Effect of Inspiratory Muscle Training in Patients With Multiple Sclerosis Brita Klefbeck, PT, PhD, Jallal Hamrah Nedjad, PT, MSc
ABSTRACT. Klefbeck B, Hamrah Nedjad J. Effect of
confirmed through laboratory tests. The disease presents either
inspiratory muscle training in patients with multiple sclerosis.
with an exacerbating-remitting pattern, which is characterized
Arch Phys Med Rehabil 2003;84:994-9.
by periods of impairment followed by full or partial remissionof symptoms, or with a chronic, progressive pattern. This latter
Objective: To evaluate whether inspiratory muscle training
(IMT) improves inspiratory muscle strength, respiratory capac-
pattern can be subdivided into progressive from the onset and
ity, fatigue, and subjective perception of physical endurance in
secondarily progressive, in which there is a steady worsening
patients with advanced multiple sclerosis (MS).
of symptoms over time, with ataxia, visual loss, weakness,
Design: Randomized controlled trial.
spasticity, fatigue, bladder dysfunction, and so on.4-6
Setting: Outpatient clinic in Sweden.
When a neuromuscular disorder is progressive, symptomatic
Participants: Fifteen severely disabled patients with MS,
respiratory muscle weakness is inevitable. The MS plaques are
randomized to a training or control group.
often found in the brainstem and upper cervical spinal cord.7
Intervention: Seven patients trained with a Threshold in-
Pathophysiology and clinical features of MS vary in each
spiratory muscle trainer, twice every other day, with 3 sets of
patient. As a result of the demyelinated plaques, abnormalities
10 loaded inspirations (40%– 60% of patients’ maximal in-
of speech and weakness of muscle groups responsible for
spiratory pressure [PImax]) over a 10-week period.
speech and/or swallowing are common. In addition, patients
Main Outcome Measures: Spirometry, PImax, maximal
with bulbar lesions may have both laryngeal and pharyngeal
expiratory pressure (PEmax), clinical assessments, and ques-
dysfunction, causing symptoms such as dysphonia, dysphagia,
tionnaires on the patients’ fatigue severity and physical endur-
and aspiration.7 Severe respiratory muscle weakness can be
expected in patients with MS who are severely paraplegic, and
Results: After training, the PImax (PϽ.008) and PEmax
the weakness increases as the upper extremities become in-
(PϽ.02) increased in the training group. The improvement in
creasingly involved.8-10 Respiratory complications are a major
PImax after 10 weeks of training was higher than the improve-
cause of morbidity and mortality in patients with MS.11 Aspi-
ment in the control group (PϽ.01) and was maintained 1 month
ration and pneumonia secondary to bulbar weakness and im-
after the training period ended. The training affected neither
mobility have long been recognized as common events in
respiratory function nor the patients’ symptoms. Conclusions: IMT had a beneficial effect on inspiratory
muscle strength in patients with MS and is recommended as a
Inspiratory muscle weakness often occurs in neuromuscular
complement to ordinary physical training.
disorders. It is sometimes associated with a chronic increase in
Key Words:
Multiple sclerosis; Physical therapy tech-
arterial carbon dioxide tension.13 Immobility reduces lung vol-
niques; Rehabilitation; Respiration.
ume and can lead to postural hypotension, constipation, urine
2003 by the American Congress of Rehabilitation Medi-
retention, osteoporosis, depression, and deconditioning.13 Pa-
cine and the American Academy of Physical Medicine and
tients with MS show a poor exercise tolerance, with fatigue and
dyspnea on exertion, which limits their ability to performactivities of daily living14 (ADLs). MULTIPLE SCLEROSIS (MS) is a chronic inflammatory
Fatigue is a particular problem in patients with MS. Its
disease of the central nervous system (CNS); this disease
mechanism and precise etiology remain unresolved,3 because
affects mostly young and middle-aged adults and is associated
fatigue does not correlate with the degree of neurologic im-
with selective destruction of the myelin sheaths. This leads to
pairment or disability in these patients.15,16
the formation of large demyelinated plaques dispersed through-
Efforts have been made to examine the effect of training of
out the CNS, with a predilection for the optic nerves, brain-
respiratory muscle strength and endurance by using different
stem, spinal cord, and periventricular white matter. In partic-
resistive breathing devices. In several studies, a Threshold
ular, in cases with progressive disease, severe neurologic
inspiratory muscle training (IMT) device has been used in
deficit axonal destruction and loss can be profound.1-3 MS is
patients with chronic obstructive pulmonary disease (COPD) orasthma to improve inspiratory muscle strength and endur-ance.17-23 The usefulness of the IMT device in patients withneurologic dysfunction has been shown by several research-ers24,25 who have explored the influence of this training method
From the Neurotec Department, Division of Physiotherapy, Karolinska Institutet
on inspiratory muscle strength and endurance. Few studies
(Klefbeck); and Habilitation Center for Adults (Hamrah Nedjad), Stockholm, Swe-den.
have, however, focused on increasing respiratory muscle func-
Supported by the Swedish Association of the Neurologically Disabled, Norrbacka-
tion in patients with MS to improve respiratory function and/or
Eugeniastiflelsen, the Foundation of the Swedish Committee for Rehabilitation, and
Handicap & Habilitation, Stockholm County Council.
