Pharmacokinetics and Pharmacodynamicsof Nelfinavir Administered Twice or ThriceDaily to Human Immunodeficiency VirusType 1–Infected Children
G. Gatti,1,a G. Castelli-Gattinara,2 M. Cruciani,3 S. Bernardi,2 C. R. De Pascalis,1 E. Pontali,1 L. Papa,1 F. Miletich,1 and D. Bassetti1
1Gaslini Childrens Hospital, Genoa, 2Bambin Gesu` Childrens Hospital, Rome, and 3Center of Preventive Medicine/HIV Outpatient Clinic,Verona, Italy
We studied the pharmacokinetics and pharmacodynamics of nelfinavir administered 2 or 3 times per day to human immunodeficiency virus type 1 (HIV-1)–infected children receiving highly active antiretroviral therapy containing nelfinavir. The geometric mean trough concentrations of nelfinavir for the thrice- and twice-daily regimens were 1.55 mg/L and 1.11 mg/L, respectively (P p not significant). Nelfinavir concentrations did not correlate with total daily dose, dose per kilogram of weight, age, weight, previous protease inhibitor (PI) experience, or CD4+ cell percentage. In the 25 PI-naive children, the virus load reductions at 24 weeks of treatment with the twice- and thrice-daily regimens were comparable. A significantly higher percentage of children in the twice-daily group had a trough concentration of nelfinavir of less than the inhibitory concen- tration of 95% (P p .042). The decrease in the virus load at 24 weeks of treatment was not correlated with the trough concentration of nelfinavir. The variability of trough concentrations was extremely high, particularly among recipients of the twice-daily regimen, resulting in a higher number of patients with subinhibitory concentrations of nelfinavir in this group.
Although several aspects of HIV infection are similar
macokinetics of nelfinavir have been investigated in
for patients of all age groups, pediatric HIV infection
healthy volunteers and in HIV-infected adults [2, 9, 10].
requires special considerations with respect to epide-
Data on the pharmacokinetics of nelfinavir in children
miological, clinical, pharmacokinetic, and therapeutic
with HIV infection are scarce [3, 4, 6, 11–13]. In older
issues [1]. Nelfinavir is one of the currently available
children, administration of nelfinavir at a dosage of
protease inhibitors (PIs) used for the treatment of HIV
∼20–30 mg/kg 3 times per day provides exposure sim-
infection in both adults and children [2–8]. The phar-
ilar to a dosage of 750 mg 3 times per day for adults.
Nelfinavir has recently been approved for a twice-
daily dose regimen for adults, whereas, for pediatricpatients, twice-daily administration is being studied [1].
Received 25 August 2002; accepted 10 February 2003; electronically published
However, the pharmacokinetics of twice-daily admin-
istration of nelfinavir to children is limited to prelim-
Financial support: Istituto Superiore di Sanita´, Rome (grant 30C8), and a grant
from Gaslini Children’s Hospital, Genoa, Italy.
inary reports [4, 11, 12]. Because a twice-daily regimen
a Present affiliation: Vertex Pharmaceuticals, Cambridge, Massachusetts.
may improve adherence to treatment, additional eval-
Reprints or correspondence: Dr. Giorgio Gatti, Malattie Infettive, Nuovo
uation of the pharmacokinetics of twice-daily regimens
Isolamento Ospedale San Martino, 16132 Genova, Italy (gatti@vpharm.com).
of nelfinavir in children is timely and relevant. Clinical Infectious Diseases 2003; 36:1476–82
The present study was designed to evaluate pharma-
2003 by the Infectious Diseases Society of America. All rights reserved.
cokinetic and pharmacodynamic data for HIV-1–infected
1476 • CID 2003:36 (1 June) • HIV/AIDS
children receiving HAART that involves twice- or thrice-daily
(for 20 children). The drug was taken with food, as recom-
administration of nelfinavir. The pharmacokinetic study aimed
to assess the variability of plasma concentrations of nelfinavir
Adherence to the treatment regimen and dietary require-
for the administered regimen. In the pharmacodynamic study,
ments was evaluated at every visit by an interview conducted
we focused on the relationship between the trough concentra-
by the care givers. Only patients defined as compliant with
tion of nelfinavir and the virologic response in PI-naive
treatment (compliance of у95%) were included in the analysis
Obtainment of blood samples for nelfinavir concentration analysis.
