Lowlevel laser (light) therapy (lllt) for treatment of hair loss
Lasers in Surgery and Medicine 9999:1 (2013)
Low-Level Laser (Light) Therapy (LLLT) for Treatment ofHair Loss
Pinar Avci, MD,1,2,3 Gaurav K. Gupta, MD, PhD,1,2 Jason Clark, MD,1,2 Norbert Wikonkal, MD, PhD,3and Michael R. Hamblin,
1Wellman Center for Photomedicine, Massachusetts General Hospital, Boston, Massachusetts 021142Department of Dermatology, Harvard Medical School, Boston, Massachusetts 021153Department of Dermatology, Venereology and Dermato-Oncology, Semmelweis University School of Medicine, Budapest1085, Hungary4Harvard-MIT Division of Health Sciences and Technology, Cambridge, Massachusetts 02139
Objective: Alopecia is a common disorder affecting more
wound healing, nerve regeneration, joint pain relief, stroke
than half of the population worldwide. Androgenetic
recovery, and the prevention and treatment of mucosi-
alopecia, the most common type, affects 50% of males
tis [2–8]. Home-use LLLT devices that emit low power
over the age of 40 and 75% of females over 65. Only two
coherent monochromatic red light have been developed for
drugs have been approved so far (minoxidil and finaste-
various skin conditions, including hair growth [9]. In this
ride) and hair transplant is the other treatment alterna-
review, we will focus on the use of LLLT as a potential
tive. This review surveys the evidence for low-level laser
treatment for several types of hair loss.
therapy (LLLT) applied to the scalp as a treatment for hairloss and discusses possible mechanisms of actions.
Methods and Materials: Searches of PubMed and Google
Hair is one of the fastest growing tissues of the human
Scholar were carried out using keywords alopecia, hair
body and the hair follicle, which is a unique characteristic
of mammals, represents a stem cell-rich, prototypic
Results: Studies have shown that LLLT stimulated hair
neuroectodermal–mesodermal interaction system [10].
growth in mice subjected to chemotherapy-induced alope-
Hair follicles undergo repetitive regenerative cycles and
cia and also in alopecia areata. Controlled clinical trials
each of these cycles consists of three stages: anagen (rapid
demonstrated that LLLT stimulated hair growth in both
growth, active stage), catagen (apoptosis-driven regres-
men and women. Among various mechanisms, the main
sion, physiological involution stage), and telogen (resting
mechanism is hypothesized to be stimulation of epidermal
stage) (Fig. 1) [10]. Bulge stem cells are found in the region
stem cells in the hair follicle bulge and shifting the follicles
of the outer root sheath located just below the sebaceous
gland, coinciding with the point of anchorage of the
Conclusion: LLLT for hair growth in both men and
arrector pili muscle [11]. During the telogen to anagen
women appears to be both safe and effective. The optimum
transition, there is a tightly controlled activation of these
wavelength, coherence and dosimetric parameters remain
epithelial bulge stem cells and within the same period,
to be determined. Lasers Surg. Med. 9999:1–8, 2013. ß
secondary hair germ cells give rise to transient amplifying
(TA) progeny cells [12]. Throughout the entire anagen
Key words: alopecia; androgenetic alopecia; hair loss;LLLT; low level laser (light)
Conflict of Interest Disclosures: All authors have completed
and submitted the ICMJE Form for Disclosure of Potential
Conflicts of Interest. Michael R. Hamblin is on the scientificadvisory board and holds stock in Transdermal Cap Inc. He has
It has long been known that red or near-infrared laser
been on the scientific advisory board and has received sponsoredresearch funding from Lexington Int. He has been an expert
light promotes tissue repair and regeneration and low-
witness for Advanced Hair Studio Australia. Other authors
intensity light called low-level laser therapy (LLLT)
stimulates cellular activity [1]. After the discovery of
Contract grant sponsor: US NIH; Contract grant number:
lasers in the 1960s, there has been tremendous interest in
ÃCorrespondence to: Michael R. Hamblin, PhD, Department of
using these laser devices to treat various medical
Dermatology, Harvard Medical School, BAR 414 Wellman,
conditions. The most commonly used devices have wave-
Center for Photomedicine, Massachusetts General Hospital, 40Blossom Street, Boston, MA 02114.
lengths in the range 500–1,100 nm (the so-called optical
window of tissue) and they deliver fluences of 1–10 J/cm2
with a power density of 3–90 mW/cm2. LLLT has shown
beneficial effects for a variety of medical conditions such as
Fig. 1. Stages of hair cycle. Anagen stage is the growth stage which may last 2–6 years. In cagatenstage, club hair transitions upwards towards the skin pore and the dermal papilla begins to separatefrom the follicle. This phase usually lasts from 1 to 2 weeks. In telogen stage, the dermal papilla fullyseparates from the follicle and it takes about 5–6 weeks. Lastly, the dermal papilla moves upward tomeet hair follicle once again and the hair matrix begins to form new hair, which represents thereturn to anagen stage.
