Medical Innovation Revisited: Social Contagion versus Marketing Effort1
Christophe Van den BulteUniversity of Pennsylvania
Gary L. LilienPennsylvania State University
This article shows that Medical Innovation—the landmark studyby Coleman, Katz, and Menzel—and several subsequent studiesanalyzing the diffusion of the drug tetracycline have confoundedsocial contagion with marketing effects. The article describes themedical community’s understanding of tetracycline and how thedrug was marketed. This situational analysis finds no reasons toexpect social contagion; instead, aggressive marketing efforts mayhave played an important role. The Medical Innovation data set isreanalyzed and supplemented with newly collected advertising data. When marketing efforts are controlled for, contagion effects dis-appear. The article underscores the importance of controlling forpotential confounds when studying the role of social contagion ininnovation diffusion.
Researchers from various disciplines have long studied how innovationsdiffuse through populations of individuals, households, and organizations.
1 We benefited from comments by Wayne Baker, Hans Baumgartner, Albert Bemmaor,the late Clifford Clogg, Jehoshua Eliashberg, Elihu Katz, David Krackhardt, KeithOrd, Arvind Rangaswamy, David Schmittlein, David Strang, Thomas Valente, SusanWatkins, the AJS reviewers, and audience members at the 1999 INSNA Sunbelt Con-ference, the 1994 and 1998 INFORMS Marketing Science Conferences, the AustralianGraduate School of Management, Carnegie Mellon University, Columbia University,Cornell University, Duke University, Harvard University, Catholic University of Leu-ven, University of Michigan, Northwestern University, Pennsylvania State University,Stanford University, University of North Carolina at Chapel Hill, University of Texasat Austin, and the Wharton School. We thank Thomas Valente for providing us withthe Medical Innovation data set prepared by Ronald Burt. Financial support fromPenn State’s Institute for the Study of Business Markets and the Richard D. Irwin
᭧ 2001 by The University of Chicago. All rights reserved. 0002-9602/2001/10605-0006$02.50
AJS Volume 106 Number 5 (March 2001): 1409–35
Sociologists have offered the important insight that innovation diffusionmay be driven by social contagion—another way of saying that actors’adoption behavior is a function of their exposure to other actors’ knowl-edge, attitude, or behavior concerning the innovation. Researchers haveoffered different theoretical accounts of social contagion, each describinga different causal mechanism of social influence. Information transfer.—The social influence process may simply consist
of information transfer. Actors may become aware of the existence of theinnovation through word of mouth from previous adopters (Katz andLazarsfeld 1955). Actors may also update their beliefs about the costs andbenefits of adopting the innovation after discussing it with previous adopt-ers or after observing the outcomes of adoption (e.g., increased status orprofits). Bayesian updating through social learning under risk aversion(e.g., Chatterjee and Eliashberg 1990; Roberts and Urban1988) and Ban-dura’s (1986) vicarious learning and modeling concepts are examples ofthis influence process, as is the modeling process posited by DiMaggioand Powell (1983). Normative pressures.—The social influence process may take the form
of normative pressures, such as when actors experience dissonance andhence discomfort when peers whose approval they value have adoptedan innovation, but they have not (e.g., Coleman, Katz, and Menzel 1966;Davis, Bagozzi, and Warshaw 1989; DiMaggio and Powell 1983). Competitive concern.—Social contagion may also be driven by the com-
petitive concern that one’s rivals who have adopted the innovation mightbe able to gain a competitive edge unless one adopts as well (e.g., Burt1987; Hannan and McDowell 1987). Performance network effect.—Some innovations exhibit a performance
network effect when the benefits of use, and hence of adoption, increasewith the number of prior adoptions. This effect may be direct, as withpoint-to-point communication devices like telephones and fax machines,but it may also be indirect, operating through the increased supply ofcomplementary products, as with videocassette recorders and prerecordedtapes (Katz and Shapiro 1994), or through the increased supply of sup-porting infrastructure, such as video rental stores (Brown 1981; Delacroixand Rao 1994).2
Although these social contagion mechanisms are conceptually distinct,
Foundation is gratefully acknowledged. Direct correspondence to Christophe Van denBulte, Wharton School, University of Pennsylvania, 3620 Locust Walk, Philadelphia,Pennsylvania 19104-6371. E-mail: vdbulte@wharton.upenn.edu2 Some may prefer to label such indirect endogenous feedback mediated through sup-pliers’ decisions “ecological influence” rather than “social contagion” to distinguish itfrom more direct interpersonal or interorganizational influence (Marsden and Friedkin1994).
their expressions in data may often be indistinguishable, making it im-possible to identify the exact nature of the mechanism at work (DiMaggioand Powell 1983; Montgomery and Casterline 1996). In this article, weemphasize and empirically illustrate another fundamental challenge in thestudy of social contagion in innovation diffusion processes: how socialnetwork effects may be confounded with common contextual effects.
