Lithium Dilution Cardiac Output Measurement in Oleic Acid–Induced Pulmonary Edema
Tadayoshi Kurita, MD, Koji Morita, PhD, Hiroyuki Kawasaki, BSc, Kiyoyasu Fujii, BSc,
Tomiei Kazama, MD, and Shigehito Sato, MD
Objective: To determine whether lung injury influences infusion, CO measurements were repeated in the same man- the accuracy of lithium dilution cardiac output (CO) mea- ner as the control measurement had been taken. surement. Measurements and Main Results: Under each condition, Design: Animal experimental study. right atrium lithium injection was similar to left ventricle Setting: Animal experimental laboratory. lithium injection. The mean of these differences at injury Participants: Swine (n ؍ 23) weighing 26.4 ؎ 2.47 kg (؊0.06 ؎ 0.55 L/min) was the same as that at control (mean ؎ SD). (؊0.05 ؎ 0.36 L/min). Interventions: The animals were anesthetized and trache- Conclusions: Although the variability of lithium dilution otomized, then a pulmonary artery catheter was inserted CO measurement after oleic acid–induced pulmonary edema into the right jugular vein, and a catheter (18G) was placed was greater than that of the control, this technique was in the femoral artery. After median sternotomy and pericar- acceptable even in cases of lung injury. diotomy, a left ventricular catheter (18G) was directly in- Copyright 2002, Elsevier Science (USA). All rights reserved. serted. CO was measured by giving a bolus injection of lithium chloride into either the right atrium or the left ven- KEY WORDS: cardiac output (CO), indicator dilution, lithium tricle in each animal. After control measurements, perme- dilution, thermodilution, critical care, lung injury, oleic acid, ability pulmonary edema was initiated by infusing oleic acid pulmonary edema, measurement technique, pulmonary ar- into the central vein (injury). About 2 hours after oleic acid tery catheter THE LITHIUM DILUTION TECHNIQUE for the mea- drome. If there is a significant loss of lithium after an increase
surement of cardiac output (LiDCO) (LiDCO, Ltd, Lon-
in pulmonary capillary permeability, this loss could affect the
don, UK) was introduced by Linton et al1,2 in 1993 and has
CO values measured by the LiDCO technique. To the authors’
been developed further more recently. The LiDCO system has
knowledge, no previous studies have investigated the reliability
been approved by the Food and Drug Administration and is
of the LiDCO technique after acute lung injury. The present
now in use in several hospitals in the United States. In this
study was conducted to assess the reliability of the LiDCO
method of cardiac output (CO) measurement, lithium chloride
technique by comparing the CO values before and after injec-
is injected into the atrium through a central venous catheter,
tion of lithium chloride into the right atrium or left ventricle
and CO can be determined from the arterial lithium dilution
using a pulmonary edema model in swine.
curve, without a pulmonary artery catheter. In a previous ani-
mal study, this method was more accurate than that of conven-tional thermodilution in comparison with direct electromag-
This study was approved by the Committee on Animal Research,
Hamamatsu University School of Medicine, Hamamatsu, Japan. Twenty-
netic flowmetry (the laboratory gold standard).3 A peripheral
three swine (mean body weight Ϯ SD, 26.4 Ϯ 2.47 kg) were studied.
vein, which is more easily accessed than a central vein, could
After administration of ketamine, 10 mg/kg intramuscularly, general
be used for the indicator injection port.4,5 Because there are
anesthesia was induced by inhalation of 5% sevoflurane in oxygen at 6
some objections regarding the use of a pulmonary artery cath-
L/min using a standard animal mask. After tracheostomy, anesthesia
eter,6 this method could be considered as an alternative one that
was maintained with 4% end-tidal sevoflurane and 100% oxygen via
does not involve the use of a pulmonary artery catheter for
mechanical ventilation. A peripheral venous catheter (20G) was placed
management of critically ill patients.
in the dorsal ear vein, and lactated Ringer’s solution was infused at a
The accuracy of the LiDCO method depends on the loss of
rate of 10 mL/kg/h. After induction, pancuronium bromide was admin-
lithium in the lungs being negligible; Band et al7 reported that
istered to ensure proper control of ventilation. Lead II of an electro-cardiogram was monitored with subcutaneous electrodes in the legs.