phase, there is a robust proliferation of the TA cells within
involved in hair loss are not clearly known, some of the
the epithelial matrix of the hair follicle. Consequently,
proposed genes responsible for hair growth are desmoglein,
proliferating trichocytes terminally differentiate to form
activin, epidermal growth factor (EGF), fibroblast growth
the bulk of the hair filament which is the final product of
factor (FGF), lymphoid-enhancer factor-1 (LEF-1), and
the hair cycle. The dermal papilla of the hair follicle is
sonic hedgehog [15]. As of today, the most common methods
believed to be the key regulatory element in progenitor cell
used for treating AGA are topical minoxidil, finasteride
activation, hair matrix cell proliferation and terminal
(males only), and surgical hair transplantation [14].
differentiation of trichocytes [13].
Unfortunately, current therapies are not efficacious for
Androgenetic alopecia (AGA) is the most common form of
all patients with AGA. Medical therapies require indefinite
hair loss in men affecting almost 50% of the male
use and are limited by patient adherence; surgical options
population [14]. AGA refers to hair loss in genetically
(hair transplants) are limited by cost, each patient’s supply
susceptible individuals caused by effects of androgens such
of donor hair, and possible scarring in donor sites [18]. Due
as testosterone and its derivative dihydrotestosterone
to a need for more efficacious therapies, LLLT has emerged
(DHT). Testosterone is a lipophilic compound that diffuses
as a new therapeutic approach to treat AGA. The Hairmax
across the cell membrane. Testosterone is converted by the
Lasercomb1 was approved by the US Food and Drug
cytoplasmic enzyme 5-a reductase to DHT, which is its
Administration (FDA) and received 510 K clearance as a
more active form. There are two types of 5-a reductase;
safe therapy for the treatment of male AGA in 2007 and
Type 1 is found in keratinocytes, fibroblasts, sweat glands,
female AGA in 2011 [19]. There has been a recent
and sebocytes, and Type 2 is found in skin and the inner
review [20] on the use of lasers and light therapies for
root sheath of hair follicles [15]. DHT binds the nuclear
alopecia that covered 308 nm excimer laser, fractional
androgen receptor which regulates gene expression [15].
photothermolysis, and UV phototherapy, but did not cover
Disruption of epithelial progenitor cell activation and TA
LLLT mediated by red laser which is the main subject of the
cell proliferation due to abnormal androgen signaling forms
the essential pathophysiological component of this condi-
There are several other forms of hair loss such as
tion which in turn leads to continuous miniaturization of
alopecia areata (AA), telogen effluvium (TE), and chemo-
sensitive terminal hair follicles, and their conversion to
therapy-induced alopecia. AA is an autoimmune inflam-
vellus hair follicles [16,17]. Although the exact genes
matory condition, which presents with non-scarring
alopecia and is characterized on histology by intra- or peri-
LLLT for Hair Regrowth, Proposed Mechanisms
follicular lymphocytic infiltrates composed of CD4þ and
As previously mentioned, in 2007 and 2011, LLLT
CD8þ T-cells [19]. There are severe variants of AA:
mediated by a laser comb was approved by the FDA as a
alopecia totalis, a total loss of scalp hair and alopecia
safe treatment for male and female pattern hair loss
universalis, total loss of scalp and body hair [21]. The most
respectively [19]. Laser phototherapy is assumed to
common treatment modality is intralesional corticosteroid
stimulate anagen re-entry in telogen hair follicles, prolong
injections; however, other treatments include topical and
duration of anagen phase, increase rates of proliferation in
systemic corticosteroids, minoxidil, anthralin, contact
active anagen hair follicles and to prevent premature
sensitizers, psoralen plus ultraviolet A, cyclosporine,
catagen development [19,30]. The exact mechanism of
tacrolimus, and biologics such as alefacept, efalizumab,
action of LLLT in hair growth is not known; however,
etanercept, infliximab, and adalimumab [15]. TE is
several mechanisms have been proposed. Evidence sug-
abnormal hair cycling causing excessive loss of telogen
gests that LLLT acts on the mitochondria and may alter
hair [15]. Some common causes include acute severe
cell metabolism through photodissociation of inhibitory
illness, surgery, iron deficient anemia, thyroid disease,
nitric oxide (NO) from cytochrome c oxidase (CCO) [31]
malnutrition, chronic illness, and medications such as oral
(Unit IV in the respiratory chain of mitochondria), causing
contraceptives, lithium, and cimetidine. Chemotherapy
increased ATP production, modulation of reactive oxygen
works by destroying rapidly dividing cancer cells, however,
species, and induction of transcription factors such as
at the same time, other rapidly dividing cells of the body
nuclear factor kappa B, and hypoxia-inducible factor-1
such as hair follicles are also destroyed, and this unwanted
[32]. These transcription factors in return cause protein
effect leads to chemotherapy-induced alopecia starting 1–3
synthesis that triggers further effects down-stream, such
weeks and peaking at 1–2 months of treatment [22].
