D R U G T H E R A P Y
50 percent is conjugated to glucuronic acid in thekidneys.9 Thus, in patients with renal insufficiency,the plasma half-life of furosemide is prolonged be-
A L A S T A I R J . J . W O O D , M . D. , Editor
cause not only urinary excretion but also renal con-jugation is decreased7,8,10-14 (Table 1). The other twoloop diuretics available in the United States, bumet-
DIURETIC THERAPY
anide and torsemide, are largely metabolized by theliver (50 and 80 percent, respectively)4,15-17; there-
fore, their half-lives are not prolonged in patientswith renal insufficiency, although renal disease im-
pairs their delivery to the tubular fluid. In contrast,
in patients with liver disease, the plasma half-lives of
these drugs, loop diuretics such as furose-
these drugs are prolonged, and more drug reaches
mide are perhaps the most frequently prescribed,
and their clinical pharmacology is better understood
Although the pharmacologic characteristics of eth-
than is that of other diuretics. This review will there-
acrynic acid have been characterized as typical of
fore focus on this class of diuretics, but others will
those of loop diuretics, there are no data on its phar-
macokinetics. The drug’s ototoxic potential is greaterthan that of other loop diuretics, and it is therefore
CLINICAL PHARMACOLOGY
now given only to patients who have allergic reac-
OF DIURETICS Pharmacokinetics
The pharmacokinetics of thiazide diuretics (Table
1) have been studied less extensively than those of
The pharmacologic characteristics of all loop di-
loop diuretics. Some thiazide diuretics are metabo-
uretics are similar. Therefore, a lack of response to
lized primarily by the liver (e.g., bendroflumethia-
adequate doses of one loop diuretic militates against
zide, polythiazide, and indapamide); others are pri-
the administration of another loop diuretic; instead,
marily excreted in unchanged form in the urine (e.g.,
combinations of diuretics with different mechanisms
chlorothiazide, chlorthalidone, hydrochlorothiazide,
hydroflumethiazide, and trichlormethiazide). There
Loop diuretics block the sodium–potassium–chlo-
is little information about the influence of disease on
ride transporter, thiazide diuretics block the electro-
the pharmacokinetics of these drugs.
neutral sodium–chloride transporter, and amiloride
Since amiloride is excreted by the kidneys, renal
and triamterene block apical sodium channels.1-6 All
disease prolongs its plasma half-life,19,20 whereas liver
diuretics except spironolactone reach these luminal
disease has little effect on the drug.20 The pharma-
transport sites through the tubular fluid; all but os-
cokinetics of triamterene are complicated, because it
motic diuretics are actively secreted into the urine by
is converted to an active metabolite by the liver, and
proximal tubule cells. A high degree of protein bind-
the metabolite is then secreted into the tubular flu-
ing (>95 percent) limits glomerular filtration,1-6 even
id.7,21,22 Renal disease impairs the secretion of this
in patients with hypoalbuminemia. In effect, bind-
metabolite into the tubular fluid.21 The amount of
ing to serum proteins traps the diuretic in the vas-
metabolite that reaches the tubular fluid is also re-
cular space so that it can be delivered to secretory
duced in patients with liver disease, because of di-
sites of proximal tubule cells. Loop and thiazide di-
minished formation of the metabolite in the liver.22
uretics and acetazolamide are secreted through the
The pharmacokinetics of spironolactone are even
organic-acid pathway,1-4 and amiloride and triamter-
more complex, because it is converted to numerous
About 50 percent of a dose of furosemide is ex-
In addition to the routes of metabolism, the phar-
creted in unchanged form into the urine7,8; the other
macokinetic features of diuretics that are clinicallyimportant are bioavailability and half-life. On aver-age, the amount of an oral dose of furosemide that is
From the Division of Clinical Pharmacology, Department of Medicine,
absorbed is 50 percent, but it ranges from 10 to 100
Indiana University School of Medicine, Emerson Hall 317, 545 Barnhill
percent.7 This wide range makes it difficult to predict
Dr., Indianapolis, IN 46202-5124, where reprint requests should be
how much furosemide will be absorbed in an indi-
1998, Massachusetts Medical Society.
vidual patient, and different doses must be tried be-
Downloaded from www.nejm.org at HOUSTON ACADEMY OF MEDICINE on January 3, 2008 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
TABLE 1. PHARMACOKINETICS OF DIURETIC DRUGS.* DIURETIC BIOAVAILABILITY ELIMINATION HALF-LIFE
†Values are for the active metabolite.
fore the drug is judged to be ineffective. In contrast,
Pharmacodynamics
absorption of bumetanide and torsemide is nearly
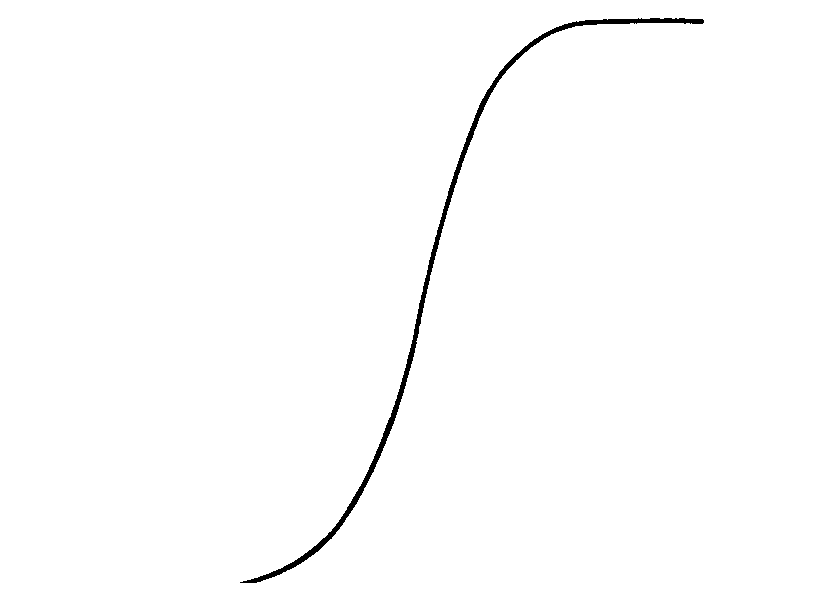
The relation between the arrival of a diuretic at its
complete, ranging from 80 to 100 percent (Table
site of action (determined on the basis of the rate of
1).18,25,26 There is therefore probably less need for ti-
urinary excretion) and the natriuretic response de-
tration of these drugs when one is switching from
termines the pharmacodynamics of the drug (Fig.