The danger of confounding common contextual effects for social con-
tagion has long been recognized (e.g., Collier and Messick 1975; Erbringand Young 1979; Taibleson 1974). Classic studies by Katz and Lazarsfeld(1955) and Coleman et al. (1966), for instance, documented that awarenessof and attitude toward new products can be affected not only by socialcontagion but also by mass media exposure and by companies’ marketingefforts. More recent research has further challenged the empirical supportfor the role of social contagion in innovation diffusion by showing thatS-shaped diffusion curves—often interpreted as evidence of social con-tagion—can result from population heterogeneity rather than contagion(Bemmaor 1994; Bonus 1973; Thirtle and Ruttan 1987). For instance,when a product’s price decreases linearly over time and reservation pricesare normally distributed over the population, the diffusion curve will bethe normal cumulative density function. These results support concernsvoiced by England (1998) and Haunschild and Miner (1997) that thepositive relationship between the prevalence of prior adoption amongone’s network alters and the likelihood of one’s own adoption—typicallyinterpreted as evidence of social contagion—is often produced by factorsthat grow over time but that are excluded from the model.3
This article provides additional support for such concerns about con-
founding social contagion with the effect of omitted contextual variables. We show that prior evidence of social contagion gained from the MedicalInnovation study by Coleman et al. (1966) is an artifact arising fromomitting the effect of marketing efforts.4 Medical Innovation is a studyon the role of social networks in the diffusion of the broad-spectrum
3 Granovetter (1978) warned of cases in which individuals appear to react to oneanother when they are actually responding to a common, external influence. In support,he provided this memorable quote from Weber ([1921] 1968, p. 23): “Thus, if at thebeginning of a shower a number of people on the street put up their umbrellas at thesame time, this would not ordinarily be a case of action mutually oriented to that ofeach other, but rather of all reacting in the same way to the like need of protectionfrom the rain.”4 In this article, we use the term “marketing efforts” to denote the range of activitiesthat a supplier engages in to further the sales of its product. Apart from developingappealing products, marketing efforts include impersonal marketing communication(advertising and direct mail), personal selling (termed “detailing” in the pharmaceuticalindustry), obtaining free publicity, and managing pricing and distribution (e.g., Bagozzi1986; van Waterschoot and Van den Bulte 1992).
antibiotic tetracycline among physicians in four communities in the Amer-ican Midwest during the mid-1950s. It is often credited with documentinginnovation diffusion as a social process in which adoption is driven bysocial contagion (Rogers 1995). The study has more than just historicalinterest, though. Its data on the diffusion of tetracycline have become “astrategic research site for testing new propositions of how social structuredrives contagion” (Burt 1987, p. 1301) and for assessing the performanceof new modeling techniques (Marsden and Podolny 1990; Strang andTuma 1993; Valente 1996). While recent reanalyses of the data have foundsocial contagion effects to be rather small (Burt 1987; Burt and Janicik1996), sensitive to model specification (Strang and Tuma 1993), or eveninsignificant (Marsden and Podolny 1990), these reanalyses were primarilydesigned to investigate which social contagion mechanism was operating(information sharing among cohesive actors vs. competitive mimesisamong positionally equivalent actors) or to assess the performance of newmodels in capturing contagion patterns in the data. With such objectives,previous reanalyses assumed that contagion was truly at work. Therefore,none started with a detailed account of how the market for the new drugoperated nor included variables capturing time-dependent nonnetworkmechanisms.
We present our argument in two steps. We first describe the medical
community’s understanding of antibiotics and sources of drug informationat the time the data were originally collected. From this description, weconclude that social contagion is unlikely to have been a key driver inphysicians’ decision to adopt, but that the pharmaceutical companies’marketing efforts may have played a considerable role. Next, we test thisconjecture empirically by applying hazard models to the Medical Inno-vation data set, which we have supplemented with new data on adver-tising. Our results indicate that previous evidence of social contagion wasspurious. Given the significance of Medical Innovation in the diffusionliterature, our findings underscore the risk of confounds in research onsocial contagion in innovation diffusion.