as increased cell proliferation and migration, alteration inthe levels of cytokines, growth factors and inflammatory
LLLT for Prevention and Reversal of Hair Loss
mediators, and increased tissue oxygenation [32]. More-
In the late 1960s, Endre Mester, a Hungarian physician,
over, NO is known to be a potent vasodilator via its effect on
began a series of experiments on the carcinogenic potential
cyclic guanine monophosphate production and it can be
of lasers by using a low-power ruby laser (694 nm) on mice.
speculated that LLLT may cause photodissociation of NO
Mice were shaved as a part of the experimental protocol. To
not only from CCO but also from intracellular stores such
Mester’s surprise, the laser did not cause cancer but
as nitrosylated forms of both hemoglobin and myoglobin
instead improved hair growth around the shaved region on
leading to vasodilation and increased blood flow which was
the animal’s back [23]. This was the first demonstration of
reported in several studies [32–34]. Yamazaki and co-
“photobiostimulation” with LLLT, and it opened a new
workers observed an upregulation of hepatocyte growth
factor (HGF) and HGF activator expression following
Recently, attention has been drawn towards an uncom-
irradiation of the backs of Sprague Dawley rats with linear
mon but striking adverse effect of lasers being used for hair
removal. It has been noticed in some cases that, increase in
Some authors have drawn comparisons between the
hair density, color or coarseness or a combination of these
mechanism of action of LLLT and the mechanism of
occurs at or around sites treated for hair removal [19,25–
minoxidil. Even though the mechanism by which minoxidil
27]. The name given for this phenomenon is “Paradoxical
promotes hair growth is not fully understood, it is known
Hypertrichosis” and the incidence varies from 0.6% to 10%
that minoxidil contains an N-oxide group which may be
[19]. A group of researchers also observed transformation
able to release NO, which is an important cellular
of small vellus hairs into larger terminal hairs upon low
signaling molecule involved in many physiological and
fluence diode laser treatment and named this phenomenon
pathological processes [36] and is also a vasodilator [37].
“terminalization” of vellus hair follicles [28,29]. Until
Furthermore, minoxidil is an ATP sensitive Kþ channel
today, different mechanisms have been proposed to explain
opener which in turn cause hyperpolarization of cell
paradoxical hypertrichosis. In one study, this was attrib-
membranes [38]. Since ATP sensitive Kþ channels in
uted to presence of polycystic ovarian syndrome in 5 out of
mitochondria and increased levels of NO [39–41] may have
49 females undergoing IPL laser treatment for facial
some role to play in effects of LLLT in brain and heart [41–
hirsutism [27]. Another group of researchers suggested
43], given what is known about the role of K-ATP channels
that although the heat produced by the laser is less than
and NO in hair regrowth mediated by minoxidil, a
the temperature necessary for thermolysis of the hair
mechanistic overlap can be identified. Weiss and co-
follicle, this heat may be sufficient to induce follicular stem
workers, by using RT-PCR and microarray analysis,
cell proliferation and differentiation by increasing the level
demonstrated that depending on the treatment param-
of heat shock proteins (HSPs) such as HSP27, which plays
eters, LLLT modulates 5-a reductase expression, which
a role in regulation of cell growth and differentiation [19].
converts testosterone into DHT, alters vascular endotheli-
Sub-therapeutic injury caused by the laser could also
al growth factor gene expression as wells as matrix
result in the release of certain factors which could
metalloproteinase (MMP-2) which have significant roles
potentially induce follicular angiogenesis and affect the
in hair follicle growth, and in turn the group reported
stimulation of hair growth on human dermal papillae cells
[44–47]. Notably, similar changes have also been reported
that laser irradiation prolongs the anagen phase [50,51].
with topical minoxidil use [47]. Furthermore, LLLT has
Furthermore, in testosterone-treated and He–Ne (1 J/cm2)
been demonstrated to modulate inflammatory processes
irradiated skin, hair follicles were seen to originate from
and immunological responses, which may also have an
the middle of the dermis, and these follicles represent early
effect in hair regrowth [32,48]. A study conducted by
anagen phase [49]. Based on this observation, it may be
Wikramanayake et al. [19] on C3H/HeJ mouse model of AA
proposed that the majority of catagen and telogen follicles
supported this assumption wherein the mice treated with
re-enter into anagen phase as a result of low-level laser
laser comb, increased number of hair follicles with majority
in anagen phase were noted with decreased inflammatory
The incidence of alopecia related to cancer treatments
infiltrates. Considering that inflammatory infiltrates are
such as chemotherapy is close to 65% and it has severe
highly disruptive to hair follicle biology and multiple
negative psychological effects [22]. LLLT has been sug-
cytokines such as IFN-g, IL-1a and b, TNF-a, MHC and
gested as a treatment modality to promote hair regrowth
Fas-antigen and macrophage migration inhibitory factor
for chemotherapy-induced alopecia. In a rat model, differ-
are all involved in the cyclic hair growth and have been
ent regimens of chemotherapy were given to each rat in
shown to play a role in the pathogenesis of AA, modulatory
conjunction with an LLLT device which had the laser unit
effects of LLLT on inflammation might have a significant
and switch from the HairMax LaserComb1, but without
the comb or handle [52]. Hair regrowth occurred 5 daysearlier in all laser treated rats when compared to control
and sham-treated rats. Histology results demonstrated
Wikramanayake et al. [19] demonstrated the hair
large anagen hair bulbs penetrating deeper into the
growth effects of LLLT on C3H/HeJ mouse model of AA,
subcutaneous adipose tissue in LLLT-treated skin. Fur-
using HairMax Laser Comb1 (emits nine beams and
thermore, it did not compromise the efficacy of chemother-
attached combs help to part the hairs and improve delivery
apy by causing localized protection of the cancer cells [52].