Blood samples (5–7 mL) were drawn into prehe-
parinized vacutainer tubes before a morning dose of nelfinavir
PATIENTS, MATERIALS, AND METHODS
of the morning dose. All samples were obtained 9–16 weeks
This open-label prospective study was conducted at 2 large
after the initiation of nelfinavir treatment. At the time of study,
Italian children’s hospitals (Istituto G. Gaslini, Genoa, and Os-
none of the children had diarrhea or had received drugs known
pedale Pediatrico Bambin Gesu`, Rome). The study protocol
or suspected to interact with nelfinavir.
was approved by the local institutional review boards of both
Analytical methods.
institutions. Written informed consent was obtained from the
were determined using a validated high-performance liquid
parents or guardians of the children before study entry. The
chromatography (HPLC) assay. In brief, standard curves and
pharmacokinetic portion of the study aimed to evaluate the
quality-control samples were prepared using nelfinavir powder
variability of plasma concentrations of nelfinavir after twice-
(kindly donated by Agouron Pharmaceuticals). Samples were
or thrice-daily administration and to correlate nelfinavir con-
loaded onto a 10-mg, 96-well Oasis MCX Extraction Plate (Wa-
centrations with potential predictors of patient exposure to the
ters), washed with acidified water, and then washed with ace-
drug. The pharmacodynamic portion of the study was limited
tonitrile. Elution was performed with a basic mixture of ace-
to PI-naive children and designed to evaluate the relationship
tonitrile and methanol; the samples were evaporated to dryness
between trough concentration of nelfinavir and virologic re-
under a gentle stream of nitrogen. The extracts were redisolved
sponse after twice- or thrice-daily administration of nelfinavir.
in a mobile phase of phosphate buffer (25 mmol/L; pH, 5) and
Study subjects.
The study population included 35 children
acetonitrile (55:45 v/v) for direct injection into the HPLC sys-
vertically infected with HIV-1, regardless of disease classifica-
tem. Nelfinavir was separated with a 5-mm Symmetry Shield
tion [14]. Twenty-five children were PI naive, and the remaining
Column (Waters) at a flow rate of 1.5 mL/
10 were PI experienced. To be eligible for enrollment in the
min (L-7100 LaChrom Pump; Merck-Hitachi). The detector
study, children had to have been receiving nelfinavir for у1
(L-4200 UV-VIS; Merck-Hitachi) was set at a wavelengh of 210
month before study entry. Before study entry, a complete med-
nm. Chromatography was performed at room temperature
ical history was obtained, a physical examination was done,
(20ЊC–25ЊC). All reagents were HPLC gradient grade.
and a panel of laboratory tests, which consisted of a chemistry
Peaks of interest were quantified using a TurboChrom Nav-
screening and a complete blood cell count with differential and
igator 4.0 Chromatography Data System (Perkin Elmer). The
concentration standard curve was prepared in the range of
Virologic and immunologic assessment.
0.1–15 mg/mL. Precision (intraday and interday variabilities;
lymphocyte count, and CD4+ cell percentage were measured at
9 of the assay was !10% at each of the quality-control
baseline and every 12 weeks. The plasma virus load was de-
concentrations (0.75, 3, and 10 mg/mL). The average recovery
termined using the branched DNA assay (Chiron), which has
was 78.6%, and the lower limit of quantification was 0.1 mg/
a lower limit of quantification of 400 copies/mL. The CD4+
lymphocyte count and the percentage of CD4+ lymphocytes,
Pharmacokinetic, pharmacodynamic, and statistical analy-
with respect to the overall lymphocyte count (CD4+ cell per-
sis.
The data obtained from all 35 study patients were used
centage), were determined using Coulter (Coulter Electronics)
for pharmacokinetic analysis. The baseline characteristics of
or Ortho (Ortho Diagnostic System) flow cytometry kits.
children receiving the twice- or thrice-daily nelfinavir regimen
Drug administration.
were analyzed using x2 test, Fisher’s exact test, and Student’s t
were receiving nelfinavir tablets in combination with 2 nucle-
test. Peak and trough concentrations of nelfinavir after twice-
oside analogue reverse-transcriptase inhibitors (NRTIs) or
daily administration were compared with concentrations after
NRTI(s) plus a nonnucleoside reverse-transcriptase inhibitor.
thrice-daily administration using the Mann-Whitney U test.
The dosage of nelfinavir administered to each patient was the
Correlations of plasma concentrations of nelfinavir with dem-
closest approximation to the recommended dosages of 20–30
ographic and other potentially predictive variables were ex-
mg/kg every 8 h (for 15 children) and 50 mg/kg every 12 h
plored using the Pearson correlation coefficient, which was
HIV/AIDS • CID 2003:36 (1 June) • 1477 Baseline demographic and clinical characteristics of children in the study.