an intravenous to an oral dose. The variation in the
1).1,17 This relation holds for all loop diuretics, al-
absorption of furosemide may be clinically impor-
though the curve may be shifted to the right or the
tant; patients with heart failure treated with a com-
left.7 This means that in any one patient, the maxi-
pletely absorbed loop diuretic (torsemide) may re-
mal response to each loop diuretic is the same. The
quire hospitalization less often and have a better
same is true for thiazide diuretics. The choice of an
quality of life than patients treated with furosemide.27
agent within either class of diuretics is governed by
The amount of loop diuretic that is absorbed is nor-
factors such as pharmacokinetic differences and cost.
mal in patients with edema,18,25,26,28-32 although ab-
Several pharmacodynamic features of diuretics are
sorption is slower than normal, particularly in those
clinically important. There is a threshold quantity of
drug that must be achieved at the site of action in
The plasma half-life of a diuretic determines the fre-
order to elicit a response. The diuretic must there-
quency of administration. Thiazide and distal diuretics
fore be titrated in each patient in order to determine
have sufficiently long half-lives that they can be admin-
the dose that will deliver enough drug to the site of
istered once or twice a day. The plasma half-lives of
action to reach the steep portion of the curve shown
loop diuretics range from about one hour for bumet-
in Figure 1 (effective dose). In addition, one can de-
anide to three to four hours for torsemide; the half-life
termine the lowest dose that elicits a maximal re-
of furosemide is one and a half to two hours.7 A truly
sponse and that should therefore not be exceeded
long acting loop diuretic is not available. Once a dose
(maximal dose). In normal subjects, an intravenous
of a loop diuretic has been administered, its effect dis-
dose of 40 mg of furosemide or an equivalent dose
sipates before the next dose is given. During this time,
of other loop diuretics results in a maximal response,
the nephron avidly reabsorbs sodium, resulting in so-
which is the excretion of 200 to 250 mmol of sodium
called rebound sodium retention,33,34 which may be
in 3 to 4 liters of urine over a period of three to four
sufficient to nullify the prior natriuresis.
Downloaded from www.nejm.org at HOUSTON ACADEMY OF MEDICINE on January 3, 2008 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y
thiazide will cause diuresis in patients with mild re-
nal insufficiency, the response in patients with a cre-atinine clearance of less than about 50 ml per min-ute is poor.
In patients with a creatinine clearance of 15 ml
per minute, 1⁄5 to 1⁄10 as much loop diuretic is secret-ed into the tubular fluid as in normal subjects.7,8
Thus, a large dose must be given to attain an effec-tive amount of diuretic in the tubular fluid (Table2). The relation between the rate at which the di-uretic is excreted and the response to it is the samein patients with renal insufficiency as it is in normalsubjects.50,51 Thus, the remaining nephrons in pa-
tients with renal insufficiency retain their responsive-
ness to the diuretic; the problem is getting enough
Figure 1. Pharmacodynamics of a Loop Diuretic.
A frequent question is, What is the largest single
The relation between the natriuretic response and the amount
dose of a loop diuretic that can be given to a patient
of diuretic reaching the site of action is represented by a sig-
with severe renal insufficiency? The maximal natriu-
retic response occurs with intravenous bolus dosesof 160 to 200 mg of furosemide or the equivalentdoses of bumetanide and torsemide,50,52 and nothingis gained by using larger doses. Some patients may re-
Diuretic Tolerance
quire these large doses several times a day. The maxi-
There are two forms of diuretic tolerance. Short-
mal response is the excretion of about 20 percent of
term tolerance, so-called braking, refers to a decrease
filtered sodium. In a patient with a creatinine clear-
in the response to a diuretic after the first dose has
ance of 15 ml per minute, this means that about 25
been administered. This can be prevented by restor-
mmol of sodium will be excreted. If the patient in-
ing diuretic-induced loss of volume.35-37 Teleologically,
gests 75 mmol of sodium per day, then the single dose
this response appropriately protects intravascular vol-
causing 25 mmol to be excreted must be administered
ume. The mechanism by which short-term tolerance
three times per day, and sodium will be retained if the
occurs is unclear. It may be mediated by activation of
intake is higher. Single intravenous bolus doses of 160
angiotensin II or the sympathetic nervous system, but
to 200 mg can occasionally cause transient tinni-
neither the inhibition of angiotensin-converting en-
tus,53,54 but this effect can be minimized by adminis-
zyme nor adrenergic blockade, separately or together,
tering the dose over a period of 20 to 30 minutes.
The bioavailability of loop diuretics is the same in
With long-term administration of a loop diuretic,
patients with renal insufficiency as it is in normal
the solute that escapes from the loop of Henle floods
subjects.25,26,28-32 Therefore, the intravenous and oral
more distal regions of the nephron. By unknown
doses of bumetanide and torsemide are similar. For fu-
mechanisms, increased exposure to solute causes hy-
rosemide, the usual maximal oral dose is twice the
pertrophy of distal nephron segments, with concom-
intravenous dose (160 to 320 mg in patients with
itant increases in the reabsorption of sodium.41-45
moderate renal insufficiency and 320 to 400 mg in
Sodium that escapes from the loop of Henle is there-
those with severe renal insufficiency). However, the
fore reabsorbed at more distal sites, decreasing over-
absorption of furosemide varies from one patient to
all diuresis. The result is long-term tolerance of the
another. Occasionally, a very small fraction of the dose
loop diuretic. Thiazide diuretics block the nephron
is absorbed, and very large oral doses are therefore
sites at which hypertrophy occurs, accounting for the
required. Before concluding that a patient has not had
synergistic response to the combination of a thiazide
a response to furosemide and contemplating the use
and a loop diuretic.46-49 This phenomenon reinforces
of dialysis to control volume, the physician should
the logic of using combinations of loop and thiazide
administer larger oral doses of furosemide or a maxi-
diuretics in patients who do not have adequate re-
mal oral dose of either bumetanide or torsemide.
sponses to optimal doses of a loop diuretic.