This study evaluated whether 10 weeks of supervised train-
No commercial party having a direct financial interest in the results of the research
supporting this article has or will confer a benefit upon the author(s) or upon any
ing of inspiratory muscles in patients with MS would affect
organization with which the author(s) is/are associated.
their respiratory muscle strength, respiratory capacity, and gen-
Reprint requests to Jallal Hamrah Nedjad, Habilitation Center for Adults,
eral well-being, as measured by indices such as fatigue and
Kemistva¨gen 8, SE-183 79 Ta¨by, Sweden, e-mail: jal_hamrah@hotmail.com.
subjective perception of physical endurance, without causing
0003-9993/03/8407-7386$30.00/0doi:10.1016/S0003-9993(03)00133-3
any adverse effects. Furthermore, our aim was to establish
Arch Phys Med Rehabil Vol 84, July 2003 INSPIRATORY MUSCLE TRAINING IN MS, Klefbeck
whether any effects of training would be evident 1 month after
Table 1: Patient Characteristics and Pretraining Respiratory Function Measures of the Training Group (n؍7) and Control Group (n؍8) Participants
The patients in this study were recruited from 3 rehabilita-
tion outpatient clinics in Stockholm, Sweden. All patients met
the criteria of Poser et al4 for the diagnosis of MS, presented
with a progressive pattern of MS, and scored between 6.5 and
9.5 on the Expanded Disability Status Scale26 (EDSS). This
evaluation scale was used to describe symptoms and to quan-
tify neurologic deficits, based on a neurologic examination.
Patients who did not meet the diagnostic criteria, according to
EDSS, scored 0.0 to 6.0, were excluded from the study, as were
patients with chronic obstructive airways, asthma, emphysema,and cystic fibrosis. Also excluded were patients with heart
NOTE. No significant differences were observed between the
insufficiency, patients with chronic pain, and patients with
another diagnosis or other disorders. Patients who had diffi-
Abbreviations: FEV , forced expiratory volume in 1 second; FEV%,
forced expiratory volume in percent of FVC; FVC, forced vital capac-
culty in understanding instructions and patients who were
ity; PEF, peak expiratory flow; VC, vital capacity.
already participating in other projects were likewise excluded.
Altogether, 22 patients with MS expressed interest in the
study. The first contact between the examiner (JHN) and thepotential participants was by telephone, for the purpose of
Evaluation
assessing their physical and mental status, as determined by the
All tests were performed at the beginning and at the end of
EDSS, and to inquire about what medications they were tak-
a 10-week period and again 1 month after the training ended.
ing—with special emphasis on their history of respiratory
Respiratory muscle strength was assessed by measuring max-
illness—and about their use of tobacco. We also wanted to
imal inspiratory pressure (PImax) and maximal expiratory pres-
establish whether the patients had medical problems or histo-
sure (PEmax), according to the method of Black and Hyatt,27 by
ries that were probably not related to MS. Two patients had had
using a handheld mouth pressure meter (Micro MPM).a The
other diagnoses, such as stroke; 1 patient had rheumatism and
Micro MPM consists of a pressure transducer and electronic
chronic airway obstruction; 1 patient had another neurologic
calculator with a liquid crystal display screen. The patient,
disorder and a probable MS diagnosis; and 2 patients said they
while comfortably seated and wearing a nose clip, performed
were too busy to participate. These 6 patients were excluded
maximal inspiratory and expiratory efforts, starting from near
from the study. In all, 16 patients met the inclusion criteria and
residual volume and near total lung capacity, into an obstructed
were sent a letter assigning them an individual examination
flanged mouthpiece with a small air leak to prevent generation
date at the clinic. The patients were randomized to a training
of high buccal pressures. For measurements to be considered
(nϭ8) or a control (nϭ8) group. One patient in the training
technically acceptable, no air leaks could be detected around
group dropped out after 4 weeks, having failed to cooperate,
the mouthpiece, and the patient had to maintain the pressure for
and was excluded from data analysis.
least 1 second. All measurements were taken at approximately
Data were analyzed for 15 patients (9 women, 6 men)
the same time of day to minimize the effect of time of day on
between the ages of 37 and 61 years (mean age, 49y). All gave
patients’ level of subjective fatigue.28
their informed consent to participate in the study, which was
Achievement of PImax and PEmax in clinical laboratory tests
approved by the local ethics committee. The training group was
requires motivation, practice, and effort. Numerous research-
composed of 6 women and 1 man. No patient had acute
ers28,29 have shown the effect of learning with repeated mea-
respiratory or cardiac failure at the time of the study, and none
sures of PImax and PEmax in both able-bodied people and
experienced an exacerbation or a relapse during the study. All
patients with airway obstructions. Therefore, taking into ac-
patients were wheelchair bound, and 3 patients were essentially
count the learning of the technique of PImax and PEmax
bedridden but were able to sit up for a few hours every day.
measurement, the patients were verbally encouraged to achieve
Time since MS was diagnosed ranged from 3 to 35 years
maximal strength and coordination so that baseline values
(mean Ϯ standard deviation [SD], 17Ϯ7.8y). Patients had
could be obtained. The maneuver was repeated at least 3 times
disabilities ranging from ataxia to quadriplegia, and the median
or until 2 reproducible efforts were obtained (ie, within 5% of
EDSS score was 8 (range, 6.5–9.0). Most patients showed
each other). An interval of about 1 minute was allowed be-
laryngeal and pharyngeal dysfunction, as indicated by the
tween the measurements to avoid short-term fatigue of the
symptoms of dysphonia, dysphagia, and aspiration. They re-
respiratory muscles. The reliability of maximal respiratory
quired individual attention from 0 to 24 hours per day. Four
pressure has been described by several authors.30,31 The higher
patients reported being current or former smokers. EDSS score,
of 2 reproducible values was considered in the data analysis.