CDC HIV disease stage, no. (%) of patients
CDC, Centers for Disease Control and Prevention.
a Patients were protease inhibitor naive.
obtained by unweighted regression analysis. The following var-
iables were tested: total daily dose, dose per kilogram of bodyweight, dosage regimen (twice-daily vs. thrice-daily), age,
Study populations.
Thirty-five children were enrolled in the
weight, previous PI experience, and baseline CD4+ cell per-
study during the period of February 1999 through September
centage. The percentage of CD4+ cells was considered because
2000. Baseline patient characteristics are shown in table 1. Of
children may have had physiological lymphocytosis. Therefore,
the 35 children, 10 were PI experienced and 25 were PI naive.
the CD4+ cell percentage may be a more reliable parameter of
This subgroup of 25 patients was included in the pharmaco-dynamic analysis.
disease progression and treatment efficacy than is the absolute
Twenty children (14 of whom were PI naive) received nel-
CD4+ cell count in this particular population. Multivariate
finavir at a mean dosage of 47.2 mg/kg twice per day (range,
analysis was performed using the stepwise multiple regression
32.9–62.5 mg/kg b.i.d.). Fifteen children (11 of whom were PI
test when the result of univariate analysis was statistically
naive) received a mean dosage of 25.8 mg/kg 3 times per day
(range, 17.4–35.7 mg/kg t.i.d.). No statistically significant dif-
Only the 25 PI-naive children were included in the phar-
ferences were found between patients receiving twice-daily reg-
macodynamic analysis. The virus load was measured at baseline
imens and those receiving thrice-daily regimens with regard to
and after 24 weeks of nelfinavir therapy. The relationship be-
age, sex, previous PI experience, weight, baseline CD4+ cell
tween virologic response (virus load at 24 weeks minus the
percentage, total number of CD4+ cells, HIV-1 infection clas-
virus load at baseline) and trough concentration of nelfinavir
sification group (by Centers for Disease Control and Prevention
was evaluated by linear and nonlinear regression. Also, the
criteria), and baseline virus load (table 1).
percentage of patients with trough concentrations that were less
A variety of antiretroviral combinations were administered
than the mean nelfinavir concentration to produce 95% in-
concomitantly with nelfinavir, including didanosine and sta-
hibition of viral replication (IC ) was compared for the twice-
vudine (10 children); stavudine and lamivudine (12 children);
daily and thrice-daily regimens. Because the activity of nelfi-
zidovudine and lamivudine (5 children); stavudine, lamivudine,
navir is reduced significantly in the presence of human serum,
and nevirapine (1 child); stavudine and nevirapine (2 children);
we used the wild-type, protein binding–corrected IC (1 mg/
stavudine and zalcitabine (2 children); zidovudine and abacavir
L), as estimated in the presence of 50% human serum [15, 16].
(2 children); and lamivudine and abacavir (1 child). At the
Statistical calculation was performed on a MacIntosh com-
time of initiation of nelfinavir treatment, 7 children were an-
puter using the Staview II program (Abacus Concepts). A P
tiretroviral therapy naive, 21 children modified all underlying
value of !.05 was considered the cutoff for statistical sig-
NRTIs, 6 children added nelfinavir to their treatment regimens,
1478 • CID 2003:36 (1 June) • HIV/AIDS Peak and trough plasma concentrations of nelfinavir.
regimen group (P p .042, by 2-tail Fisher’s exact test; figure 2,
There was a large interpatient variability in plasma concentra-
tions of nelfinavir. Plasma samples with peak nelfinavir con-
At 24 weeks of follow-up, we observed a mean virus load
centrations were obtained 3.7 ע 2.2 h after nelfinavir admin-
reduction (עSD) of 2.8 ע 0.7 log copies/mL in the twice-
daily regimen group, compared with a reduction of 2.1 ע 1.2
regimen group (geometric mean, 5.65 mg/L), compared with
log copies/mL in the thrice-daily regimen group. This differ-
2.24–11.72 mg/L in the thrice-daily regimen group (geometric
ence was not statistically significant.