In patients who have poor responses to intermit-
DIURETIC THERAPY IN PATIENTS
tent doses of a loop diuretic, a continuous intrave-
WITH EDEMA
nous infusion can be tried. If an effective amount ofthe diuretic is maintained at the site of action at all
Renal Insufficiency
times, a small but clinically important increase in the
A loop diuretic is the diuretic of choice in patients
response may occur.55 There are other reasons to con-
with renal insufficiency. Although a large dose of a
sider giving a continuous infusion of a loop diuretic.
Downloaded from www.nejm.org at HOUSTON ACADEMY OF MEDICINE on January 3, 2008 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
TABLE 2. THERAPEUTIC REGIMENS FOR LOOP DIURETICS IN PATIENTS WITH DIMINISHED RESPONSES TO INITIAL THERAPY. RENAL INSUFFICIENCY PRESERVED RENAL FUNCTION*
Mechanism of diminished Impaired delivery to site of action
more frequent administration of effective dose
*Preserved renal function is defined as a creatinine clearance of more than 75 ml per minute.
†If the maximal dose is reached without an adequate response, a thiazide diuretic should be administered as adjunctive therapy, with the dose determined
according to renal function, and alternative treatment of the primary disease should be considered.
It may be easier for nursing staff to give a continu-
loop diuretic is to add an oral thiazide diuretic.56-58
ous infusion than intermittent bolus intravenous dos-
Metolazone is frequently given in the United States,
es. In addition, with a continuous infusion, decisions
whereas other thiazides are given elsewhere. The phar-
about the timing of doses of an additional diuretic
macologic characteristics of metolazone are similar
are simplified. Finally, by closely monitoring urinary
to those of other thiazides. Some formulations of
output, one can unambiguously determine whether
the drug are absorbed poorly and slowly, and it has
a long elimination half-life (about two days).7 Thus,
Before administering a continuous infusion of a
metolazone accumulates over a period of about 10
loop diuretic, the physician should give a loading
days. Other thiazides have the same synergistic effects
dose in order to decrease the time needed to achieve
when combined with a loop diuretic.46-49 Since the
therapeutic drug concentrations (Table 3); other-
absorption of other thiazides, such as hydrochloro-
wise, 6 to 20 hours is required to achieve a steady
thiazide, is more rapid and predictable, they may be
state, depending on the diuretic used. The rate of
the continuous infusion is governed by the patient’s
Because thiazide diuretics must reach the lumen
renal function. If an adequate response has not oc-
of the nephron to be effective, higher doses are re-
curred after the drug has been given for an hour, the
quired in patients with renal insufficiency than in
loading dose should be repeated, and then the infu-
other patients.56-58 Patients with mild-to-moderate
sion rate can be increased, as shown in Table 3.
renal insufficiency require 50 to 100 mg of hydro-
Another strategy to enhance the response to a
chlorothiazide per day; those with more severe dis-ease require 100 to 200 mg per day. Thiazides canbe administered once or twice a day.
In summary, a patient with edema caused by renal
insufficiency should be given increasing doses of a
TABLE 3. DOSES FOR CONTINUOUS INTRAVENOUS INFUSION
loop diuretic until an effective dose is identified (Fig.
2 and Table 2). The effective dose should be given asoften as needed to maintain the response, according
INTRAVENOUS
to the patient’s ability to restrict sodium intake and
DIURETIC LOADING DOSE INFUSION RATE*
the duration of action of the drug. If the response is
inadequate after the maximal dose has been reached,
a thiazide should be added (Fig. 2). If diuresis remainsinadequate, the only recourse is dialysis. The Nephrotic Syndrome
It is often difficult to achieve a satisfactory diuresis
in patients with the nephrotic syndrome. In suchpatients, serum albumin concentrations are frequently
*Before the infusion rate is increased, the loading dose should be admin-
low, and the diffusion of diuretics into the extracel-
Downloaded from www.nejm.org at HOUSTON ACADEMY OF MEDICINE on January 3, 2008 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y
Administer as frequently asmnecessary to maintain response
For added natriuresis, if urinary excretion of sodium decreasedmand urinary excretion of potassium increased
Figure 2. Algorithm for Diuretic Therapy in Patients with Edema Caused by Renal, Hepatic, or Cardiac Disease.
Cl denotes creatinine clearance, HCTZ hydrochlorothiazide, and bid twice a day.
lular fluid is therefore increased. This may reduce the
fore unnecessary. This conclusion may not be appli-
amount of drug delivered to renal secretory sites.59 If
cable to patients with serum albumin concentrations
so, the efficacy of diuretic therapy may be increased
of less than 2 g per deciliter. In such patients, it may
by administering a mixture of albumin and a loop di-
be reasonable to try combined infusions.