of laser light to scalp), 655 nm for 20 seconds daily threetimes per week for a total of 6 weeks [19]. At the end of the
treatment, hair regrowth was observed in all the laser
In order to test the effect of linear polarized infrared
treated mice but no difference was observed in the sham-
irradiation in treatment of AA, a study was conducted
treated group (control group undergoing similar treatment
with 15 patients (6 men, 9 women) using Super LizerTM, a
procedures without administration of the key therapeutic
medical instrument emitting polarized pulsed linear light
element, such as application of light that has no
with a high output (1.8 W) of infrared radiation (600–
therapeutic effect) [19]. On histology, while an increased
1,600 nm) that is capable of penetrating into deep
number of anagen hair follicles was observed in laser-
subcutaneous tissue [53]. The scalp was irradiated for
treated mice, sham-treated mice demonstrated telogen
3 minutes either once every week or once every other week
follicles with absent hair shafts [19].
until vellus hair regrowth in at least 50% of the affected
Shukla et al. [49] investigated the effect of helium–neon
area was observed. Additionally, carpronium chloride 5%
(He–Ne) laser (632 nm, at doses of 1 and 5 J/cm2 at 24-hour
was applied topically twice daily to all the lesions in
intervals for 5 days) on the hair follicle growth cycle of
combination with oral antihistamines, cepharanthin and
testosterone-treated and un-treated Swiss albino mice
glycyrrhizin (extracts of Chinese medicine herbs) [53]. As
skin. Testosterone treatment led to the inhibition of hair
a result of this study, in 47% of the patients’ hair growth
growth which was characterized by a significant increase
occurred 1.6 months earlier in irradiated areas than in
in catagen follicles [49].The results showed that exposure
non-irradiated areas [53]. However, 1 year after irradia-
of testosterone treated mice to the He–Ne laser at a dose of
tion, all the lesions disappeared; hair density, length and
1 J/cm2 led to significant increase in the number of hair
diameter of hair shafts were the same both in irradiated
follicles in anagen phase when compared to the other
and non-irradiated lesions; suggesting that LLLT only
groups. However, the 5 J/cm2 treated group showed a
accelerates the process of hair regrowth in AA patients. It
significant decrease in the number of anagen hair and an
is worth mentioning that the method for assessment of
increase in telogen hair follicles. This is consistent with the
hair regrowth, density and thickness was not clearly
biphasic effect of LLLT wherein low irradiation doses may
stated, which was one of the main limitations of this
cause biostimulation and high irradiation doses may cause
inhibition [32,49]. Since hair growth promoting effect of
Using 655 nm red light and 780 nm infrared light once
He–Ne laser (1 J/cm2) was much higher for the testoster-
a day for 10 minutes, 24 male AGA patients were treated
one-treated mice than the non-testosterone treated mice, it
and evaluated by a group of investigators [54]. Evalua-
can be suggested that cells growing at slower rate or under
tion has been performed via global photography and
stress conditions respond better to the stimulatory effects
phototrichogram [54]. Following 14 weeks of treatment,
of LLLT. Another notable observation in this study is that
increase in hair density on both the vertex (145.1/cm2 vs.
in He–Ne laser (1 J/cm2) irradiated skin, some of the
137.3/cm2 pre-treatment, P < 0.005) and occiput (163.3/
anagen follicles appeared from deeper layers of the skin
cm2 vs. 153.3/cm2, P < 0.005) as well as anogen/telogen
and possessed a different orientation which both represent
ratio (vertex: 84.7 vs. 79.7 pre-treatment and occiput:
the late anagen stage in the hair cycle that in turn suggests
91.9 vs. 89.6 pre-treatment) was observed, and 83% of
the patients reported to be satisfied with the treatment
patients. Each patient was given a HairMax LaserComb1
655 nm, to use at home for 6 months for 5–10 minutes every
Satino et al. [55] tested the efficacy of LLLT on hair
other day [55]. Tensile strength was measured by VIP
growth and tensile strength on 28 male and 7 female AGA
HairOSCope (Belson Imports, Hialeah, FL) through
TABLE 1. Summary of the Studies That Investigated the Efficacy of LLLT for Hair Growth
655 nm, 5–10 minutesevery other day, for 6
removal of three typical terminal hairs from a one square
centimeter area. Hair count was performed within one
LLLT was discovered serendipitously in the 1960s when
centimeter square space created within a mold that was
mice irradiated with a low fluence red laser grew hair.