age, medications, and smoking history did not differ for pa-
PImax and PEmax were expressed as absolute values in cmH O
tients in the training and the control groups.
and as percentages of the predicted normal value, according to
The patients’ characteristics are presented in table 1. Most
had undergone therapy with interferon-beta and baclofen and
Respiratory function through dynamic spirometry was as-
had also received physical therapy (PT)—which included bal-
sessed, with the subjects sitting, by use of a handheld spirom-
ance, coordination, gait, transfer, and strength training, as well
eter (Micro Loop).a Pollard et al33 have shown that the Micro
as range of motion therapy—1 to 2 times a week. The duration
Loop is reliable. The patients wore a nose clip during the test.
and intensity of PT was the same for all patients.
The method has been previously described.34 The vital capacity
Arch Phys Med Rehabil Vol 84, July 2003 INSPIRATORY MUSCLE TRAINING IN MS, Klefbeck
(VC), forced vital capacity (FVC), forced expiratory volume in
The patients were visited in their homes every other week by
1 second (FEV ), forced expiratory volume in percent (FEV%),
the authors to exchange logbooks and to help them with log-
and peak expiratory flow (PEF) were measured. The values
book entries, as needed. During these visits, changes were
were expressed as both an absolute value in liters and a per-
made in the inspiratory threshold training load, as indicated by
centage of the predicted normal value, according to the Euro-
the PImax and RPE scale, and any changes in the patients’
pean Coal Community standards.35 No patient had previous
clinical status were noted. Furthermore, patient compliance
experience with spirometry. The patients were verbally encour-
with the procedures was assessed, and, at each visit, they
aged to achieve maximal effort, and the best of 3 trials was
performed a complete training session. Patients were assured
accepted. The Micro MPM and Micro Loop were calibrated to
that personal and telephone contact would be maintained with
meet the requirements of the American Thoracic Society36
them weekly during the training program to answer their ques-
tions and to provide them with feedback. Patients in the control
Patients’ subjective perceptions of fatigue were examined
group were contacted repeatedly by telephone, but they were
through the Fatigue Severity Scale (FSS), as described by
given no specific feedback about the study. Deep-breathing
Krupp et al.37 The FSS score is established through answers to
exercises were, however, a routine part of their ordinary phys-
a questionnaire containing a 9-point test about both mental and
physical fatigue. In this study, the FSS was used to detectclinical change in fatigue over time. Each item is scored from
Statistics
1 to 7, with 1 indicating strong disagreement and 7 indicating
Descriptive nonparametric statistics were used to calculate
strong agreement with each statement in the questionnaire. The
median and range and to characterize variables. Mean and SD
mean score is obtained so that the test result range is 1 to 7.
were used for variables with normal distribution. The Wil-
Predicted scores for healthy adults are expressed for this ques-
coxon rank-sum test was used to compare the groups, and the
tionnaire. A high total score indicates severe fatigue.
Wilcoxon signed-rank test was used to characterize changes
Patients were asked to estimate their degree of perceived
that took place after training in each group. Finally, the Spear-
physical exertion on the Borg 6 –20 Ratings of Perceived
man rank-order correlation coefficient was used to highlight the
Exertion (RPE) scale38 after they had bathed and dressed in the
relation between the FSS and the EDSS. Statistical significance
morning. The perceived physical exertion on the RPE scale
was defined as P less than .05.
was ranked from 6 (not strenuous at all) to 20 (extremelystrenuous at the physical task or exercise level). Inspiratory Muscle Training Pretraining
The specificity and overload principles of exercise training
All 15 patients passed the initial series of tests. The baseline
were used to train the respiratory muscles, as described in the
respiratory muscle function did not differ between the groups,
study by Smeltzer et al.39 The specific target of training in our
and the PImax and PEmax values were significantly lower than
study was to strengthen the inspiratory muscles. The overload
predicted normal values. The mean PEmax value was
principle was implemented through high-intensity exercise of
54Ϯ31cmH O (48%Ϯ17% of the predicted value), and the
short duration twice every other day. A Threshold IMT deviceb
mean PImax value was 53Ϯ30cmH O (59%Ϯ25% of the pre-
was used for IMT. The valve on this device blocks airflow until
dicted value); they are presented with median values and range
the patient generates sufficient inspiratory pressure to over-
come the resistance provided by the spring-load valve. The
The baseline respiratory function values did not differ be-
threshold pressure is independent of airflow or breathing fre-
tween the groups, and the observed values in all respiratory
quency. The pressure settings are adjustable in Ϫ2cmH O
parameters were markedly reduced compared with predicted
increments (range, Ϫ7 to Ϫ41cmH O). The device has been
Training Group Table 2: Pre- and Posttraining Values of Maximal Inspiratory and Expiratory Pressures, FSS Scores, and Borg RPE Scale Scores in
Before starting the training, the patients had a 1-week run-in
15 Patients With MS
period to become familiar with the Threshold IMT device.
