected. There is a brief video cartoon of the operation on the DVD to show what happens. The LAP BAND is placed across the very top of the stomach. There is almost no stomach above the band. With minimal dissection a pathway is made across the back of the top of the stomach, the band is placed along that pathway, closed and fixed into that position by suturing some of the stomach wall across the front of the band. The tubing is then connected to an access port which is placed under the skin of the abdominal wall.
or stapled or removed or redirected. There is a brief video cartoon of the operation on the DVD to show what happens. The LAP BAND is placed across the very top of the stomach. There is almost no stomach above the band. With minimal dissection a pathway is made across the back of the top of the stomach, the band is placed along that pathway, closed and fixed into that position by suturing some of the stomach wall across the front of the band. The tubing is then connected to an access port which is placed under the skin of the abdominal wall.