mean, 4.00 mg/L). This difference was not statistically sig-
On univariate analysis, the decrease in the virus load at 24
weeks of treatment was not correlated with trough concentra-
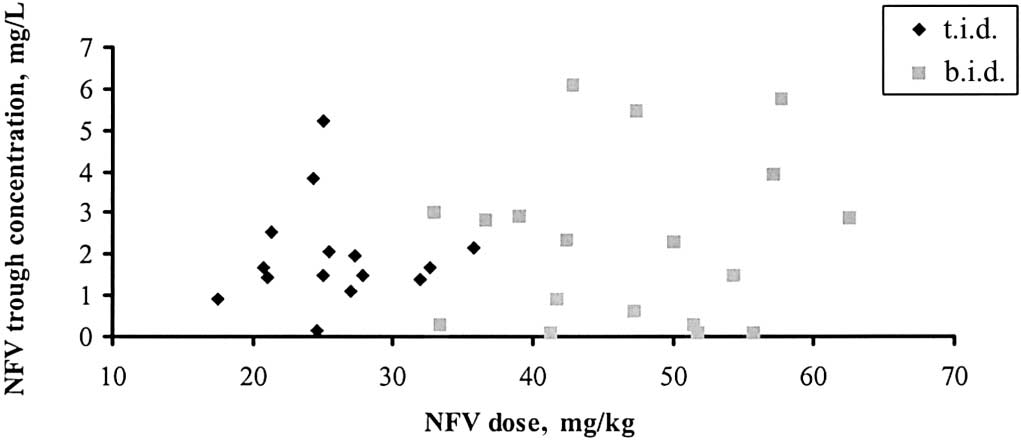
The relationship between trough plasma concentrations and
tion of nelfinavir. There was, however, a trend toward a de-
administered dose is depicted in figure 1. The geometric mean
creased virus load in patients with higher trough concentrationsof nelfinavir (figure 3).
trough concentration for the thrice-daily regimen group (1.55mg/L; range, 0.13–5.22 mg/L) was not significantly differentthan that for the twice-daily regimen group (1.11 mg/L; range,
DISCUSSION
nondetectable to 6.08 mg/L). In the whole population exam-
We studied the variability of plasma concentrations of nelfinavir
ined, peak and trough concentrations of nelfinavir did not cor-
after twice-daily and thrice-daily dosing, the correlation of
relate with total daily dose, dose per kilogram of weight, age,
plasma concentrations with potential predictors of patient ex-
weight, previous PI experience, or CD4+ cell percentage.
posure to the drug, and the relationship between trough con-
Pharmacodynamic study.
centrations of nelfinavir and virologic response, according to
SD for the 25 PI-naive children in the twice-daily
14 and thrice-daily (n p 11) groups, respectively, were
In our study of 35 children, we found an extremely high
as follows: age, 8.1 ע 3.0 versus 6.3 ע 2.5 years; weight,
interindividual variability in trough and peak concentrations
20.2 ע 6.9 versus 21.6 ע 7.1 kg; baseline CD4+ cell percentage,
of nelfinavir, as was already observed in adults and in small
20.6% ע 10.7% versus 26.3% ע 12.0%; and baseline virus
cohort studies of children [2, 4, 6, 11–13, 17, 18]. We did not
load, 5.1 ע 0.4 versus 5.2 ע 0.8 log copies/mL. Mean dosages
identify factors that could explain the observed variability in
of nelfinavir were 48.7 mg/kg twice per day (range, 33.3–62.5
plasma concentrations of nelfinavir. Despite the high dose range
mg/kg b.i.d.) and 27.6 mg/kg 3 times per day (range, 21.4–35.7
used, peak and trough concentrations did not correlate with
mg/kg t.i.d.), respectively. Geometric mean trough concentra-
total daily dose and dose per kilogram of weight, nor with age,
tions of nelfinavir in the twice- and thrice-daily regimen groups
weight, previous PI experience, and CD4+ cell percentage. Pos-
were 0.94 mg/L (range, not detectable to 5.74 mg/L) and 1.63
sible sources of variation in plasma concentrations are attrib-
mg/L (range, 0.13–5.22 mg/L), respectively. Seven (50%) of 14
utable to peculiar pharmacokinetic properties of nelfinavir. Be-
children in the twice-daily regimen group had a trough con-
cause the drug has relatively slow gut absorption, peak and
centration of nelfinavir of !1 mg/L (estimated IC
trough concentrations may occur after the C
value), compared with 1 (9%) of 11 children in the thrice-daily
ples have been obtained [19]. Moreover, as already observed
Figure 1.
The relationship between nelfinavir (NFV) dose per kilogram of body weight and predose plasma concentration of NFV
HIV/AIDS • CID 2003:36 (1 June) • 1479 Figure 2.