uretic; in several patients with severe hypoalbumine-
The diuretic response is subnormal in patients with
mia, an infusion of 30 mg of furosemide mixed with
the nephrotic syndrome, despite an adequate rate of
25 g of albumin enhanced diuresis.59 However, in
excretion of drug into the tubular fluid. In animals,
most patients with the nephrotic syndrome60,61 (and
and presumably also in humans, diuretics become
in those with cirrhosis10-14), renal tubular secretion of
bound to albumin in tubular fluid, resulting in a di-
furosemide is normal (unless the patient also has re-
minished amount of unbound, active drug and a de-
nal insufficiency), and combined infusions are there-
creased diuretic response.62-65 When urinary albumin
Downloaded from www.nejm.org at HOUSTON ACADEMY OF MEDICINE on January 3, 2008 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
concentrations exceed 4 g per liter, one half to two
with cirrhosis. In patients with normal renal func-
thirds of the diuretic that reaches the tubular fluid is
tion, the diuretic concentration in the tubular fluid
bound to albumin in the fluid. Consequently, doses
is normal.10-14,18 Thus, a decreased response to a loop
two to three times the normal dose are needed to
diuretic in a patient with cirrhosis is not due to de-
deliver adequate amounts of unbound, active drug
creased delivery of the drug to its site of action, and
to the site of action (Table 2). In addition, patients
there is no need to administer large doses, unless the
with the nephrotic syndrome may have a diminished
patient has concomitant renal dysfunction.
response because of a decrease in the drug’s action
Responses to loop diuretics are decreased in pa-
on cells within the loop of Henle66 and because of
tients with cirrhosis because the relation between
increased proximal or distal reabsorption of sodi-
the excretion rate and the natriuretic response (Fig.
um.7 Doses must therefore be sufficient to overcome
1) is shifted downward and to the right, so that the
urinary binding and must be administered more fre-
response to a maximally effective dose is substantial-
quently than in other patients, and combinations of
ly less than the normal response.10-14,18 The cause of
this shift is unknown. The maximal response in a pa-
In summary, several mechanisms result in a de-
tient with severe cirrhosis may be the excretion of
creased diuretic response in patients with the nephrot-
only 25 or 30 mmol of sodium, as compared with
ic syndrome (Table 2). Overcoming the binding of a
200 to 250 mmol in normal subjects. This response
diuretic to albumin in urine requires the administra-
is not increased with larger doses, but more frequent
tion of a dose that is sufficiently high to result in
doses, given alone or with a thiazide diuretic, may
normal concentrations of unbound diuretic in the
tubular fluid. Concomitant decreases in creatinine
In summary, spironolactone is the mainstay of di-
clearance make it necessary to increase the dose even
uretic therapy for patients with cirrhosis, with the
more. The diminished response in the loop of Henle
addition of a thiazide, a loop diuretic, or both as
mandates frequent doses and often the addition of a
necessary (Fig. 2). Single high doses of a thiazide or
thiazide diuretic, the dose of which is governed by
loop diuretic are inappropriate; instead, moderate
the level of renal function (Fig. 2). If these strategies
doses should be given several times daily, and dietary
fail and the patient has severe hypoalbuminemia, a
sodium restriction should be encouraged.
trial of a mixture of a loop diuretic and albumin canbe tried. Other alternatives entail more aggressive
Congestive Heart Failure
treatment of the nephrotic syndrome.
Patients with edema caused by mild congestive
heart failure should be treated initially with a thia-
Cirrhosis
zide diuretic (Fig. 2), but most will require a loop
The mainstay of diuretic therapy for patients with
diuretic. In patients with normal or nearly normal
cirrhosis who have edema is spironolactone, because
renal function, the delivery of loop diuretics to the
secondary hyperaldosteronism is an important cause
tubular fluid is normal.69-71 The rate of absorption of
of sodium and water retention in such patients.23
loop diuretics is slowed in patients with severe heart
Spironolactone causes only a moderate diuresis, which
failure; therefore, the maximal response occurs four
is desirable because greater diuresis may compromise
hours or more after the dose has been adminis-
the intravascular volume.68 Even if patients need addi-
tered.32 Since the delivery of loop diuretics to the
tional diuretics, spironolactone should be continued
site of action is normal, patients do not need large
(Fig. 2). Repeated large-volume paracentesis may be
doses of these diuretics unless they have concomitant
used to minimize the need for more potent diuretics.
renal insufficiency (Table 2). However, renal respon-
The initial dose of spironolactone is usually 50 mg
siveness to loop diuretics may be decreased.26,72 As
per day. The drug and its active metabolites have
compared with normal subjects, patients with New
sufficiently long half-lives that once-daily adminis-
York Heart Association class II or III heart failure
tration is adequate.23,24 Its biologic half-life is such
have one fourth to one third the natriuretic response
that three to four days of treatment are needed to
to maximally effective doses of loop diuretics,26,72
attain steady-state effects. The dose can be increased
and the response is even smaller in patients with
to as much as 400 mg per day, although doses high-
more severe heart failure. The response is not in-
er than 200 mg per day are often poorly tolerated.
creased by giving large doses, but it may be increased
If maximal doses of spironolactone do not cause
by giving moderate doses more frequently (Table 2).
an adequate diuresis, a thiazide diuretic can be add-
If loop diuretics and dietary sodium restriction are
ed, the dose being determined by the level of renal
not adequate, a thiazide diuretic should be added in
function (Fig. 2). If diuresis is still inadequate, a
a dose determined according to the patient’s renal
loop diuretic can be given instead of the thiazide
function (Fig. 2). A synergistic response can result
in a profound diuresis with cardiovascular collapse.73
The pharmacokinetics and pharmacodynamics of
In addition, through sequential blocking of nephron
loop diuretics have been well characterized in patients
sites at which potassium is normally reabsorbed, sub-
Downloaded from www.nejm.org at HOUSTON ACADEMY OF MEDICINE on January 3, 2008 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y
stantial kaliuresis usually occurs. Patients given com-
the urine to be effective. If it is unfiltered, as in pa-
binations of a thiazide and a loop diuretic should
tients with renal insufficiency, it increases vascular
therefore be followed closely to prevent volume and
volume.85,86 The risks associated with mannitol, cou-
pled with the availability of other highly effective di-
In some patients, the addition of a potassium-
uretics, relegate its use to nondiuretic indications,
sparing diuretic that acts at distal nephron sites may
increase sodium excretion slightly. This response canbe predicted by measuring urinary electrolyte excre-
ADVERSE REACTIONS AND DRUG
tion. If urinary sodium and potassium concentrations
INTERACTIONS
are both low, then a distal diuretic will not be effec-
Thiazide and loop diuretics may cause skin reac-
tive because the amount of sodium delivered to the
tions and interstitial nephritis. Loop diuretics may
distal nephron is not sufficient for the diuretic to have
cause ototoxicity, usually in patients receiving both
an effect. If the urinary sodium concentration is low
very high doses and other ototoxic drugs, particular-
and the urinary potassium concentration is high, so-
ly aminoglycoside antibiotics.87,88 Ototoxicity is usu-
dium is being exchanged for potassium distally, and
ally transient. Large doses of spironolactone can cause
the addition of a diuretic that acts on distal tubules
The most serious adverse effects of diuretics are ab-
In summary, patients with congestive heart failure
normalities in fluid and electrolyte homeostasis.90
have normal delivery of loop diuretics to the tubular
Both loop and thiazide diuretics cause loss of potas-
fluid and therefore do not require large doses, but
sium and magnesium in the urine, and when admin-
the doses should be given more often than in other
istered in combination, they may result in substantial
patients (Table 2). Loop diuretics are the mainstay
depletion of these cations. Oral supplements will suf-
of therapy, but the addition of a thiazide and some-
fice in many patients, but some patients require the
times triamterene or amiloride may be helpful.