Each patient was asked to record home practice sessions in a
logbook and to do the training at home for 10 minutes twiceevery other day, with at least 4 hours between each training
session. Over a 10-week period, this totaled 70 training ses-
sions. A complete training session consisted of 3 sets of 10
loaded inspirations, with a 1-minute rest between sets. The
initial training load was submaximal, was based on 40% to
session, was not to be perceived as more than 17 (very hard) on
the Borg 6 –20 RPE scale. Patients were encouraged to inter-
rupt the training if they reached 17 before the end of the
session. The perceived sense of 17 on the RPE scale was
defined as very strenuous. Expiration was unloaded, and each
patient was free to choose his/her respiratory rate. The patients
were also asked to estimate degrees of perceived physical
exertion on the RPE scale after bathing or dressing and to
record the degrees in the logbook. Patients were asked to make
NOTE. Borg RPE scale score was measured after washing and dress-
a note of all their activities during the week that were not
Arch Phys Med Rehabil Vol 84, July 2003 INSPIRATORY MUSCLE TRAINING IN MS, Klefbeck
(40%– 60% of PImax) over a 10-week period, improved thePImax and PEmax (PϽ.008, PϽ.02, respectively) in the train-ing group. The improvement in PImax was higher than that inthe control group (PϽ.01), and the benefits of the 10 weeks ofsupervised training were still seen 1 month later. Inspiratorymuscle training did not affect respiratory parameters, such asFEV , FVC, VC, PEF, and FEV%, nor were its benefits re-
flected in the FSS questionnaires or the patients’ subjectiveperception of physical endurance after bathing and dressing inthe morning. No correlation could be found between EDSS andFSS scores. Respiratory Muscle Function
Baseline PEmax (48%Ϯ17%) was more affected than was
baseline PImax (59%Ϯ25%), and both these values were sig-nificantly lower than predicted normal values. This finding haspreviously been described by Smeltzer et al.8 Paralysis inadvanced MS is disposed toward ascending slowly from the
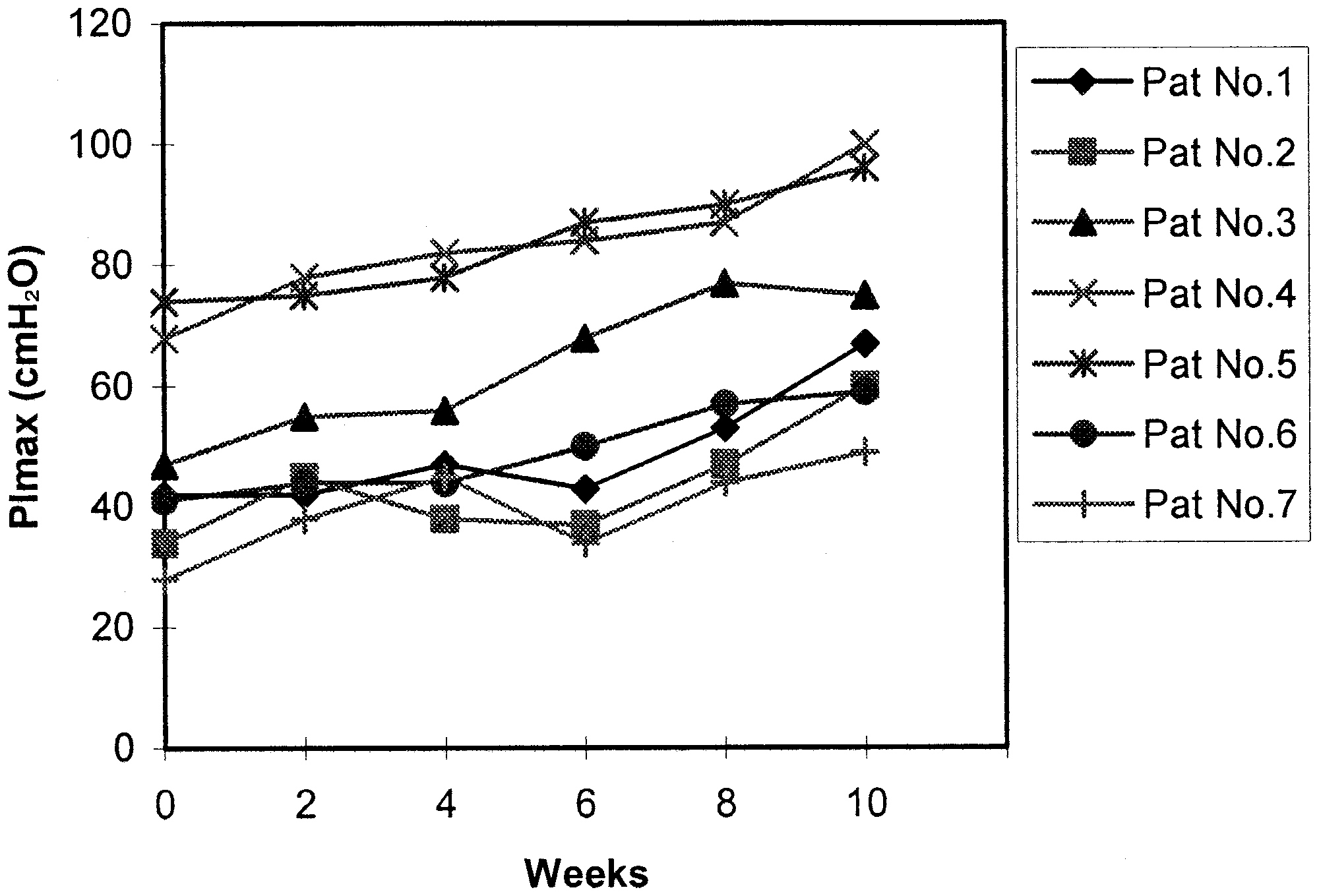
Fig 1. PImax (cmH O), measured by mouth pressure meter, from baseline to 10 weeks of IMT in 7 patients with MS. Abbreviations:
lower extremities to the upper extremities.8 As a result, the
Pat, patients.