The trough concentrations of nelfinavir in protease inhibitor–naive children receiving nelfinavir thrice (top) or twice (bottom) per day. Horizontal line, protein binding–corrected concentration producing 95% inhibition of viral replication (IC ) of nelfinavir (1 mg/L) for wild-type virus.
with other PIs, the variability of nelfinavir concentrations may
in the twice-daily regimen group. Eight (40%) of 20 patients
reflect the interindividual variability in the activity of the P450
in the twice-daily regimen group, compared with 2 (13%) of
enzyme system metabolizing the drug and the extent of its
15 patients in the thrice-daily regimen group, had a trough
saturability. It should be noted that, in our study, nevirapine
concentration that was less than the wild-type, protein bind-
was coadministered to 3 children (2 in the thrice-daily regimen
of 1 mg/L [15, 16]. Although the limit of
group and 1 in the twice-daily regimen group); however, this
this approach should be acknowledged, particularly in the pres-
drug did not appear to influence nelfinavir metabolism in vivo
ence of drug-resistant virus, the finding of a trough plasma
level that was less than the minimum effective concentration
In our study, trough and peak concentrations did not differ
should be recognized as a clear indication of treatment inad-
between regimen groups. Although this was an observational
study without randomized design, it is unlikely that the design
Because there is evidence showing a relationship between
introduced an important bias. Our results are in agreement
virologic outcome and plasma concentration of PIs [19], we
with the results of other studies that have compared concen-
investigated the effect of thrice-daily versus twice-daily admin-
trations of nelfinavir after administration of twice-daily and
istration of nelfinavir on virologic response. Because previous
thrice-daily regimens in children [4, 11, 12] and adults [18].
exposure history may affect the emergence of drug-resistant
Of interest, we found that the interindividual variability in
HIV variants, in this part of the study, we included only PI-
the plasma concentration of nelfinavir was even more evident
1480 • CID 2003:36 (1 June) • HIV/AIDS Figure 3.
The relationship between the decrease in the virus load at 24 weeks of treatment and trough concentrations of nelfinavir (NFV) in
protease inhibitor–naive children.
Overall, patients responded well to treatment. The mean re-
of nelfinavir daily dose and concomitant antiretroviral drugs
duction in the virus load did not differ significantly between
received, may also be regarded as a source of variability. On
recipients of the twice-daily regimen and recipients of the
the other hand, the study was aimed at harvesting data reflecting
thrice-daily regimen, despite there being a significantly higher
number of children in the twice-daily regimen group with
Although the lack of correlation between virologic outcome
trough concentrations that were less than the IC . Also, the
and exposure would suggest that TDM may not be of benefit
decrease in the virus load at 24 weeks of treatment did not
for this particular clinical setting, the above description of con-
correlate with trough concentrations of nelfinavir, even though
founding factors should mitigate this conclusion. In fact, the
we observed a trend toward a better response in patients with
high interindividual variability in plasma concentrations is in
favor of TDM, as a recent study also suggests [21].
In the present study, there are several factors that can explain
In conclusion, our study confirms the unpredictability of
the lack of difference in virologic response between recipients
plasma concentrations of nelfinavir. The variability of trough
of twice-daily regimens and recipients of thrice-daily regimens,
concentrations was extremely high, particularly in the twice-
as well as the lack of correlation between exposure and response.
daily regimen group, resulting in a higher number of patients
First of all, the number of PI-naive children was too low to
who had a trough concentration less than the IC in the twice-
detect significant differences in virologic response between
daily regimen group, compared with the thrice-daily regimen
group. Despite this difference in exposure, the virologic re-
exposure. In fact, in some patients, the plasma concentration
sponse at 24 weeks of treatment was similar for the 2 dosage
of PIs continues to decay after drug administration because of
regimens in PI-naive children. A number of confounding fac-
delayed absorption. Moreover, the utility of estimating single
tors may explain the lack of correlation between nelfinavir ex-
plasma drug concentrations (trough or random sample) is un-
posure and virologic response. Therefore, our study does not
clear at this time [19]. Third, in our study, we did not monitor
exclude the utility of TDM, which is instead suggested by the
the M8 nelfinavir metabolite, although this procedure does not
high interindividual variability in plasma concentrations.
seem to be essential for the purpose of therapeutic drug mon-itoring (TDM) [17]. Fourth, we did not provide data on in-tracellular concentration of antiretroviral drugs and on the pos-
References
sibility of antiretroviral drug interactions (synergy, antagonism,
1. Centers for Disease Control and Prevention. Guidelines for the use of
or indifference). Fifth, the twice-daily regimen of nelfinavir may
antiretroviral agents in pediatric HIV infection. MMWR Recomm Rep
have facilitated adherence to the treatment regimen. Questions
1998; 47:1–43.