addition of a potassium-sparing diuretic. Loop di-uretics block solute reabsorption at nephron sites that
OTHER TREATMENT REGIMENS
are important for concentrating the urine and thus
Acetazolamide plus Loop Diuretics
impair urinary concentrating ability. As a result, water
Acetazolamide has been used in patients with ede-
is excreted in excess of sodium, an effect that can help
ma, usually those with congestive heart failure refrac-
correct hyponatremia. Thiazides block solute reab-
tory to high doses of loop diuretics, and in patients
sorption at nephron sites involved in the dilution of
with metabolic alkalosis. In such patients, increased
urine. Thus, the use of these agents impairs the abil-
proximal tubular reabsorption of sodium results in
ity to dilute urine, which entails a risk of hyponatre-
decreased distal delivery, rendering loop diuretics in-
mia, particularly in patients who drink large amounts
effective.76-79 In a study of normal subjects with in-
of hypotonic fluids. More distal nephron sites also
creased proximal tubular reabsorption of sodium as
contribute to urinary dilution. Although distal di-
a result of severely restricted dietary sodium intake,
uretics have not been associated with hyponatremia,
acetazolamide had a synergistic effect with furose-
the addition of distal diuretics to thiazide diuretics in-
mide.80 No studies have examined the efficacy of ace-
creases the risk of hyponatremia.90 Loop diuretics in-
tazolamide in patients with severe heart failure. Ace-
crease urinary calcium excretion and can be used to
tazolamide should be given only if a thiazide and a
treat hypercalcemia; thiazide diuretics cause urinary
loop diuretic are ineffective. A single 500-mg intra-
calcium retention and may cause hypercalcemia or
venous dose can be given in addition to a continuous
may be given to treat hypercalciuria.
intravenous infusion of a loop diuretic.
Nonsteroidal antiinflammatory drugs diminish the
response to loop and thiazide diuretics,91 because
Dopamine
they increase solute reabsorption at the thick as-
Low-dose infusions of dopamine («3 µg per kilo-
cending limb of the loop of Henle.92 These agents
gram of body weight per minute) may improve renal
can cause hyperkalemia by decreasing the secretion
hemodynamics and increase the response to loop
of renin and aldosterone.90 Presumably, the use of a
diuretics. However, recent reports have questioned
nonsteroidal antiinflammatory drug combined with
these indications and have emphasized that even low
a potassium-sparing diuretic would entail an in-
doses of dopamine may have adverse effects.81-83 In
creased risk of hyperkalemia. Other drugs that impair
one study involving patients with heart failure, do-
potassium excretion, such as angiotensin-converting–
pamine did not increase the response to a maximally
enzyme inhibitors and trimethoprim, would also
increase the risk of hyperkalemia if they were com-bined with a potassium-sparing diuretic. Mannitol
Organic acids such as probenecid can diminish
Mannitol exerts a diuretic effect at the proximal
proximal tubular secretion of thiazides and loop
tubule and loop of Henle.84 It must be filtered into
diuretics,1-4 and organic bases such as trimethoprim
Downloaded from www.nejm.org at HOUSTON ACADEMY OF MEDICINE on January 3, 2008 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
The Ne w E n g l a nd Jo u r n a l o f Me d ic i ne
and histamine H –receptor antagonists can compete
20. Sahn H, Reuter K, Mutschler E, Gerok W, Knauf H. Pharmacokinet-
ics of amiloride in renal and hepatic disease. Eur J Clin Pharmacol 1987;
for the secretion of amiloride and triamterene,5,6 but
clinically important interactions have not been re-
21. Knauf H, Möhrke W, Mutschler E. Delayed elimination of triamterene
ported. Spironolactone can decrease the renal excre-
and its active metabolite in chronic renal failure. Eur J Clin Pharmacol 1983;24:453-6. 22. Villeneuve JP, Rocheleau F, Raymond G. Triamterene kinetics and dy- namics in cirrhosis. Clin Pharmacol Ther 1984;35:831-7. CONCLUSIONS 23. Ochs HR , Greenblatt DJ, Bodem G, Smith TW. Spironolactone. Am Heart J 1978;96:389-400.