this loss was clinically insignificant. In clinical situations, the
A pulmonary artery catheter (5F, 4-lumen; Nihon Kohden, Tokyo,
pulmonary capillary permeability becomes greater than normal
Japan) was inserted into the right jugular vein, and a catheter (18G) was
as a result of raised left atrial pressure, residual effects of recent
placed in the femoral artery. After median sternotomy and pericardiot-
cardiopulmonary bypass, and adult respiratory distress syn-
omy, a left ventricular catheter (18G) was directly inserted. The posi-tion of the left ventricular catheter was checked after the swine hadbeen killed with potassium chloride under deep anesthesia with 5%
From the Department of Anesthesiology and Intensive Care,
inspired sevoflurane. A lithium sensor was attached to the femoral
Hamamatsu University School of Medicine, Hamamatsu; and Research
artery for measurement of the lithium concentration. Heparin (100
and Development Center, Nipro Corporation, Osaka, Japan.
U/kg) was administered to avoid blood coagulation on the membrane
All funding from the Department of Anesthesiology and Intensive
surface of the lithium sensors, and deterioration of the sensors was
Care, Hamamatsu University School of Medicine.
prevented. By warming with heat lamps, the blood temperature of the
Address reprint requests to Tadayoshi Kurita, MD, Department of
swine was maintained in the range of 38.5°C to 40.0°C. Anesthesiology and Intensive Care, Hamamatsu University School of
After hemodynamic stability had been maintained for at least 10
Medicine, 1-20-1 Handayama, Hamamatsu, 431-3192 Japan. E-mail:
minutes, CO was determined. The LiDCO technique was performed by
giving a bolus injection of lithium chloride into the right atrium through
Copyright 2002, Elsevier Science (USA). All rights reserved.
the atrial port of the pulmonary artery catheter (LiD-RA) or into the left
ventricular catheter (LiD-LV). During apnea at the end of expiration,
the same person administered lithium chloride. The interval between
Journal of Cardiothoracic and Vascular Anesthesia, Vol 16, No 3 (June), 2002: pp 334-337
LITHIUM DILUTION CARDIAC OUTPUT MEASUREMENT
transit time of lithium dilution curves representing injection into the leftventricle).9
The statistical data analysis was performed using StatView 4.54
(Abacus Concepts, Berkeley, CA). A paired t-test was performed tocompare each arterial blood gas and hemodynamic parameter, LiD-RA,LiD-LV, the difference between LiD-RA and LiD-LV (⌬), the differ-ence expressed as a percentage of the left ventricular injection value(⌬%), and MTT-LiD-RA and MTT-LiD-LV between control and in-jury conditions. LiD-RA and MTT-LiD-RA were compared withLiD-LV and MTT-LiD-LV under each condition by Student t-test. Thelinear regression equations of LiD-RA and LiD-LV under each condi-tion were calculated by simple linear regression analysis using theleast-squares method. As recommended by Bland and Altman,10 thedifference (LiD-RA Ϫ LiD-LV) was plotted against (LiD-LV ϩ LiD-RA)/2 for each condition, and the means and SDs (bias and precision)
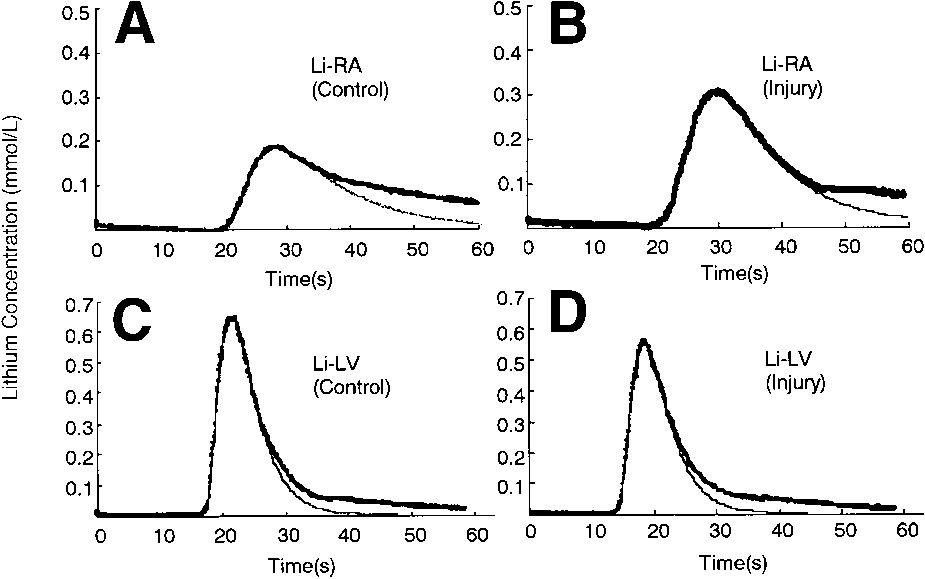
(A and B) Lithium dilution curves for lithium chloride in-
of the differences were calculated. All data are expressed as mean Ϯ