prepared around the area of greatest alopecia. A surgical
Since that time LLLT has demonstrated promise in
hook and magnification has been used while counting the
conditions from wound healing to stroke recovery, from
number of hair. In terms of hair tensile strength, the
treatment of musculoskeletal pain to prevention of
results revealed greater improvement in the vertex area
mucositis. Animal and human data have slowly accumu-
for males and temporal area for females; however, both
lated supporting LLLT for hair growth (Table 1). LLLT
sexes benefited in all areas significantly [55]. In terms of
appears to improve a variety of non-scarring alopecias—
hair count, both sexes and all areas had substantial
AGA, AA, and chemotherapy-induced alopecia. Based on
improvement (for temporal area: 55% in women, 74% in
the studies demonstrating LLLT’s effects on promoting
men, in vertex area: 65% in women, 120% in men) with
graft survival, it may be further suggested to have a
vertex area in males having the best outcome [55]. The
potential to be used during the immediate period of post-
HairMax LaserComb1 device was tested by Leavitt et al.
hair transplant surgery to facilitate the healing process
in a double-blind, sham device-controlled, multicenter, 26-
and enhance viability and earlier growth of the grafts
week trial randomized study among 110 male AGA
[60,61]. While mechanisms are still emerging, LLLT may
patients [30]. Patients used the device three times per
increase anagen hairs through release of NO from CCO by
week for 15 minutes for a total of 26 weeks [30].
photodissociation and LLLT may reduce inflammation in
Significantly greater increase in mean terminal hair
AA. However, more studies are needed to optimize
density compared to subjects in the sham device group
treatment parameters and determine long-term efficacy
has been reported [30]. Significant improvements in
as well as safety of emerging LLLT technologies. Most
overall hair regrowth, slowing of hair loss, thicker feeling
studies investigating effects of LLLT on hair growth have
hair, better scalp health and hair shine were also
used wavelengths that range from 635 to 650 nm, but as of
demonstrated in terms of patients’ subjective assessment
today no study has compared the effect of near-infrared
wavelengths such as 810 nm, which have deeper penetrat-
Recently, a double-blind randomized controlled trial by
ing capacities, to red light. Moreover, further studies are
Lanzafame et al. [56] using a helmet containing 21, 5 mW
required to compare efficacy of different light sources
lasers and 30 LEDs (655 Æ 5 nm, 67.3 J/cm2, 25 minutes
(continuous vs. pulsed) and methods of light delivery (laser
treatment) every other day for 16 weeks reported 35%
increase in hair growth among male AGA patients. Another recent study by Kim et al. [57] designed a 24
weeks randomized, double-blind, sham device-controlled
Research in the Hamblin Laboratory is supported by US
multicenter trial among both male and female AGA
patients in order to investigate the efficacy of a helmettype LLLT device combining 650 nm laser with 630 and
1. Schindl A, Schindl M, Pernerstorfer-Schon H, Schindl L. Low-
47.90 J/cm2 for 18 minutes). Even though mean hair
intensity laser therapy: A review. J Investig Med 2000;48
thickness (12.6 Æ 9.4 vs. 3.9 Æ 7.3 in control group,
P ¼ 0.01) and hair density (17.2 Æ 12.1 vs. À2.1 Æ 18.3 in
2. Bjordal JM, Couppe C, Chow RT, Tuner J, Ljunggren EA. A
control group, P ¼ .003) increased significantly in the
systematic review of low level laser therapy with location-specific doses for pain from chronic joint disorders. Aust J
treatment group, there was no prominent difference in
global appearance between the two groups [57]. Findings
3. Brosseau L, Welch V, Wells G, deBie R, Gam A, Harman K,
from a different study by Avram and Rogers [58] were in
Morin M, Shea B, Tugwell P. Low level laser therapy (classesI, II and III) in the treatment of rheumatoid arthritis.
accordance with these results where LLLT increased hair
Cochrane Database Syst Rev 2000; (2):CD002049.
count and shaft diameter, however, blinded global images
4. Cauwels RG, Martens LC. Low level laser therapy in oral
mucositis: A pilot study. Eur Arch Paediatr Dent 2011;12(2):118–123.