An effective diuresis can be attained in most pa-
24. Overdiek HWPM, Hermens WAJJ, Merkus FWHM. New insights into
tients with renal, hepatic, or cardiac disease by using
the pharmacokinetics of spironolactone. Clin Pharmacol Ther 1985;38:
a systematic approach to diuretic therapy. The ther-
469-74. 25. Gehr TWB, Rudy DW, Matzke GR , Kramer WG, Sica DA, Brater
apeutic strategies differ according to the type of dis-
DC. The pharmacokinetics of intravenous and oral torsemide in patients
order, because each type affects the metabolism and
with chronic renal insufficiency. Clin Pharmacol Ther 1994;56:31-8. 26. Vargo DL, Kramer WG, Black PK, Smith WB, Serpas T, Brater DC.
action of different diuretics in different ways. Di-
Bioavailability, pharmacokinetics, and pharmacodynamics of torsemide and
uretic therapy should therefore be tailored first to
furosemide in patients with congestive heart failure. Clin Pharmacol Ther
the primary disease process and then to the individ-
1995;57:601-9. 27. Murray MD, Ferguson JA, Bennett SJ, et al. Fewer hospitalizations for
ual patient. With such tailoring, treatment failure
heart failure by using a completely and predictably absorbed loop diuretic.
J Gen Intern Med 1998;13:Suppl:18. abstract. 28. Chaturvedi PR , O’Donnell JP, Nicholas JM, Shoenthal DR , Waters DH, Gwilt PR. Steady state absorption kinetics and pharmacodynamics of
Supported by grants from the General Clinical Research Center (MO1
furosemide in congestive heart failure. Int J Clin Pharmacol Ther Toxicol
RR00750) and the National Institutes of Health (R01 DK 37994 and R01
29. Van Meyel JJM, Gerlag PGG, Smits P, et al. Absorption of high dose furosemide (frusemide) in congestive heart failure. Clin Pharmacokinet REFERENCES
1992;22:308-18. 30. Bailie GR , Grennan A, Waldek S. Bioavailability of bumetanide in 1. Chennavasin P, Seiwell R , Brater DC, Liang WMM. Pharmacodynamic
grossly oedematous patients. Clin Pharmacokinet 1987;12:440-3.
analysis of the furosemide-probenecid interaction in man. Kidney Int 1979;
31. Brater DC, Day B, Burdette A, Anderson S. Bumetanide and furose-
mide in heart failure. Kidney Int 1984;26:183-9. 2. Odlind B, Beermann B. Renal tubular secretion and effects of furose- 32. Vasko MR , Cartwright DB, Knochel JP, Nixon JV, Brater DC. Furo-
mide. Clin Pharmacol Ther 1980;27:784-90.
semide absorption altered in decompensated congestive heart failure. Ann
3. Lau HSH, Shih LJ, Smith DE. Effect of probenecid on the dose-
response relationship of bumetanide at steady state. J Pharmacol Exp Ther
33. Wilcox CS, Mitch WE, Kelly RA, et al. Response of the kidney to fu-
rosemide. I. Effects of salt intake and renal compensation. J Lab Clin Med
4. Brater DC, Leinfelder J, Anderson SA. Clinical pharmacology of to-
rasemide, a new loop diuretic. Clin Pharmacol Ther 1987;42:187-92. 34. Ferguson JA, Sundblad KJ, Becker PK, Gorski JC, Rudy DW, Brater 5. Besseghir K, Rennick B. Renal tubule transport and electrolyte effects
DC. Role of duration of diuretic effect in preventing sodium retention.
of amiloride in the chicken. J Pharmacol Exp Ther 1981;219:435-41. 6. Kau ST. Handling of triamterene by the isolated perfused rat kidney. 35. Hammarlund MM, Odlind B, Paalzow LK. Acute tolerance to furo-
J Pharmacol Exp Ther 1978;206:701-9.
semide diuresis in humans: pharmacokinetic-pharmacodynamic modeling.
7. Brater DC. Diuretic pharmacokinetics and pharmacodynamics. In: van
J Pharmacol Exp Ther 1985;233:447-53.
Boxtel CJ, Holford NHG, Danhof M, eds. The in vivo study of drug ac-
36. Wakelkamp M, Alván G, Gabrielsson J, Paintaud G. Pharmacodynamic
tion: principles and applications of kinetic-dynamic modelling. Amsterdam:
modeling of furosemide tolerance after multiple intravenous administra-
tion. Clin Pharmacol Ther 1996;60:75-88. 8. Beermann B. Aspects of pharmacokinetics of some diuretics. Acta Phar- 37. Almeshari K, Ahlstrom NG, Capraro FE, Wilcox CS. A volume-inde-
macol Toxicol (Copenh) 1984;54:Suppl 1:17-29.
pendent component to postdiuretic sodium retention in humans. J Am Soc
9. Pichette V, du Souich P. Role of the kidneys in the metabolism of fu-
rosemide: its inhibition by probenecid. J Am Soc Nephrol 1996;7:345-9. 38. Kelly RA, Wilcox CS, Mitch WE, et al. Response of the kidney to 10. Fuller R , Hoppel C, Ingalls ST. Furosemide kinetics in patients with
furosemide. II. Effect of captopril on sodium balance. Kidney Int 1983;24:
hepatic cirrhosis with ascites. Clin Pharmacol Ther 1981;30:461-7. 11. Verbeeck RK, Patwardhan RV, Villeneuve JP, Wilkinson GR , Branch 39. Wilcox CS, Guzman NJ, Mitch WE, et al. Na+, K+, and BP homeo-
RA. Furosemide disposition in cirrhosis. Clin Pharmacol Ther 1982;31:
stasis in man during furosemide: effects of prazosin and captopril. Kidney
12. Villeneuve JP, Verbeeck RK, Wilkinson GR , Branch RA. Furosemide 40. Petersen JS, Shalmi M, Abildgaard U, Christensen NJ, Christensen S.