jected into the right atrium of the control (A) and after injury (B). (C
SD. A level of p ϭ 0.05 was considered significant in each statistical
and D) Lithium dilution curves for lithium chloride injected into the left ventricle of the control (C) and after injury (D). The bold lines show the data points recorded from the lithium ion selective elec- trode. The regular lines are the least-squares lognormal derived using the points from 0 to 10% down from the peak on the washout
The representative dilution curves using both injection sites
limb. The data points deviate from the lognormal as the lithium ion
and those before and after injury are shown in Fig 1. All
starts to recirculate.
dilution curves closely approximated a lognormal curve to 50%below the peak. The arterial blood gas analysis and hemody-namic data for control and oleic acid–induced injury groups are
LiD-RA and LiD-LV was kept as short as possible. The paired mea-
shown in Table 1. Two hours after oleic acid administration,
surement of CO was made in each animal. After the control measure-
the pH and PaO2 significantly decreased, and the PaCO2, mean
ment was obtained, 0.1 mL/kg of oleic acid was administered into the
pulmonary artery pressure, and pulmonary artery occlusion
right atrium over 1 hour to produce the pulmonary edema model. About
pressure significantly increased. No significant differences
2 hours after oleic acid administration and after obtaining hemody-
were observed between the mean systemic arterial pressure of
namic stability, CO measurements were determined using the same
the respective groups. Table 2 shows LiD-RA, LiD-LV, differ-
The LiDCO system was used for the measurements of CO using
ences in CO, and mean transit time of lithium dilution curves
lithium dilution. CO was measured by injecting 1 mL of an isotonic
representing injection into the right atrium (MTT-LiD-RA) and
solution of lithium chloride (0.15 mol/L) while withdrawing arterial
mean transit time of lithium dilution curves representing injec-
blood from the femoral arterial catheter at 4 mL/min past the lithium
tion into the left ventricle (MTT-LiD-LV) for each condition.
sensor. A roller pump was used to regulate the blood flow from the
Under both conditions, no statistical differences were observed
femoral arterial catheter. Lithium chloride solution, 1 mL, was injected
between LiD-RA and LiD-LV, and MTT-LiD-RA was signif-
as a bolus into the right atrium through the atrial port of the pulmonary
icantly greater than MTT-LiD-LV. The mean of those differ-
artery catheter or into the left ventricular catheter during apnea at the
ences (⌬) was Ϫ0.05 Ϯ 0.36 L/min (⌬% ϭ Ϫ1.84 Ϯ 9.18%)
end of expiration. The same person performed all injections. To ensure
for the control and Ϫ0.06 Ϯ 0.55 L/min (⌬% ϭ Ϫ0.16 Ϯ
that the bolus injection dose was exactly 1 mL, the deadspaces of the
12.62%) for the injury conditions. No significant differences in
central venous lumen of the pulmonary artery catheter (0.39 mL) andthe left ventricular catheter were filled with lithium chloride solution
any parameter were observed between control and injury con-
until a small amount of indicator leakage was observed and a small
peak appeared on the recording curve of the concentration time course.