muscles primarily affected are the expiratory muscles, fol-lowed by the abdominal and intercostal muscles, and, finally,the inspiratory muscles, including accessory inspiratory mus-
normal values. The mean FVC was 2.7Ϯ1.5L, the mean FEV1
cles in patients with quadriplegia and who are bedridden.8
value was 2.3Ϯ1.1L, the mean VC was 2.5Ϯ1.4L, and the
In this study, patients showed a restrictive respiratory pat-
mean PEF was 292Ϯ152L/s. All are presented with median
tern. Their immobility, fatigue, reduced respiratory function,
tobacco use, dysphagia, aspiration, and use of medication re-
The baseline FSS score did not differ between the training
inforced their primary restrictive respiratory patterns. There-
group (mean, 5.0Ϯ1.3) and the control group (mean, 4.5Ϯ1.3),
fore, sustained treatment that combines physical and respira-
but their scores were significantly higher than scores for able-
tory muscle training should be initiated early to preserve
bodied healthy adults (mean, 2.3Ϯ0.7).37 Baseline subjective
respiratory function and to avoid aspiration pneumonia. The
perception of physical endurance in the morning after bathing
importance of combined physical training and respiratory mus-
and dressing, as rated on the RPE scale, did not differ between
cle training has been confirmed in several studies of patients
the training group (median, 13; range, 9 –16) and the control
group (median, 14; range, 9 –17). There was no correlation
Previous studies39-41 have shown the effect of respiratory
muscle training and/or expiratory muscle training to improverespiratory muscle strength and coughing ability in patients
Posttraining
with MS. To our knowledge, no other studies have been pub-
Respiratory muscle function, as evaluated by the PImax,
lished concerning inspiratory muscle training in patients with
improved after 10 weeks for the patients in the training group
MS. To obtain an effective cough, a deep inspiration, elastic
(PϽ.008) (fig 1), but it remained unchanged in the control
recoil, abdominal muscle pressure, and glottis closure are
group. PEmax was also improved for patients in the training
needed.13 In this study, the patients had paralysis or weakness
group (PϽ.02), but did not change in the control group (table
in the expiratory muscles, as indicated by the reduced PEmax.
2). The improvement in PImax after 10 weeks was significantly
Most of the patients also showed laryngeal and pharyngeal
higher than the improvement in the control group (PϽ.01), but
dysfunction and, thus, an impaired glottis function and diffi-
the improvement in PEmax failed to reach statistical signifi-
culty in breathing as deeply as needed to produce an effective
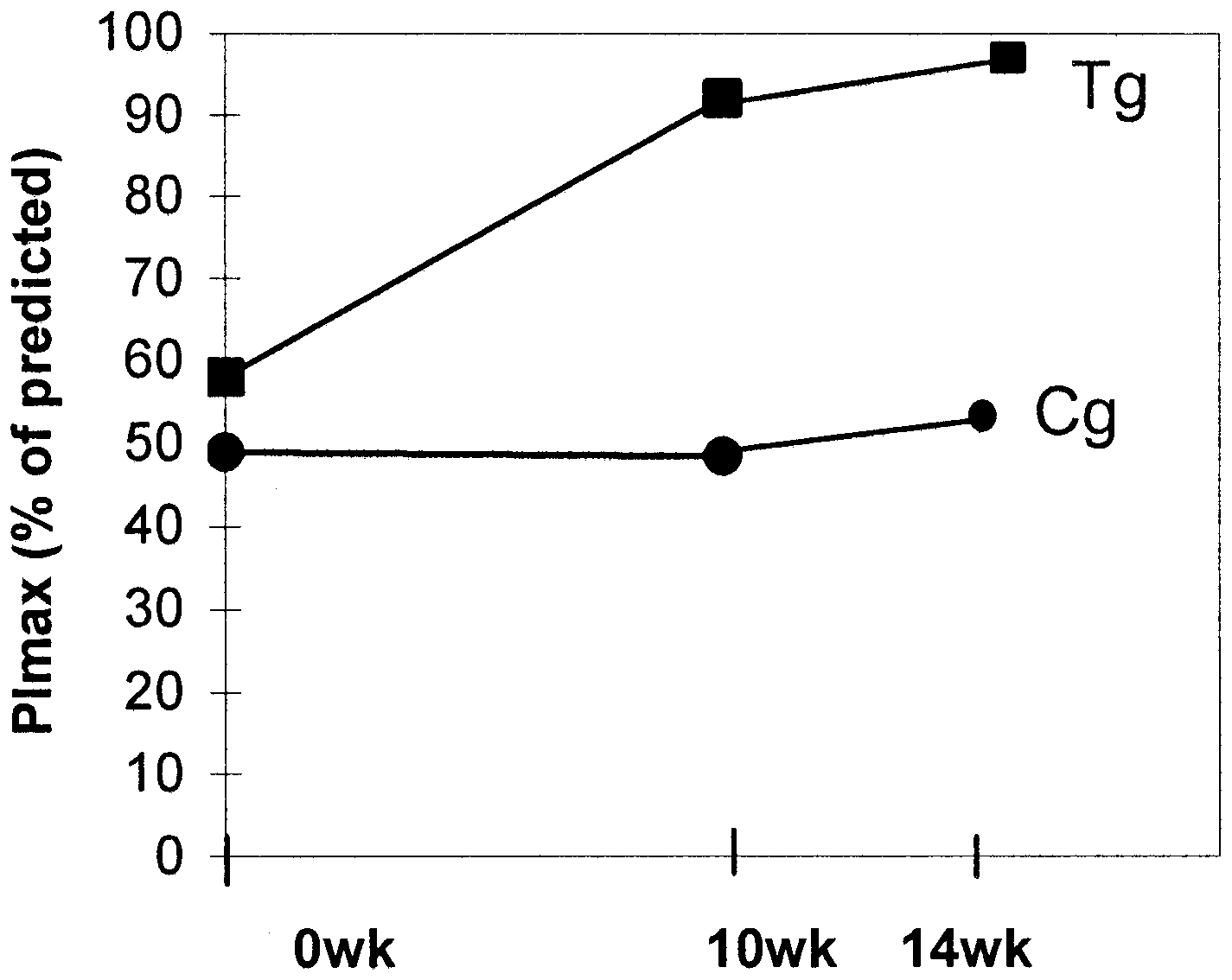
cance between the groups. Figure 2 shows the median PImaxpercentage of predicted normal values in both groups overtime. The improvement in PImax percentage of predicted nor-mal values remained unchanged in the training group after 1month, compared with the posttraining values (fig 2).
Respiratory function values remained unchanged in the
training group after 10 weeks and did not differ between thegroups.
The mean FSS scores were 4.7Ϯ1.4 in the training group and
5.6Ϯ1.4 in the control group. No significant differences couldbe found between the groups. The score of subjective percep-tion of physical endurance in the morning after bathing anddressing did not change after training compared with baselinescores in both groups. There was no evidence of enhancedactivities during the week that were not related to the patients’ordinary ADLs, as perceived by the patients. No complicationswere reported or observed during the 10 weeks. DISCUSSION Fig 2. PImax percentage (median) of predicted normal values, mea- sured by mouth pressure meter, from baseline to after training
In this study, specific inspiratory threshold loading training,
(10wk) and 4 weeks after training (14wk) in the training group (Tg)
twice every other day, by 3 sets of 10 loaded inspirations
and the control group (Cg). Arch Phys Med Rehabil Vol 84, July 2003 INSPIRATORY MUSCLE TRAINING IN MS, Klefbeck