kinetics and dynamics in patients with cirrhosis. Clin Pharmacol Ther
Renal effects of a-adrenoceptor blockade during furosemide diuresis in
conscious rats. Pharmacol Toxicol 1992;70:3-12. 13. Traeger A, Häntze R , Penzlin M, et al. Pharmacokinetics and pharma- 41. Kaissling B, Stanton BA. Adaptation of distal tubule and collecting
codynamic effects of furosemide in patients with liver cirrhosis. Int J Clin
duct to increased sodium delivery. I. Ultrastructure. Am J Physiol 1988;
Pharmacol Ther Toxicol 1985;23:129-33. 14. Keller E, Hoppe-Seyler G, Mumm R , Schollmeyer P. Influence of 42. Stanton BA, Kaissling B. Adaptation of distal tubule and collecting
hepatic cirrhosis and end-stage renal disease on pharmacokinetics and phar-
duct to increased Na delivery. II. Na+ and K+ transport. Am J Physiol
macodynamics of furosemide. Eur J Clin Pharmacol 1981;20:27-33. 15. Davies DL, Lant AF, Millard NR , Smith AJ, Ward JW, Wilson GM. 43. Ellison DH, Velázquez H, Wright FS. Adaptation of the distal convo-
Renal action, therapeutic use, and pharmacokinetics of the diuretic bumet-
luted tubule of the rat: structural and functional effects of dietary salt in-
anide. Clin Pharmacol Ther 1974;15:141-55.
take and chronic diuretic infusion. J Clin Invest 1989;83:113-26. 16. Holazo AA, Colburn WA, Gustafson JH, Young RL, Parsonnet M. 44. Loon NR, Wilcox CS, Unwin RJ. Mechanism of impaired natriuretic re-
Pharmacokinetics of bumetanide following intravenous, intramuscular, and
sponse to furosemide during prolonged therapy. Kidney Int 1989;36:682-9.
oral administrations to normal subjects. J Pharm Sci 1984;73:1108-13. 45. Kobayashi S, Clemmons DR, Nogami H, Roy AK, Venkatachalam MA. 17. Brater DC, Chennavasin P, Day B, Burdette A, Anderson S. Bumetanide
Tubular hypertrophy due to work load induced by furosemide is associated
and furosemide. Clin Pharmacol Ther 1983;34:207-13.
with increases of IGF-1 and IGFBP-1. Kidney Int 1995;47:818-28. 18. Schwartz S, Brater DC, Pound D, Greene PK, Kramer WG, Rudy D. 46. Ellison DH. The physiologic basis of diuretic synergism: its role in
Bioavailability, pharmacokinetics, and pharmacodynamics of torsemide in
treating diuretic resistance. Ann Intern Med 1991;114:886-94.
patients with cirrhosis. Clin Pharmacol Ther 1993;54:90-7. 47. Sica DA, Gehr TWB. Diuretic combinations in refractory oedema 19. Smith AJ, Smith RN. Kinetics and bioavailability of two formulations
states: pharmacokinetic-pharmacodynamic relationships. Clin Pharmacokinet
of amiloride in man. Br J Pharmacol 1973;48:646-9.
Downloaded from www.nejm.org at HOUSTON ACADEMY OF MEDICINE on January 3, 2008 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
D R U G T H E R A P Y 48. Epstein M, Lepp BA, Hoffman DS, Levinson R. Potentiation of furo- 71. Perez J, Sitar DS, Ogilvie RI. Kinetic disposition and diuretic effect
semide by metolazone in refractory edema. Curr Ther Res 1977;21:656-67.
of frusemide in acute pulmonary oedema. Br J Clin Pharmacol 1980;9:
49. Olesen KH, Sigurd B. The supra-additive natriuretic effect addition of
quinethazone or bendroflumethiazide during long-term treatment with
72. Brater DC, Chennavasin P, Seiwell R. Furosemide in patients with
furosemide and spironolactone: permutation trial tests in patients with con-
heart failure: shift in dose-response curves. Clin Pharmacol Ther 1980;28:
gestive heart failure. Acta Med Scand 1971;190:233-40. 50. Voelker JR , Cartwright-Brown D, Anderson S, et al. Comparison of 73. Oster JR , Epstein M, Smoller S. Combined therapy with thiazide-type
loop diuretics in patients with chronic renal insufficiency. Kidney Int 1987;
and loop diuretic agents for resistant sodium retention. Ann Intern Med
51. van Olden RW, van Meyel JJM, Gerlag PGG. Sensitivity of residual 74. Alexander WD, Branch RA, Levine DF, Hartog M. The urinary sodi-
nephrons to high dose furosemide described by diuretic efficiency. Eur J
um: potassium ratio and response to diuretics in resistant oedema. Postgrad
52. Rudy DW, Gehr TWB, Matzke GR , Kramer WG, Sica DA, Brater DC. 75. Van Vliet AA, Donker AJM, Nauta JJP, Verheugt FWA. Spironolac-
The pharmacodynamics of intravenous and oral torsemide in patients with
tone in congestive heart failure refractory to high-dose loop diuretic and
chronic renal insufficiency. Clin Pharmacol Ther 1994;56:39-47.
low-dose angiotensin-converting enzyme inhibitor. Am J Cardiol 1993;71:
53. Gallagher KL, Jones JK. Furosemide-induced ototoxicity. Ann Intern 76. Maren TH. Carbonic anhydrase inhibition. IX. Augmentation of the 54. Gerlag PGG, van Meijel JJM. High-dose furosemide in the treatment
renal effect of meralluride by acetazolamide. J Pharmacol Exp Ther 1958;
of refractory congestive heart failure. Arch Intern Med 1988;148:286-91. 55. Rudy DW, Voelker JR , Greene PK, Esparza FA, Brater DC. Loop di- 77. Rodicio JL, Hernando L. Effects and interactions of furosemide and
uretics for chronic renal insufficiency: a continuous infusion is more effica-
acetazolamide on tubular function in rat kidney. Rev Esp Fisiol 1977;33:
cious than bolus therapy. Ann Intern Med 1991;115:360-6. 56. Wollam GL, Tarazi RC, Bravo EL, Dustan HP. Diuretic potency of 78. Gibson DG, Marshall JC, Lockey E. Assessment of proximal tubular
combined hydrochlorothiazide and furosemide therapy in patients with
sodium reabsorption during water diuresis in patients with heart disease.