The correlations between LiD-LV and LiD-RA in each state
The disposable sensor consisted of a lithium-selective electrode in a
are shown in Fig 2. The correlation coefficient of the linear
flow-through cell. The voltage across the lithium-selective membrane
regression line between LiD-LV and LiD-RA in the control
was digitized on-line and recorded by a dedicated computer, whichconverted the voltage signal to lithium concentration and calculated COas: CO (L/min) ϭ [dose of lithium chloride (mmol) ϫ 60]/[area undercurve (mmol/xs/L) ϫ (1 Ϫ PCV)] (area under curve ϭ the integral of
Table 1. Arterial Blood Gas and Hemodynamic Parameters
the primary curve; PCV ϭ packed cell volume). Division by (1 Ϫ
PCV) converts plasma flow to blood flow because the lithium ion is
distributed only in the plasma fraction of blood. Packed cell volume
was measured as the value of hematocrit (Kubota Hematocrit KH-
120A, Tokyo, Japan) before each CO measurement. The primary
circulation curve was distinguished from the secondary (or recircula-
tion) curve by Linton’s8 method based on the theory of lognormal
analysis to determine the integral of the primary curve. After eachexperiment, the obtained curves were evaluated to determine whether
they approximated a lognormal curve, and mean transit times (MTT)
Abbreviations: MAP, mean arterial pressure; MPAP, mean pulmo-
were calculated (MTT-LiD-RA, mean transit time of lithium dilution
nary arterial pressure; PAOP, pulmonary arterial occlusion pressure;
curves representing injection into the right atrium; MTT-LiD-LV, mean
Table 2. Lithium Dilution Cardiac Output Values at Injection Sites and the Differences in These Values
NOTE. Data are shown as mean Ϯ SD. Abbreviations: LiD-RA, lithium dilution cardiac outputs for lithium
Difference between LiD-RA and LiD-LV plotted against
chloride injected into the right atrium; LiD-LV, lithium dilution cardiac
mean at control (left) and at injury (right). The bold line shows the
output for lithium chloride injected into the left ventricle; ⌬, the
mean; regular lines indicate ؎ 2 SD.
difference between the 2 cardiac output estimations; ⌬ %, the differ-ence expressed as a percentage of the left ventricular injection value;
MTT-LiD-RA, mean transit time of lithium dilution curves represent-
ing injection into the right atrium; MTT-LiD-LV, mean transit time of
extent of diffusion of lithium into pulmonary extracellular fluid
lithium dilution curves representing injection into the left ventricle.
may be smaller, or its diffusion back into capillary blood maybe rapid when the diffusion gradient reverses. If pulmonary
state (0.93, r2 ϭ 0.86) was greater than that between LiD-LV
capillary permeability is increased, however, significant loss or
and LiD-RA in the injury state (0.87, r2 ϭ 0.75); however, this
difference was not statistically significant. The differences
The authors examined the accuracy of the LiDCO technique
(LiD-RA Ϫ LiD-LV) plotted against (LiD-LV ϩ LiD-RA)/2 in
within the period during which lithium was most likely to be
each state are shown in Fig 3. The bias (the mean of the
lost or to undergo unexpected distribution in the lung. Band et
differences) at injury (Ϫ0.06) was almost the same as that at
al7 reported in a study of cardiac surgical patients that in
control (Ϫ0.05). The precision (the SD of the differences) at
comparing the LiDCO technique of LiD-RA with LiD-LA,
injury (0.55) was greater than that at control (0.36).
LiD-RA was greater than LiD-LA, and the mean of thesedifferences was 3.6 Ϯ 4.9%. Band et al7 concluded that these
differences reflected increases of pulmonary capillary perme-
Oleic acid–induced lung injury has been established as an
ability caused by raised left atrial pressure and the residual
experimental model for permeability pulmonary edema. Previ-
effects of recent cardiopulmonary bypass.