about treatment adherence were asked at every visit; however,
2. Bardsley-Elliot A, Plosker GL. Nelfinavir: an update on its use in HIV
infection. Drugs 2000; 59:581–620.
a more comprehensive assessment may have detected differ-
3. Starr SE, Fletcher CV, Spector SA, et al. Combination therapy with
ences between regimens. Clearly, patient heterogeneity, in terms
efavirenz, nelfinavir, and nucleoside reverse-transcriptase inhibitors in
HIV/AIDS • CID 2003:36 (1 June) • 1481
children infected with human immunodeficiency virus type 1. N Engl
12. Hayashi S, Wiznia A, Jaywardene A, et al. Nelfinavir pharmacokinetics
J Med 1999; 341:1874–81.
in stable HIV positive children: the effect of weight and a comparison
4. Wizna A, Stanley K, Krogstad P, et al. Combination nucleoside analog
of BID to TID dosing [abstract 427]. In: Program and abstracts of the
reverse transcriptase inhibitor(s) plus nevirapine, nelfinavir, or rito-
6th Conference on Retroviruses and Opportunistic Infections (Chi-
navir in stable antiretroviral therapy–experienced HIV-infected chil-
cago). Alexandria, VA: Foundation for Retrovirology and Human
dren: week 24 results of a randomized controlled trial—PACTG 377.
Health, 1999:148.
AIDS Res Hum Retroviruses 2000; 16:1113–21.
13. Capparelli EV, Sullivan JL, Mofenson L, et al. Pharmacokinetics of
5. Nadal D, Steiner F, Cheseaux JJ, et al. Long-term responses to treatment
nelfinavir in human immunodeficiency virus–infected infants. Pediatr
including ritonavir or nelfinavir in HIV-1–infected children. Infection
Infect Dis J 2001; 20:746–51. 2000; 28:287–96.
14. Centers for Disease Control and Prevention. Guidelines for the use of
6. Krogstad P, Wiznia A, Luzuriaga K, et al. Treatment of human im-
antiretroviral agents in pediatric HIV infection. MMWR Morb Mortal
munodeficiency virus 1–infected infants and children with the protease
Wkly Rep 1998; 47:1–43.
inhibitor nelfinavir mesylate. Clin Infect Dis 1999; 28:1109–18.
15. Molla A, Vasavanoda S, Kumar G, et al. Human serum attenuates the
7. Funk MB, Linde R, Wintergerst U, et al. Preliminary experiences with
activity of protease inhibitors toward wild-type and mutant human
triple therapy including nelfinavir and two reverse transcriptase in-
immunodeficiency virus. Virology 1998; 250:255–62.
hibitors in previously untreated HIV-infected children. AIDS 1999; 13:
16. Condra JH, Petropoulos CJ, Ziermann R, Schleif WA, Shivaprakash
M, Emini EA. Drug resistance and predicted virologic responses to
8. Gibb DM, Newberry A, Klein N, et al. Immune repopulation after
human immunodeficiency virus type 1 protease inhibitor therapy. J
HAART in previously untreated HIV-1–infected children. Paediatric
Infect Dis 2000; 182:758–65.
European Network for Treatment of AIDS (PENTA) Steering Com-
17. Baede-van Dijk PA, Hugen PWH, Verweij-van Wissen CPWGM, Koop-
mittee. Lancet 2000; 355:1331–2.
mans PP, Burger DM, Hekster YA. Analysis of variation in plasma
9. Quart BD, Chapman SK, Peterskin J, et al. Phase I safety, tolerance,
concentrations of nelfinavir and its active metabolite M8 in HIV-pos-
pharmacokinetics and food effect studies of AG1343—a novel HIV
itive patients. AIDS 2001; 15:991–8.
protease inhibitor [abstract LB3]. In: Proceedings of the 2nd National
18. Marzolini C, Buclin T, Decosterd LA, et al. Nelfinavir plasma levels
Conference on Human Retroviruses and Opportunistic Infections
under twice-daily and three-times-daily regimens: high interpatient and
(Washington, DC). Washington, DC: American Society for Microbi-
low intrapatient variability. Ther Drug Monit 2001; 23:394–8.
ology, 1995:167.
19. Khoo SH, Gibbons SE, Back DJ. Therapeutic drug monitoring as a
10. Moyle GJ, Youle M, Higgs C, et al. Safety, pharmacokinetics, and an-
tool in treating HIV infection. AIDS 2001; 15(Suppl 5):S171–81.
tiretroviral activity of the potent, specific human immunodeficiency
20. Malaty L, Kuper JJ. Drug interactions of HIV protease inhibitors. Drug
virus protease inhibitor nelfinavir: results of a phase I/II trial and
Safety 1999; 20:147–69.
extended follow-up in patients infected with human immunodeficiency
21. Bergshoeff AS, Fraaij P, Wolfs T, et al. Nelfinavir pharmacokinetics in
virus. J Clin Pharmacol 1998; 38:736–43.