cough. The coughing effectiveness might have been improved
such maneuvers, Fiz et al29 recommend that a minimum of 9
by the IMT, just as the PImax and PEmax improved. Interest-
technically acceptable maneuvers should be performed. Smelt-
ingly, our patients showed a strong coughing reflex, which may
zer and Lavietes30 assessed the reliability of PImax and PEmax
have been caused by retention in the trachea. Unfortunately,
in a group of healthy controls and patients with MS and
this reflex may be impaired in the later stages of MS and in
concluded that 3 maneuvers were needed to obtain a reproduc-
patients who are unconscious. Gosselink et al41 studied the
ible value in the former group and more than 3 maneuvers were
effect of expiratory muscle training in patients with MS with
necessary for patients with MS. Previous studies9,14 have stated
approximately the same level of neurologic deficit as in our
that performing a respiratory function test can be laborious and
study (median EDSS score, 8.5; range, 6.5–9.5), using a resis-
stressful for patients with MS and that, in fact, such patients
tive respiratory device. They showed improvement in both the
show a poor activity tolerance and often complain of fatigue.
PImax and coughing in the training group, which reinforces the
Therefore, respiratory function tests should be singly per-
fact that effective inspiration is an important part of the ability
formed in these patients because of the rapid onset of fatigue.
The patients in our study had a manifest and more severe
Physical endurance results in our study were dissimilar to
neurologic deficit than did those in the study by Smeltzer.30
those in a study by Klefbeck et al24 of patients with polio, who
Our patients performed the maneuvers at least 3 times and
showed improvement in the performance of ADLs after in-
mentioned fatigue often during or after the test. The patients
spiratory muscle endurance training with an IMT device. This
were, however, probably highly motivated, because they were
difference may be because patients in our study were more
self-enrolled in the respiratory training study. This high level of
affected by neurologic disorders (with 70% of patients wheel-
motivation may be the most apparent explanation for the high
chair bound and 30% bedridden) and the appearance of fatigue.
reliability in this study. Variation resulting from daytime fa-
The patients with prior polio were also users of part-time
tigue was avoided by testing each patient at the same time each
assisted ventilation and used the assisted ventilation before and
after the training program; also, the designs of the 2 studies
The questions remain whether the threshold inspiratory
differed. In our study, no patient experienced dyspnea while
training load and the training intensity were too low or too high
performing this kind of activity, because all patients reached
and whether the training period needs to be extended to achieve
the level of fatigue before dyspnea set in, an observation also
improvement in the level of physical activity and fatigue se-
verity. This study’s purpose was to strengthen inspiratory mus-
The improvement in inspiratory and enhanced expiratory
cles; however, the variables of physical activity and fatigue
muscle strength in the training group was apparent after 6
severity might be associated with endurance rather than
weeks, and significant changes were found after 10 weeks of
strength training of inspiratory muscles. The number of pa-
training. The improvements continued after 10 weeks for 4
tients in the training group was small, which can be explained
patients who continued the training protocol, but it did not
because the number of MS survivors at such a high level of
change in the other patients. The other 3 patients in the training
disability is not large (approximately 20% of the total MS
group continued their IMT periodically after 10 weeks, which
patients in the selected region). A multicenter trial would be
was not difficult because of its training design (it was short and
necessary to obtain a larger number of participants.
