PLEASE FILL OUT THIS FORM COMPLETELY SO WE CAN HELP YOU WITH YOUR PAINFUL CONDITION. NAME:_____________________________ AGE:_____ HEIGHT ___'___"WEIGHT______lbs OCCUPATION:__________________________________________ DATE LAST WORKED____/____/____ CC: WHY WERE YOU REFERRED TO OUR CLINIC?______________________________________________________
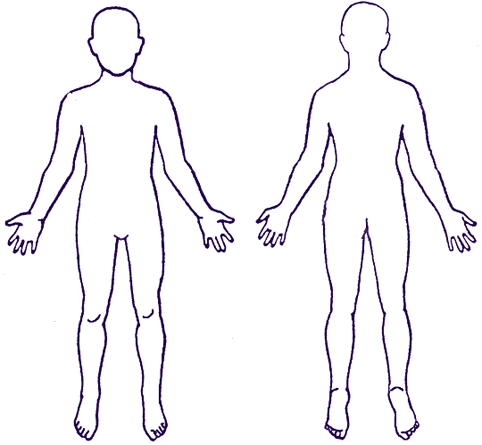
PLEASE DESCRIBE YOUR PAIN BY SHADING IN THE AFFECTED AREAS AND PLACING AN 'X' ON THE
AREA THAT HURTS THE MOST. CIRCLE ALL APPLICABLE DESCRIPTIVE WORDS.
PLEASE ATTEMPT TO QUANTIFY YOUR PAIN USING PERCENTAGES. YOUR TOTAL PAIN SHOULD ADD UP TO 100%. ( EXAMPLE: 20% LOW BACK PAIN AND 80% RIGHT LEG PAIN = 100%.) HEAD_____% NECK_____% RIGHT ARM_____% LEFT ARM_____%
LOWER BACK_____% HIPS/BUTTOCKS_____% RIGHT LEG_____% LEFT LEG_____%
CIRCLE THE ACTIVITIES WHICH TEND TO INCREASE YOUR PAIN: WALKING TWISTING STANDING
FILL IN ACTIVITIES WHICH DECREASE YOUR PAIN:__________________________________________________________
DOES THIS PAIN AFFECT YOUR SLEEP? YES / NO CURRENT PAIN MEDICATIONS:_________________________________________PRESCRIBED BY DR._________________ MARK YOUR AVERAGE PAIN SCORE: 0-----------1-----------2-----------3-----------4-----------5-----------6-----------7-----------8-----------9-----------10 MARK YOUR WORST PAIN SCORE: 0-----------1-----------2-----------3-----------4-----------5-----------6-----------7-----------8-----------9-----------10 NOTE: (ZERO EQUALS NO PAIN AND TEN EQUALS YOUR WORST IMAGINABLE PAIN) WHEN DID THIS PAIN BEGIN?_________ (SPONTANEOUS/ INJURY/ ACCIDENT/ SURGERY/ OTHER) PLEASE DESCRIBEHOW IT BEGAN: __________________________________________________________________________________________________________ __________________________________________________________________________________________________________ __________________________________________________________________________________________________________ __________________________________________________________________________________________________________ HAVE YOU EVER HAD ANY ACCIDENTS OR INJURIES AFFECTING THESE SAME AREAS BEFORE? YES / NO IF YES, WHEN?__________________________________________________________________________________________ TREATMENT: WHICH TYPES OF TREATMENT HAVE YOU HAD IN THE PAST TO TREAT YOUR CURRENT PAIN.
PLEASE CIRCLE ALL THAT APPLY.
PAIN CLINIC PHYSICAL THERAPY MASSAGE CHIROPRACTIC INJECTIONS SURGERY ACUPUNCTURE MAGNETS HERBS OTHER:_______________________________________________________ PLEASE LIST ALL TREATMENT BELOW: HEALTH CARE APPROXIMATEDIAGNOSIS TREATMENT/ PROFESSIONALDATES MEDICATIONS
DIAGNOSTIC EXAMINATIONS:
PLEASE CIRCLE ALL THAT APPLY
XRAY CT-SCAN MRI MYELOGRAM EMG/NCV OTHER___________________________________________________ PAST/CURRENT MEDICAL HISTORY:
PLEASE CIRCLE ALL THAT APPLY:
ARTHRITIS ASTHMA BLEEDING PROBLEMS CANCER CIRRHOSIS COLITIS DIABETES EMPHYSEMA HEART TROUBLE HEPATITIS / JAUNDICE HIGH BLOOD PRESSURE HIV / AIDS KIDNEY DISEASE MURMUR SEIZURE STROKE THYROID TROUBLE URINATING ULCER VASCULAR DISEASE ARE YOU TAKING ANY BLOOD THINNERS SUCH AS COUMADIN, WARFARIN, PLAVIX, OR TICLID? YES / NO LIST ALL CURRENT MEDICATIONS:________________________________________________________________________ ALLERGIES TO MEDICATIONS:_____________________________________________________________________________ PAST SURGICAL HISTORY: (PLEASE LISTALL OPERATIONS YOU HAVE HAD)________________________________ __________________________________________________________________________________________________________ SH:SINGLE____ MARRIED____ DIVORCED____ SEPARATED____ WIDOWED____ # OF CHILDREN_____ PACKS OF CIGARETTES SMOKED/DAY_________
# OF ALCOHOLIC BEVERAGES/DAY_________
HISTORY OF SUBSTANCE ABUSEYES / NO IF YES, WHAT TYPE?_____________________________________________
FH:LIST ANY ILLNESSES WHICH RUN IN YOUR FAMILY: ___________________________________________________ ROS: PLEASE CIRCLE ALL SYMPTOMS YOU MAY CURRENTLY HAVE: CHANGE IN VISION CHEST PAIN COUGH DIARRHEA / CONSTIPATION DIZZINESS EASY BLEEDING FAINTING FEVER ITCHING SHORTNESS OF BREATH STOMACH PROBLEMS URINARY PROBLEMS WEIGHT LOSS / WEIGHT GAIN WHO IS YOUR CURRENT PRIMARY CARE PHYSICIAN / PROVIDER:__________________________________________
Using Your Benesyst Benny™! Over-The-Counter (OTC) Drugs FSA Guide Over-The-Counter Drugs & Products Reimbursable through a Healthcare Flexible Spending Account IRS Revenue Ruling 2003-102, permits many OTC drugs to be reimbursed medical expenses in an FSA. Under the ruling, (OTC) drugs purchased without a physician’s prescription are reimbursable as long as the it
SISC Flex Plan HEALTH CARE AND DEPENDENT CARE EXPENSES *Please note, all "potentially eligible expenses" require a Certification of Medical Necessity form completed by your medical practitioner in order to be considered eligible for reimbursement. The letter must include 1. Medical condition/diagnosis 2. Specific recommended treatment 3. Duration of treatment. This letter must be sub