5. Christie A, Jamtvedt G, Dahm KT, Moe RH, Haavardsholm
EA, Hagen KB. Effectiveness of nonpharmacological and
LLLT has demonstrated a remarkably low incidence of
nonsurgical interventions for patients with rheumatoid
adverse effects when it has been used over 50 years for
arthritis: An overview of systematic reviews. Phys Ther2007;87(12):1697–1715.
diverse medical conditions and in a variety of anatomical
6. Jamtvedt G, Dahm KT, Holm I, Flottorp S. Measuring
sites. In the specific area of LLLT for hair growth, the only
physiotherapy performance in patients with osteoarthritis of
adverse reports in humans, was the temporary onset of TE
the knee: A prospective study. BMC Health Serv Res2008;8:145.
developing in the first 1–2 months after commencing
7. Schubert MM, Eduardo FP, Guthrie KA, Franquin JC,
LaserComb treatment [55], but disappearing on continued
Bensadoun RJ, Migliorati CA, Lloid CM, Eduardo CP, Walter
application. Some other possible considerations are pres-
NF, Marques MM, Hamdi M. A phase III randomized double-
ence of dysplastic or malignant lesions on the scalp which
blind placebo-controlled clinical trial to determine the efficacyof low level laser therapy for the prevention of oral mucositis
could be stimulated to grow by proliferative effects of LLLT
in patients undergoing hematopoietic cell transplantation.
Support Care Cancer 2007;15(10):1145–1154.
8. Silva GB, Mendonca EF, Bariani C, Antunes HS, Silva MA.
33. Lohr NL, Keszler A, Pratt P, Bienengraber M, Warltier DC,
The prevention of induced oral mucositis with low-level laser
Hogg N. Enhancement of nitric oxide release from nitrosyl
therapy in bone marrow transplantation patients: A random-
hemoglobin and nitrosyl myoglobin by red/near infrared
ized clinical trial. Photomed Laser Surg 2011;29(1):27–31.
radiation: Potential role in cardioprotection. J Mol Cell
9. Metelitsa AI, Green JB. Home-use laser and light devices for
the skin: An update. Semin Cutan Med Surg 2011;30(3):144–
34. Makihara E, Masumi S. Blood flow changes of a superficial
temporal artery before and after low-level laser irradiation
10. Paus R, Foitzik K. In search of the “hair cycle clock”: A guided
applied to the temporomandibular joint area. Nihon Hotetsu
tour. Differentiation 2004;72(9–10):489–511.
Shika Gakkai Zasshi 2008;52(2):167–170.
11. Braun KM, Niemann C, Jensen UB, Sundberg JP, Silva-
35. Miura Y, Yamazaki M, Tsuboi R, Ogawa H. Promotion of rat
Vargas V, Watt FM. Manipulation of stem cell proliferation
hair growth by irradiation using Super LizerTM. Jpn J
and lineage commitment: Visualisation of label-retaining
cells in wholemounts of mouse epidermis. Development
36. Hou YC, Janczuk A, Wang PG. Current trends in the
development of nitric oxide donors. Curr Pharm Des 1999;5
12. Tiede S, Kloepper JE, Bodo E, Tiwari S, Kruse C, Paus R. Hair
follicle stem cells: Walking the maze. Eur J Cell Biol 2007;86
37. Proctor PH. Endothelium-derived relaxing factor and minox-
idil: Active mechanisms in hair growth. Arch Dermatol
13. Plikus MV, Sundberg JP, Chuong CM. Mouse skin ectodermal
organs. In: Fox J BS, Davisson M, editors. The mouse in
38. Rossi A, Cantisani C, Melis L, Iorio A, Scali E, Calvieri S.
biomedical research. New York: Academic Press; 2006. pp.
Minoxidil use in dermatology, side effects and recent patents.
Recent Pat Inflamm Allergy Drug Discov 2012;6(2):130–136.
14. Otberg N, Finner AM, Shapiro J. Androgenetic alopecia.
39. Karu TI, Pyatibrat LV, Afanasyeva NI. Cellular effects of low
Endocrinol Metab Clin North Am 2007;36(2):379–398.
power laser therapy can be mediated by nitric oxide. Lasers
15. Ghanaat M. Types of hair loss and treatment options,
including the novel low-level light therapy and its proposed
40. Tuby H, Maltz L, Oron U. Modulations of VEGF and iNOS in
mechanism. South Med J 2010;103(9):917–921.
the rat heart by low level laser therapy are associated with
16. Itami S, Inui S. Role of androgen in mesenchymal epithelial
cardioprotection and enhanced angiogenesis. Lasers Surg
interactions in human hair follicle. J Investig Dermatol Symp
41. Karu TI. Mitochondrial signaling in mammalian cells
17. Hoffmann R, Happle R. Current understanding of androge-
activated by red and near-IR radiation. Photochem Photobiol
netic alopecia. Part I: Etiopathogenesis. Eur J Dermatol
42. Karu TI, Pyatibrat LV, Afanasyeva NI. A novel mitochondrial
18. Rogers NE, Avram MR. Medical treatments for male and
signaling pathway activated by visible-to-near infrared
female pattern hair loss. J Am Acad Dermatol 2008;59(4):547–
radiation. Photochem Photobiol 2004;80(2):366–372.