did not require much time). The subjective outcome of interestin this study was that the patients in the training group reported
CONCLUSION
that after 10 weeks of IMT, deep inspiration was easier to
The MS patients in this study, with its randomized, con-
perform. They thought that the training was most effective and
trolled trial, showed a significant improvement of inspiratory
was a good way to resist the symptoms of MS; furthermore,
muscle strength after 10 weeks of supervised training. The
they were more confident and more motivated to do additional
improvements were evident 1 month after the study ended.
activities. All patients in the training group knew that training
It would be of interest to do a 1-year follow-up to establish
with the IMT device was complementary to other physical
whether the positive outcomes are still present. Furthermore,
training. Most of the patients were restricted to a wheelchair or
the optimal training stimulus needed to elicit a clinical benefit
to bed much of the time and were limited in their physical
in physical activity and fatigue severity is not known in patients
activities because of weakness, an increased body temperature
with MS. However, this study should provide a better under-
as a result of such activities, and a worsening of the fatigue
standing of respiratory muscle weakness and patients’ limited
symptom. This has also been reported in previous studies.10,14
capability resulting from severe handicap and fatigue and
In this regard, our patients were not able to reach optimal
should, therefore, enable therapists to design more effective
effects of the physical activities; therefore, additional respira-
physical and respiratory muscle training protocols.
tory training could be beneficial for them. To ensure propertraining load and no adverse effects, careful assessment of
References
1. Lucchinetti CF, Brueck W, Rodriguez M, Lassmann H. Multiple
sclerosis: lessons from neuropathology. Semin Neurol 1998;18:
A limitation of this study was our assessment of baseline
values by spirometry and mouth pressure measurements, be-
2. Lassmann H. Neuropathology in multiple sclerosis: new concepts.
cause both methods are effort and motivation dependent. Al-
though the maneuvers were repeated at least 3 times until no
3. Mathews WB, Acheson ED, Batchelro JR, Weller RO. McAlp-
further enhancement was observed, careful instruction was
ine’s multiple sclerosis. Course and prognosis. London: Churchill
given, and patients were well motivated. However, it was
sometimes difficult to achieve full cooperation and coordina-
4. Poser CM, Paty DW, Scheinberg L, et al. New diagnostic criteria
tion from all the patients. Consequently, the observed P
for multiple sclerosis: guidelines for research protocols. Ann Neu-
PEmax, and respiratory function values may have been under-
5. Kurtzke JF. Clinical definition for multiple sclerosis treatment
To determine the number of maximal mouth pressure ma-
6. Rudick RA, Schiffer RB, Schwetz KM, Herndon RM. Multiple
neuvers and obtain a reproducible value of PImax and PEmax in
sclerosis. The problem of incorrect diagnosis. Arch Neurol 1986;
patients with COPD who are untrained and inexperienced in
Arch Phys Med Rehabil Vol 84, July 2003 INSPIRATORY MUSCLE TRAINING IN MS, Klefbeck
7. De Troyer A, Pride NB. The respiratory system in neuromuscular
24. Klefbeck B, Lagerstrand L, Mattsson E. Inspiratory muscle train-
disorders. In: Roussos C, Macklem PT, editors. The thorax: lung
ing in patients with prior polio who use part-time assisted venti-
biology in health and disease. New York: Marcel Dekker; 1985.
lation. Arch Phys Med Rehabil 2000;81:1065-71.
25. McCool FD, McCann DR, Leith DE, Hoppin FG Jr. Pressure-flow
8. Smeltzer SC, Utell MJ, Rudick RA, Herndon RM. Pulmonary
effects on endurance of inspiratory muscles. J Appl Physiol 1986;
function and dysfunction in multiple sclerosis. Arch Neurol 1988;
26. Kurtzke JF. Rating neurologic impairment in multiple sclerosis:
9. Buyse M, Demedts M, Meekers J, Vandegaer L, Rochette F,
an expanded disability status scale (EDSS). Neurology 1983;33:1444-52.
Kerkhofs L. Respiratory dysfunction in multiple sclerosis: a pro-
27. Black LF, Hyatt RE. Maximal respiratory pressures: normal val-
spective analysis of 60 patients. Eur Respir J 1997;10:139-45.
ues and relationship to age and sex. Am Rev Respir Dis 1969;99:
10. Tantucci C, Massucci M, Piperno R, Betti L, Grassi V, Sorbini
CA. Control of breathing and respiratory muscle strength in pa-
28. Larsson K, Hedenstro¨m H, Malmberg P. Learning effects, varia-
tients with multiple sclerosis. Chest 1994;105:1163-70.
tion during office hours and reproducibility of static and dynamic
11. Sadovnick AD, Eisen K, Ebers GC, Paty DW. Cause of death in
spirometry. Respiration 1987;51:214-22.