57. Fliser D, Schröter M, Neubeck M, Ritz E. Coadministration of thia- 79. Earley LE, Martino JA. Influence of sodium balance on the ability of
zides increases the efficacy of loop diuretics even in patients with advanced
diuretics to inhibit tubular reabsorption: a study of factors that influence
renal failure. Kidney Int 1994;46:482-8.
renal tubular sodium reabsorption in man. Circulation 1970;42:323-34. 58. Knauf H, Mutschler E. Diuretic effectiveness of hydrochlorothiazide 80. Brater DC, Kaojarern S, Chennavasin P. Pharmacodynamics of the di-
and furosemide alone and in combination in chronic renal failure. J Car-
uretic effects of aminophylline and acetazolamide alone and combined with
furosemide in normal subjects. J Pharmacol Exp Ther 1983;227:92-7. 59. Inoue M, Okajima K, Itoh K, et al. Mechanism of furosemide resist- 81. Szerlip HM. Renal-dose dopamine: fact and fiction. Ann Intern Med
ance in analbuminemic rats and hypoalbuminemic patients. Kidney Int
82. Denton MD, Chertow GM, Brady HR. “Renal-dose” dopamine for 60. Rane A, Villeneuve JP, Stone WJ, Nies AS, Wilkinson GR , Branch RA.
the treatment of acute renal failure: scientific rationale, experimental stud-
Plasma binding and disposition of furosemide in the nephrotic syndrome
ies and clinical trials. Kidney Int 1996;50:4-14.
and in uremia. Clin Pharmacol Ther 1978;24:199-207. 83. Chertow GM, Sayegh MH, Allgren RL, Lazarus JM. Is the adminis- 61. Keller E, Hoppe-Seyler G, Schollmeyer P. Disposition and diuretic ef-
tration of dopamine associated with adverse or favorable outcomes in acute
fect of furosemide in the nephrotic syndrome. Clin Pharmacol Ther 1982;
renal failure? Am J Med 1996;101:49-53. 84. Vargo DL, Brater DC, Rudy DW, Swan SK. Dopamine does not en- 62. Green TP, Mirkin BL. Resistance of proteinuric rats to furosemide:
hance furosemide-induced natriuresis in patients with congestive heart fail-
urinary drug protein binding as a determinant of drug effect. Life Sci 1980;
ure. J Am Soc Nephrol 1996;7:1032-7. 85. Warren SE, Blantz RC. Mannitol. Arch Intern Med 1981;141:493-7. 63. Idem. Furosemide disposition in normal and proteinuric rats: urinary 86. Borges HF, Hocks J, Kjellstrand CM. Mannitol intoxication in patients
drug-protein binding as a determinant of drug excretion. J Pharmacol Exp
with renal failure. Arch Intern Med 1982;142:63-6. 87. Sheffield PA, Turner JS. Ototoxic drugs: a review of clinical aspects, 64. Kirchner KA, Voelker JR , Brater DC. Intratubular albumin blunts the
histopathologic changes and mechanisms of action. South Med J 1971;64:
response to furosemide — a mechanism for diuretic resistance in the ne-
phrotic syndrome. J Pharmacol Exp Ther 1990;252:1097-101. 88. Cooperman LB, Rubin IL. Toxicity of ethacrynic acid and furosemide. 65. Idem. Binding inhibitors restore furosemide potency in tubule fluid
containing albumin. Kidney Int 1991;40:418-24. 89. Rose LI, Underwood RH, Newmark SR , Kisch ES, Williams GH. 66. Idem. Tubular resistance to furosemide contributes to the attenuated
Pathophysiology of spironolactone-induced gynecomastia. Ann Intern
diuretic response in nephrotic rats. J Am Soc Nephrol 1992;2:1201-7. 67. Nakahama H, Orita Y, Yamazaki M, et al. Pharmacokinetic and phar- 90. Brater DC. Drug-induced electrolyte disorders and use of diuretics.
macodynamic interactions between furosemide and hydrochlorothiazide in
In: Kokko JP, Tannen RL, eds. Fluids and electrolytes. 3rd ed. Philadelphia:
nephrotic patients. Nephron 1988;49:223-7. 68. Shear L, Ching S, Gabuzda GJ. Compartmentalization of ascites and 91. Chennavasin P, Seiwell R , Brater DC. Pharmacokinetic-dynamic anal-
edema in patients with hepatic cirrhosis. N Engl J Med 1970;282:1391-6.
ysis of the indomethacin-furosemide interaction in man. J Pharmacol Exp
69. Greither A, Goldman S, Edelen JS, Benet LZ, Cohn K. Pharmacoki-
netics of furosemide in patients with congestive heart failure. Pharmacology
92. Kaojarern S, Chennavasin P, Anderson S, Brater DC. Nephron site of
effect of nonsteroidal anti-inflammatory drugs on solute excretion in hu-
70. Andreasen F, Mikkelsen E. Distribution, elimination and effect of
mans. Am J Physiol 1983;244:F134-F139.
furosemide in normal subjects and in patients with heart failure. Eur J Clin
93. Waldorff S, Anderson JD, Heeboll-Nielsen N, et al. Spironolactone-
induced changes in digoxin kinetics. Clin Pharmacol Ther 1978;24:162-7.
Downloaded from www.nejm.org at HOUSTON ACADEMY OF MEDICINE on January 3, 2008 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
RISICO’s van GRIEP (uit de CEASE opleiding van Tinus Smits/2009) De ziekte De griep is een jaarlijks terugkerend verschijnsel in de winter. Het virus wordt overgedragen door speekseldruppeltjes bij het hoesten of niezen. Slechts de helft van de besmette personen wordt daadwerkelijk ziek. De incubatietijd is twee drie dagen, dan verschijnen koude rillingen, hoge koorts, een verkoudheid
call display) I hope I can be for her what she WELCOME NEW MEMBERS Beverly Hall , 51 Catharine Cres. Barb, Dianne, Sylvia and Mary Lou . They Their fiscal management was exceptional; Gillian Woan , 1059 West Black Lake Rd. they never used the funds set out for them in the budget. Organizing the programs, that take half of the meeting time, is a lot of work. Contacting speakers,
 D R U G T H E R A P Y
D R U G T H E R A P Y