43. Ignatov YD, Vislobokov AI, Vlasov TD, Kolpakova ME,
19. Wikramanayake TC, Rodriguez R, Choudhary S, Mauro LM,
Mel’nikov KN, Petrishchev IN. Effects of helium-neon laser
Nouri K, Schachner LA, Jimenez JJ. Effects of the Lexington
irradiation and local anesthetics on potassium channels in
LaserComb on hair regrowth in the C3H/HeJ mouse model of
pond snail neurons. Neurosci Behav Physiol 2005;35:871–
alopecia areata. Lasers Med Sci 2012;27(2):431–436.
20. Rangwala S, Rashid RM. Alopecia: A review of laser and light
44. Castex-Rizzi N, Lachgar S, Charveron M, Gall Y. Implication
therapies. Dermatol Online J 2012;18(2):3.
of VEGF, steroid hormones and neuropeptides in hair follicle
21. Wasserman D, Guzman-Sanchez DA, Scott K, McMichael A.
cell responses. Ann Dermatol Venereol 2002;129(5 Pt 2):783–
Alopecia areata. Int J Dermatol 2007;46(2):121–131.
22. Trueb RM. Chemotherapy-induced alopecia. Semin Cutan
45. Weiss R, McDaniel DH, Geronemus RG, Weiss M. LED
photomodulation induced hair growth stimulation 2005;36
23. Mester E, Ludany G, Sellyei M, Szende B, Gyenes G, Tota GJ.
Studies on the inhibiting and activating effects of laser beams.
46. Yano K, Brown LF, Detmar M. Control of hair growth and
Langenbecks Arch Chir 1968;322:1022–1027.
follicle size by VEGF-mediated angiogenesis. J Clin Invest
24. Barolet D. Light-emitting diodes (LEDs) in dermatology.
Semin Cutan Med Surg 2008;27(4):227–238.
47. Yamazaki M, Tsuboi R, Lee YR, Ishidoh K, Mitsui S, Ogawa
25. Vlachos SP, Kontoes PP. Development of terminal hair
H. Hair cycle-dependent expression of hepatocyte growth
following skin lesion treatments with an intense pulsed light
factor (HGF) activator, other proteinases, and proteinase
source. Aesthetic Plast Surg 2002;26(4):303–307.
inhibitors correlates with the expression of HGF in rat hair
26. Moreno-Arias GA, Castelo-Branco C, Ferrando J. Side-effects
follicles. J Investig Dermatol Symp Proc 1999;4(3):312–315.
after IPL photodepilation. Dermatol Surg 2002;28(12):1131–
48. Meneguzzo DT, Lopes LA, Pallota R, Soares-Ferreira L,
Lopes-Martins RA, Ribeiro MS. Prevention and treatment of
27. Moreno-Arias G, Castelo-Branco C, Ferrando J. Paradoxical
mice paw edema by near-infrared low-level laser therapy on
effect after IPL photoepilation. Dermatol Surg 2002;28
lymph nodes. Lasers Med Sci 2013;28(3):973–980.
49. Shukla S, Sahu K, Verma Y, Rao KD, Dube A, Gupta PK.
28. Bernstein EF. Hair growth induced by diode laser treatment.
Effect of helium-neon laser irradiation on hair follicle growth
cycle of Swiss albino mice. Skin Pharmacol Physiol 2010;23
29. Bouzari N, Firooz AR. Lasers may induce terminal hair
growth. Dermatol Surg 2006;32(3):460.
50. Muller-Rover S, Handjiski B, van der Veen C, Eichmuller S,
30. Leavitt M, Charles G, Heyman E, Michaels D. HairMax
Foitzik K, McKay IA, Stenn KS, Paus R. A comprehensive
LaserComb laser phototherapy device in the treatment of
guide for the accurate classification of murine hair follicles in
male androgenetic alopecia: A randomized, double-blind,
distinct hair cycle stages. J Invest Dermatol 2001;117(1):3–
sham device-controlled, multicentre trial. Clin Drug Investig
51. Philp D, Nguyen M, Scheremeta B, St-Surin S, Villa AM,
31. Eells JT, Wong-Riley MT, VerHoeve J, Henry M, Buchman
Orgel A, Kleinman HK, Elkin M. Thymosin beta4 increases
EV, Kane MP, Gould LJ, Das R, Jett M, Hodgson BD, Margolis
hair growth by activation of hair follicle stem cells. FASEB J
D, Whelan HT. Mitochondrial signal transduction in acceler-
ated wound and retinal healing by near-infrared light
52. Wikramanayake TC, Villasante AC, Mauro LM, Nouri K,
therapy. Mitochondrion 2004;4(5–6):559–567.