ous investigators have reported that after its infusion, the
In the present study, LiD-LV was measured rather than
amount of extravascular lung water gradually increases over
LiD-LA because it was easier to insert a left ventricular cath-
the course of 120 minutes and reaches a plateau soon after-
eter and to confirm that there was no leakage of lithium chlo-
ward.11 Pathologic findings include alveolar flooding, epithelial
ride solution. Given that the mixture of lithium in the left
damage, and microvascular thrombosis.12 Accordingly, in the
ventricle was complete and the curve-fitting procedure accu-
present study, the CO measurements were made 2 hours after
rately discriminated the primary curve according to obtained
administering oleic acid. Chinard et al13 injected 22Naϩ into the
dilution curves (Fig 1), the difference would result from the
right atrium of anesthetized dogs and showed that its recovery
loss or unstable diffusion of lithium in the lung. Although the
in the arterial blood was similar to that of T1824 (Evans Blue,
variability of LiD-RA compared with LiD-LV at injury was
which is protein bound), showing that there was minimal loss
slightly greater than that at control (Fig 3), LiD-RA was closely
in the lungs. It is likely that lithium behaves in the same way.
correlated with LiD-LV under both conditions (Fig 2), and
When the pulmonary capillary permeability is normal, the
LiD-RA was similar to LiD-LV (Table 2). For these injectionsites, no significant difference was observed between meantransit times before and after injury (Table 2). These resultsindicated that the loss or unstable diffusion of lithium in thelung was negligible even with the lung injury. Although theaccuracy of the LiDCO technique decreased slightly with lunginjury, this finding was at a clinically insignificant level.
In the present study, the thermodilution CO measurement
was not compared with the LiDCO technique despite the in-sertion of the pulmonary artery catheter because the intervalbetween measurements was kept as short as possible. (Changesin the measurement technique require more than a few minutesto set up.) Stetz et al14 showed that individual bolus thermodi-lution readings had to change by at least 22% for a real changein CO to be assumed. Average (mean of 3) bolus thermodilu-
Linear regression between LiD-RA and LiD-LV at control (left) and at injury (right).
tion readings had to change by at least 13%. From this stand-
LITHIUM DILUTION CARDIAC OUTPUT MEASUREMENT
point, it seems to be acceptable in the clinical situation that the
is still at an acceptable level. Because this method does not
accuracy of the lithium dilution method decreases in cases of
require a pulmonary artery catheter and because a peripheral
venous catheter can be used instead of a central venous catheter at
Limitations of the present study were that the authors did not
the lithium injection site, measurement is obtained more easily;
measure the extravascular lung water, and they did not evaluate
measurements can be taken by in-place central or peripheral ve-
histologic analysis for the determination of lung edema. Given
nous and arterial catheters, which usually have already been es-
that oleic acid–induced lung injury might be less severe than
tablished in patients requiring CO measurement, without exposing
that found in other reports,15,16 these results did not completely
patients to any of the risks associated with pulmonary artery
prove the performance of the LiDCO technique in cases of
catheter insertion.17-19 Although there are some disadvantages,
more severe lung injury. Because the purpose of this study was
such as blood loss at each measurement and the possibility of
to assess the influence of lung injury on the LiDCO method, it
toxicity by multiple injections over a short time,3,4 taking the
was assumed that LiD-LV was not affected by lung injury.
results of the present study into consideration, the LiDCO
In conclusion, although the accuracy of the LiDCO tech-
technique is a viable alternative to a pulmonary artery catheter
nique decreases slightly in the lung with pulmonary edema, it
for management of CO in critically ill patients.