HIV infected children: who are at risk for subtherapeutic plasma levels
11. Schuster T, Linde R, Wintergerst U, et al. Nelfinavir pharmacokinetics
[abstract TuPeB4557]? In: Program and abstracts of the 14th Inter-
in HIV-infected children: a comparison of twice daily and three times
national AIDS Conference (Barcelona). Stockholm: International AIDS
daily dosing. AIDS 2000; 14:1466–8.
Society, 2002:14.
1482 • CID 2003:36 (1 June) • HIV/AIDS
The Global Campaign to Reduce the Burden of Headache Worldwide A partnership in action between the World Health Organization, World Headache Alliance, International Headache Society and European Headache Federation Headache disorders are common and ubiquitous. They have a neurological basis, but headache rarely signals serious underlying illness. The huge public-health importance of headach
PESTICIDE NOTIFICATION August 2013 The Healthy Schools Act of 2000/AB2260 contains the following procedures to control pests and minimize exposure of children, faculty, and staff to pesticides/herbicides: • Warning signs will be posted at all entrances to school district property 48 hours prior to regular pesticide/herbicide applications and will remain posted for 72 hours after the applic
 Peak and trough plasma concentrations of nelfinavir.
Peak and trough plasma concentrations of nelfinavir.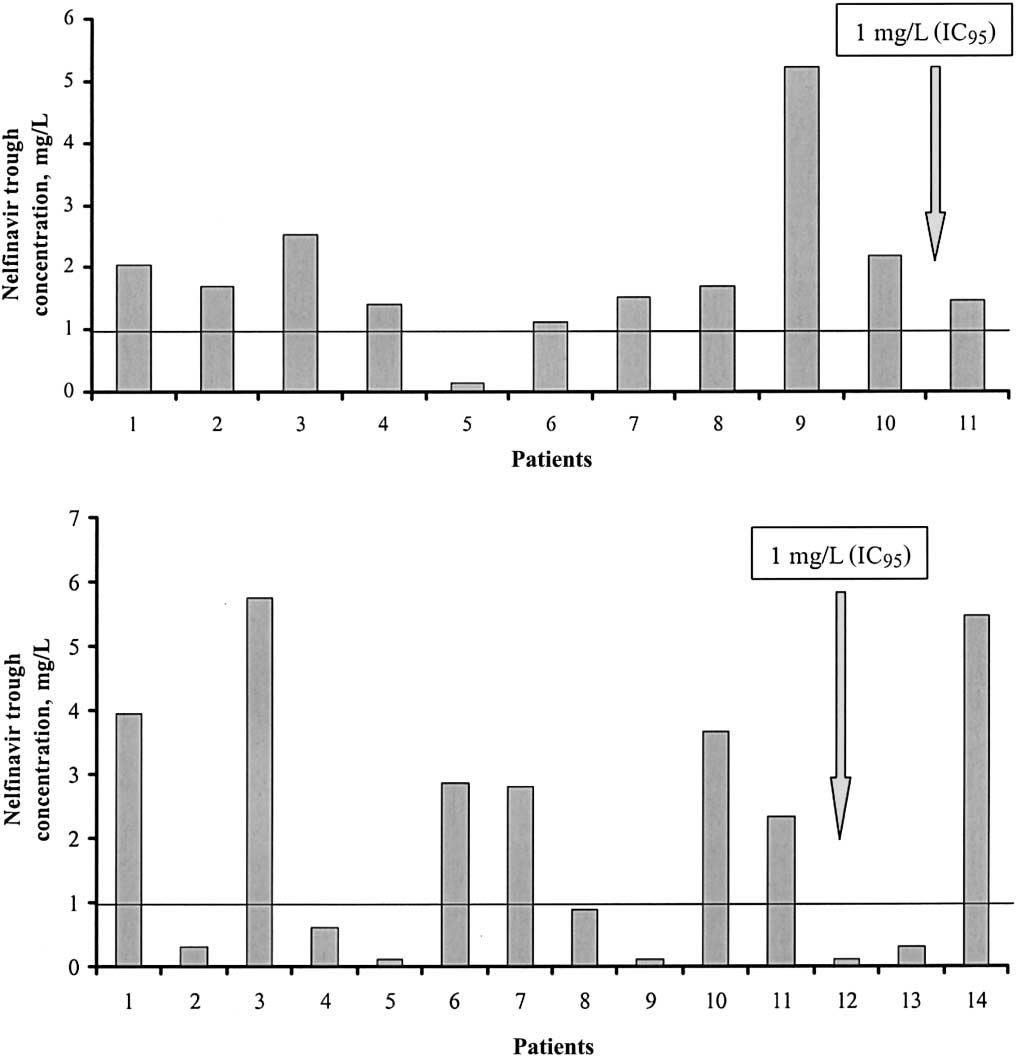 Figure 2.