Schachner LA, Perez CI, Jimenez JJ. Low-level laser
32. Chung H, Dai T, Sharma SK, Huang YY, Carroll JD, Hamblin
treatment accelerated hair regrowth in a rat model of
MR. The nuts and bolts of low-level laser (light) therapy. Ann
chemotherapy-induced alopecia (CIA). Lasers Med Sci
53. Yamazaki M, Miura Y, Tsuboi R, Ogawa H. Linear polarized
57. Kim H, Choi JW, Kim JY, Shin JW, Lee SJ, Huh CH. Low-
infrared irradiation using Super Lizer is an effective
level light therapy for androgenetic alopecia: A 24-week,
treatment for multiple-type alopecia areata. Int J Dermatol
randomized, double-blind. Sham Device-Controlled Multicen-
ter Trial. Dermatol Surg 2013;39(8):1177–1183.
54. Kim SS, Park MW, Lee CJ. Phototherapy of androgenetic
58. Avram MR, Rogers NE. The use of low-level light for hair
alopecia with low level narrow band 655-nm red light and
growth: Part I. J Cosmetic Laser Ther 2009;11(2):110–117.
780-nm infrared light. J Am Acad Dermatolog. 2007;56:
59. Frigo L, Luppi JS, Favero GM, Maria DA, Penna SC, Bjordal
AB112. American Academy of Dermatology 65th Annual
JM, Bensadoun RJ, Lopes-Martins RA. The effect of low-level
laser irradiation (In-Ga–Al–AsP—660 nm) on melanoma in
55. Satino JL, Markou M. Hair regrowth and increased hair
vitro, in vivo. BMC Cancer 2009;9:404.
tensile strength using the HairMax LaserComb for Low-
60. Pinfildi CE, Hochman BS, Nishioka MA, Sheliga TR, Neves
Level Laser Therapy. Int J Cos Surg Aest Dermatol
MA, Liebano RE, Ferreira LM. What is better in TRAM flap
survival: LLLT single or multi-irradiation? Lasers Med Sci
56. Lanzafame R, Blanche R, Bodian A, Chiacchierini R,
Fenandez-Obregon A, Kazmirek E, Raymond J. The growth
61. Prado RP, Garcia SB, Thomazini JA, Piccinato CE. Effects of
of human scalp hair mediated by visible red light laser and
830 and 670 nm laser on viability of random skin flap in rats.
LED sources in males. Lasers Surg Med 2013;45: (S25):12.
Photomed Laser Surg 2012;30(8):418–424.
Laplink Software, Inc. License Agreement BY INSTALLING THE SOFTWARE, YOU ACKNOWLEDGE THAT YOU HAVE READ THIS AGREEMENT, UNDERSTAND IT AND AGREE TO BE BOUND BY ITS TERMS AND CONDITIONS. YOU FURTHER AGREE THAT IT IS THE COMPLETE AND EXCLUSIVE STATEMENT OF THE AGREEMENT BETWEEN US AND SUPERSEDES ANY PROPOSAL OR PRIOR AGREEMENT, BOTH ORAL OR WRITTEN, AND ANY OTHER COMMUNICATIONS BETWEEN US RELATING TO
Dear Sir We read with interest the article ‘HotMoreover, the type of headache that they describebath-related headache controlled by topiramate’ byin their patient following a hot bath also seems toLee et al. (1) and wish to comment on some omis-have some features of migraine in terms of sever-sions in their article and also seek their response toity, throbbing nature, and the presence
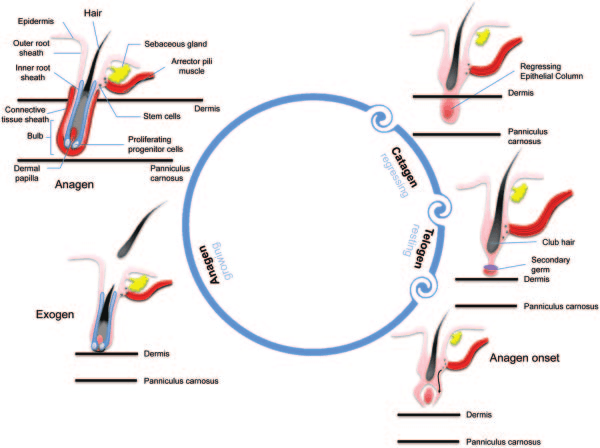 Fig. 1. Stages of hair cycle. Anagen stage is the growth stage which may last 2–6 years. In cagatenstage, club hair transitions upwards towards the skin pore and the dermal papilla begins to separatefrom the follicle. This phase usually lasts from 1 to 2 weeks. In telogen stage, the dermal papilla fullyseparates from the follicle and it takes about 5–6 weeks. Lastly, the dermal papilla moves upward tomeet hair follicle once again and the hair matrix begins to form new hair, which represents thereturn to anagen stage.
Fig. 1. Stages of hair cycle. Anagen stage is the growth stage which may last 2–6 years. In cagatenstage, club hair transitions upwards towards the skin pore and the dermal papilla begins to separatefrom the follicle. This phase usually lasts from 1 to 2 weeks. In telogen stage, the dermal papilla fullyseparates from the follicle and it takes about 5–6 weeks. Lastly, the dermal papilla moves upward tomeet hair follicle once again and the hair matrix begins to form new hair, which represents thereturn to anagen stage.