1. Linton RAF, Band DM, Haire KM: A new method of measuring
11. Lewis FR, Elings VB, Hill SL, et al: The measurement of
cardiac output in man using lithium dilution. Br J Anaesth 71:262-266,
extravascular lung water by thermal-green dye indicator dilution. Ann
2. Linton R, Band D, O’Brien T, et al: Lithium dilution cardiac
12. Schoene RB, Robertson HT, Thorning DR, et al: Pathophysio-
output measurement: A comparison with thermodilution. Crit Care
logical patterns of resolution from acute oleic acid lung injury in the
3. Kurita T, Morita K, Kato S, et al: Comparison of the accuracy of
13. Chinard FP, Enns T, Nolan MF: Indicator-dilution studies with
the lithium dilution technique with the thermodilution technique for the
diffusible indicators. Circ Res 10:473-490, 1962
measurement of cardiac output. Br J Anaesth 79:770-775, 1997
4. Kurita T, Morita K, Kato S, et al: Lithium dilution cardiac output
14. Stetz CW, Miller RG, Kelly GE, et al: Reliability of the ther-
measurements using a peripheral injection site: Comparison with cen-
modilution method in the determination of cardiac output in clinical
tral injection technique and thermodilution. Int J Clin Monit Comput
practice. Am Rev Respir Dis 126:1001-1004, 1982
15. Uchida T, Nakazawa K, Yokoyama K, et al: The combination of
5. Jonas MM, Kelly FE, Linton RAF, et al: A comparison of lithium
partial liquid ventilation and inhaled nitric oxide in the severe oleic acid
dilution cardiac output measurements made using central and antecu-
lung injury model. Chest 113:1658-1666, 1998
bital venous Injection of lithium chloride. Int J Clin Monit Comput
16. Baile’n MR, Monde’jar EF, Ruiz BH, et al: Immediate applica-
tion of positive-end expiratory pressure is more effective than delayed
6. Connors AF Jr, Speroff T, Dawson NV, et al: The effectiveness
positive end-expiratory pressure to reduce extravascular lung water.
of right heart catheterization in the initial care of critically ill patients.
17. Shah KB, Rao TLK, Laughlin S, et al: A review of pulmonary
7. Band DM, Linton RA, O’Brien TK, et al: The shape of indicator
artery catheterization in 6245 patients. Anesthesiology 61:271-275,
dilution curves used for cardiac output measurement in man. J Physiol
8. Linton RAF, Linton NWF, Band DM: A new method of analysing
18. Patel C, Laboy V, Venus B, et al: Acute complications of
indicator dilution curves. Cardiovasc Res 30:930-938, 1995
pulmonary artery catheter insertion in critically ill patients. Crit Care
9. He YL, Ueyama H, Tashiro C, et al: Pulmonary disposition of
propofol in surgical patients. Anesthesiology 93:986-991, 2000
19. Damen J, Bolton D: A prospective analysis of 1400 pulmonary
10. Bland JM, Altman DG: Statistical methods for assessing agreement
artery catheterizations in patients undergoing cardiac surgery. Acta
between two methods of clinical measurement. Lancet 1:307-310, 1986