Figure 2.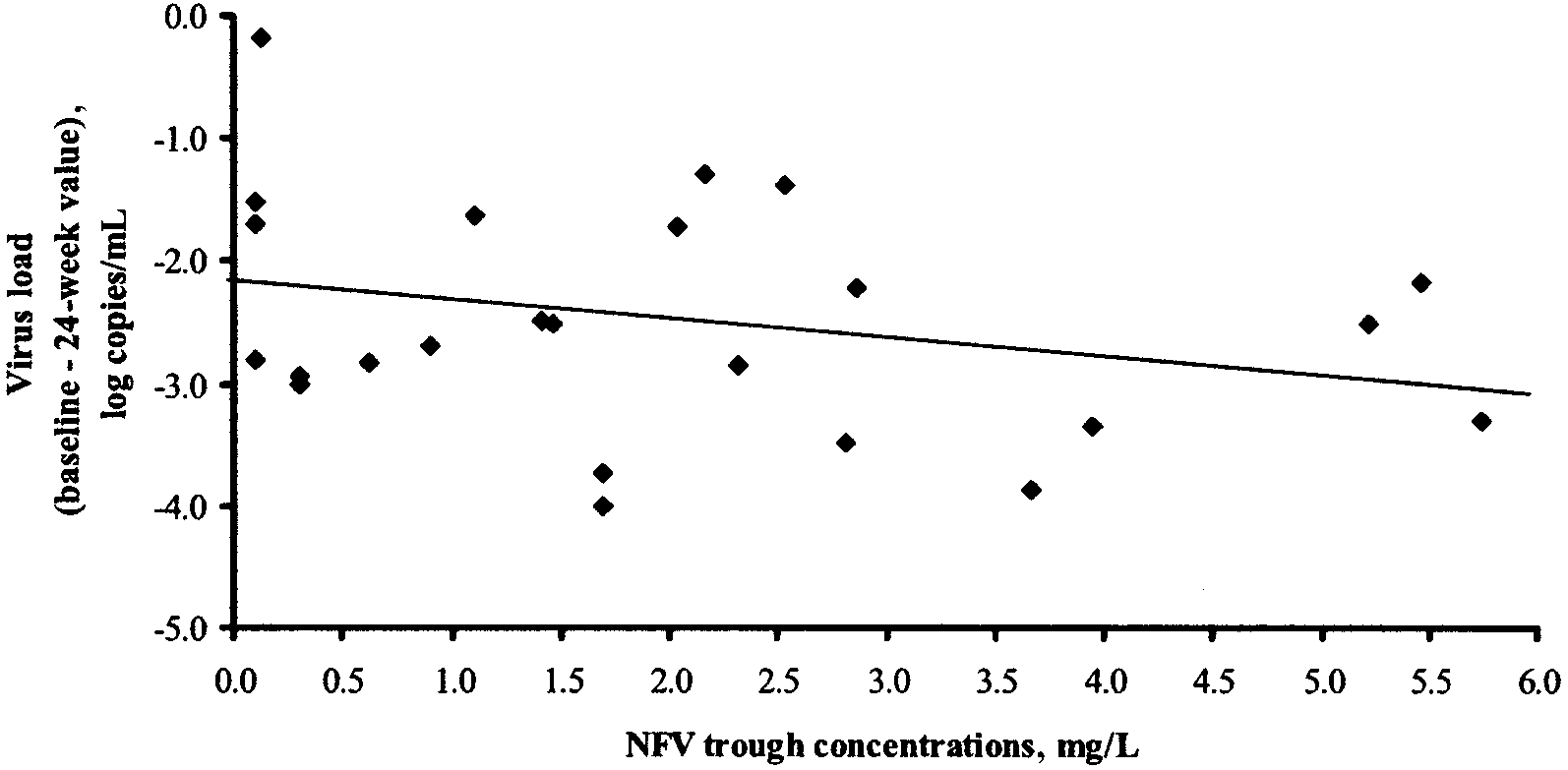 Figure 3.
Figure 3.