patients attending multiple sclerosis clinics. Neurology 1991;41:
29. Fiz JA, Montserrat JM, Picado C, Plaza V, Augusti-Vidal A. How
many manoeuvers should be done to measure maximal inspiratory
12. Howard RS, Wiles CM, Hirsch NP, Loh L, Spencer GT, Newsom-
mouth pressure in patients with chronic airflow obstruction? Tho-
Davis J. Respiratory involvement in multiple sclerosis. Brain
30. Smeltzer SC, Lavietes MH. Reliability of maximal respiratory
13. Hough A. Physiotherapy in respiratory care: a problem-solving
pressures in multiple sclerosis. Chest 1999;115:1546-52.
approach to respiratory and cardiac management. 2nd ed. London:
31. Larson J, Kim MI. Reliability of maximal inspiratory pressure.
14. Foglio K, Clini E, Facchetti D, et al. Respiratory muscle function
32. Wilson SH, Cooke NT, Edwards RH, Spiro SG. Predicted normal
and exercise capacity in multiple sclerosis. Eur Respir J 1994;7:
values for maximal respiratory pressures in Caucasian adults and
15. Ford H, Trigwell P, Johnson M. The nature of fatigue in multiple
33. Pollard AJ, Mason NP, Barry PW, et al. Effect of altitude on
spirometric parameters and the performance of peak flow meters.
sclerosis. J Psychosom Res 1998;45:33-8.
16. Vercoulen JH, Hommes OR, Swanink CM, et al. The measure-
34. Dirksen A, Madsen F, Pedersen OF, Vedel AM, Kok-Jensen A.
ment of fatigue in patients with multiple sclerosis: a multidimen-
Long term performance of a hand held spirometer. Thorax 1996;
sional comparison with patients with chronic fatigue syndrome
and healthy subjects. Arch Neurol 1996;53:642-9.
35. Standardization of lung function tests. Report working party. Bull
17. Johnson PH, Cowley AJ, Kinnear WJ. Evaluation of the
Eur Physiopathol Respir 1983;19 Suppl 5:1-95.
THRESHOLD trainer for inspiratory muscle endurance training:
36. Standardization of spirometry—1987 update. Statement of the
comparison with the weighted plunger method. Eur Respir J
American Thoracic Society. Am Rev Respir Dis 1987;136:1285-
18. Nield MA. Inspiratory muscle training protocol using a pressure
37. Krupp LB, LaRocca NG, Muir-Nash J, Steinberg AD. The fatigue
threshold device: effect on dyspnea in chronic obstructive pulmo-
severity scale. Application to patients with multiple sclerosis and
nary disease. Arch Phys Med Rehabil 1999;80:100-2.
systemic lupus erythematosus. Arch Neurol 1989;46:1121-3.
19. Weiner P, Azgad Y, Ganam R, Weiner M. Inspiratory muscle
38. Borg GA. Psychophysical bases of perceived exertion. Med Sci
training in patients with bronchial asthma. Chest 1992;102:1357-
39. Smeltzer SC, Lavietes MH, Cook SD. Expiratory training in
20. Weiner P, Azgad Y, Ganam R. Inspiratory muscle training com-
multiple sclerosis. Arch Phys Med Rehabil 1996;77:909-12.
bined with general exercise reconditioning in patients with COPD.
40. Olgiati R, Girr A, Hugi L, Haegi V. Respiratory muscle training
in multiple sclerosis: a pilot study. Schweiz Arch Neurol Psychiatr
21. Harver A, Mahler DA, Daubenspeck A. Targeted inspiratory
muscle training improves respiratory muscle function and reduces
41. Gosselink R, Kovacs L, Ketelaer P, Carton H, Decramer M.
dyspnea in patients with chronic obstructive pulmonary diseases.
Respiratory muscle weakness and respiratory muscle training in
severely disabled multiple sclerosis patients. Arch Phys Med
22. Lisboa C, Munoz V, Beroiza T, Leiva A, Cruz E. Inspiratory
muscle training in chronic airflow limitation: comparison of 2different training loads with a threshold device. Eur Respir J
Suppliers
a. Micro Medical Ltd, 6 Ambley Green, Gillingham Business Park,
23. Eastwood PR, Hillman DR, Finucane KE. Ventilatory responses
to inspiratory threshold loading and role of muscle fatigue in task
b. Health Scan Products Inc, 908 Pompton Ave, Unit B2, Cedar
failure. J Appl Physiol 1994;76:185-95. Arch Phys Med Rehabil Vol 84, July 2003
Verva Announces Results of Successful VVP808-002 Phase 2 Clinical Trial in Type 2 Diabetes and Outcome of Annual General Meeting Melbourne, Australia (06 June 2012). Verva Pharmaceuticals Ltd. (“ Verva ” or the “ Company ”) announced the top-line results of the recently-completed VVP808-002 Phase 2 clinical proof-of- concept study with the Company’s insulin sensitizer VVP808 (m
IJCCM October-December 2003 Vol 7 Issue 4 Indian J Crit Care Med July-September 2007 Vol 11 Issue 3 Review Article TNF-alpha inhibitors: Current indications Rashmi Sharma, Chaman Lal Sharma* Advances in the DNA hybrid technology led to the development of various biologicals that specifi cally target TNF-α. There are currently three anti- TNF-α drugs available- etanercept, infl ix
 INSPIRATORY MUSCLE TRAINING IN MS, Klefbeck
INSPIRATORY MUSCLE TRAINING IN MS, Klefbeck