Our first two babies had been conceived with the help of Clomid, a fertility drug, after much heartache and longing for a baby. When we found out we were pregnant with Jessie without the help of modern medicine we were truly shocked. Just a month or so before, we’d been taking a walk and discussing whether we were certain if we were ready to take a more permanent step about not having any more c
Indian Journal of Weed Science 45 (4): 247–249, 2013 Distribution of weed flora of greengram and blackgram in Haryana S.S. Punia*, V.S. Hooda, Anil Duhan, Dharambir Yadav and Amarjeet Department of Agronomy, CCS Haryana Agricultural Univesrity, Hisar125 004 Received: 12 October 2013; Revised: 23 December 2013 ABSTRACT To study the floristic composition of weeds in greengram, 50
 LITHIUM DILUTION CARDIAC OUTPUT MEASUREMENT
transit time of lithium dilution curves representing injection into the leftventricle).9
The statistical data analysis was performed using StatView 4.54
(Abacus Concepts, Berkeley, CA). A paired t-test was performed tocompare each arterial blood gas and hemodynamic parameter, LiD-RA,LiD-LV, the difference between LiD-RA and LiD-LV (⌬), the differ-ence expressed as a percentage of the left ventricular injection value(⌬%), and MTT-LiD-RA and MTT-LiD-LV between control and in-jury conditions. LiD-RA and MTT-LiD-RA were compared withLiD-LV and MTT-LiD-LV under each condition by Student t-test. Thelinear regression equations of LiD-RA and LiD-LV under each condi-tion were calculated by simple linear regression analysis using theleast-squares method. As recommended by Bland and Altman,10 thedifference (LiD-RA Ϫ LiD-LV) was plotted against (LiD-LV ϩ LiD-RA)/2 for each condition, and the means and SDs (bias and precision)
(A and B) Lithium dilution curves for lithium chloride in-
LITHIUM DILUTION CARDIAC OUTPUT MEASUREMENT
transit time of lithium dilution curves representing injection into the leftventricle).9
The statistical data analysis was performed using StatView 4.54
(Abacus Concepts, Berkeley, CA). A paired t-test was performed tocompare each arterial blood gas and hemodynamic parameter, LiD-RA,LiD-LV, the difference between LiD-RA and LiD-LV (⌬), the differ-ence expressed as a percentage of the left ventricular injection value(⌬%), and MTT-LiD-RA and MTT-LiD-LV between control and in-jury conditions. LiD-RA and MTT-LiD-RA were compared withLiD-LV and MTT-LiD-LV under each condition by Student t-test. Thelinear regression equations of LiD-RA and LiD-LV under each condi-tion were calculated by simple linear regression analysis using theleast-squares method. As recommended by Bland and Altman,10 thedifference (LiD-RA Ϫ LiD-LV) was plotted against (LiD-LV ϩ LiD-RA)/2 for each condition, and the means and SDs (bias and precision)
(A and B) Lithium dilution curves for lithium chloride in-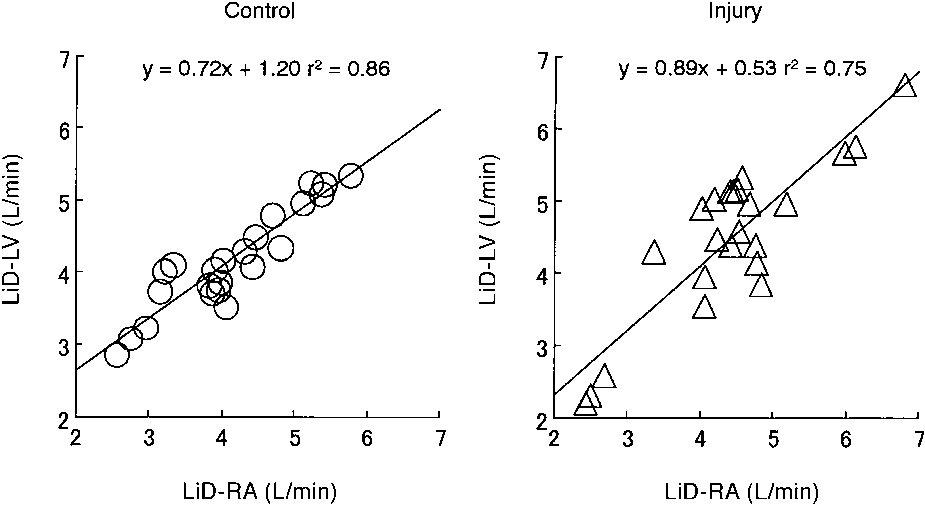
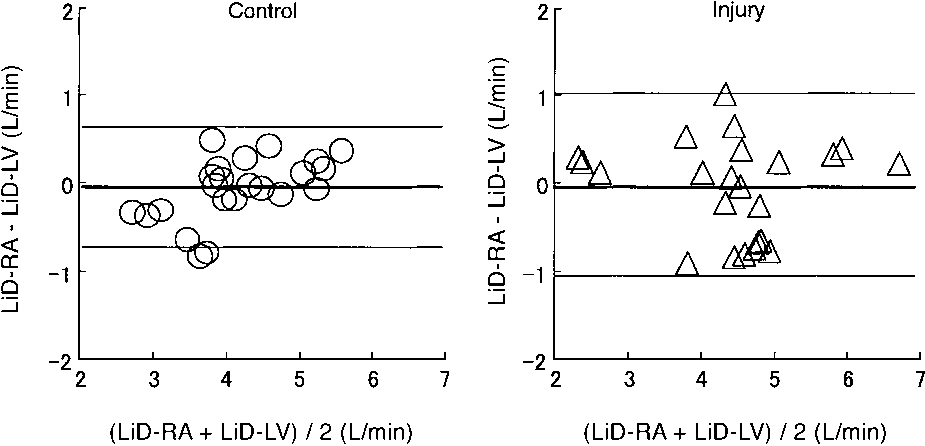 Table 2. Lithium Dilution Cardiac Output Values at Injection Sites
Table 2. Lithium Dilution Cardiac Output Values at Injection Sites