SITUATIONAL ANALYSIS OF TETRACYCLINE AND THE MEDICALCOMMUNITY
Medical Innovation is a study of the adoption of tetracycline, a broad-spectrum antibiotic, by 125 physicians in four small cities in Illinois. Atthe time that Lederle launched the first tetracycline-based product inNovember 1953, three other broad-spectrum antibiotics were already onthe market. Lederle had introduced chlortetracycline in 1948, Parke-Davishad introduced chloramphenicol in 1949, and Pfizer had introduced oxy-
tetracycline in 1950. To better understand the situation physicians foundthemselves in when deciding whether or not to adopt the new drug, weanalyze the product’s characteristics, the way it was commercialized, andthe kind of sources of information and influence physicians in the 1950stypically used.
The diffusion literature suggests that an innovation’s rate of adoption isaffected by potential adopters’ perceptions of five critical characteristics:complexity, compatibility with existing values, trialability, observabilityof results, and relative advantage over alternatives (Rogers 1995). Tet-racycline had product characteristics typically associated with rapiddiffusion. Low complexity.—Tetracycline was chemically similar to two existing
and successful antibiotics, as evidenced by their generic names. Thougha new compound, tetracycline “was merely the newest in an already es-tablished family of drugs,” and an “undramatic pharmaceutical innova-tion” (Coleman et al. 1966, pp. 17, 36). Compatibility.—Physicians were favorably disposed toward the phar-
maceutical industry, its new products, and efforts to market them (BenGaffin 1959; Caplow and Raymond 1954). Enthusiasm was particularlystrong for antibiotics (Peterson et al. 1956).5
Trialability and observability of results.—Broad-spectrum antibiotics
were generally used in the treatment of acute, rather than chronic,conditions. Because of the short time between treatment and outcome, aphysician could easily and quickly determine drug efficacy in anyparticular case and adjust the therapy if necessary (Coleman et al. 1966,p. 17). Relative advantage.—Tetracycline produced fewer side effects than the
other three broad-spectrum antibiotics (Pearson 1969). Tolerance and sideeffects had become a very important issue by the time tetracycline waslaunched. In the summer of 1952, the side effects of chloramphenicol,
5 Peterson et al. (1956) intensively studied 88 general practitioners in North Carolina,each over a period of three to three-and-a-half days. They often observed the physiciansimmediately prepare an injection of penicillin upon learning that the patient had afever. This decision was frequently reached before the patient had been examined. Two-thirds of the physicians gave antibiotics to all patients suffering from respiratoryinfections without attempting to determine whether the infection was viral or bacterial(antibiotics are ineffective against viral infections). Also, “it was apparent from ob-servation and statements from physicians that their practices in regard to medicationsand therapy are influenced significantly by the information and products supplied bythe drug salesman” (p. 103).
marketed under the brand name Chloromycetin, received wide press cov-erage. A June 28 editorial of the Journal of the American Medical As-sociation (JAMA) called doctors’ attention to reports on Chloromycetin’sside effects, and on July 3 the American Medical Association issued apress release—“AMA Warns Doctors on Chloromycetin Therapy”—thatreceived wide coverage in the popular press. Finally, the FDA even with-drew the drug’s certificate, organized its own field survey, and turned itsreports over to the National Research Council for review. On August 14,the drug was allowed back on the market, although Parke-Davis wasordered to print prominently on its labels the dangers inherent in its use(Fortune 1953; Pearson 1969). As a result of these problems, Chloromy-cetin’s share of the broad-spectrum antibiotics market declined to 5% inOctober 1952, down from 38% four months earlier. In September 1953,two months before Lederle’s launch of tetracycline, Chloromycetin’s sharewas still at only 10% (Fortune 1953). Thus, tetracycline had a competitiveadvantage on a product dimension that was especially salient at the timeof its launch.
In sum, tetracycline’s characteristics present strong reasons to expect
rapid diffusion. Also, there is little reason to expect social contagion tohave been important. Since there was little ambiguity or perceived riskin prescribing tetracycline, information from previous adopters should nothave affected physicians’ evaluation of the drug in a major way. Sincetetracycline was merely the newest member of an already establishedfamily of drugs and an undramatic innovation, it is also questionable thatadopting it would have markedly enhanced physicians’ status among theirpeers.
An analysis of the potential adopter’s situation should also include a viewof the supply side. In this section, we document characteristics that havebeen found to be associated with rapid diffusion (e.g., Bauer 1961; Hahnet al. 1994): the intensity of competition among suppliers, the reputationof suppliers among potential adopters, and the marketing efforts ofsuppliers.
In contrast to other broad-spectrum antibiotics, tetracycline did not
enjoy exclusive patent protection. After a tumultuous episode of litigation,the parties involved worked out a complex patent sharing and licensingagreement, giving Lederle, Pfizer, and Bristol the right to manufactureand sell the drug and allowing Squibb and Upjohn to sell the drug undera supply contract with Bristol (FTC 1958, pp. 245–57). These five firmsaccounted for more than half of all the antibiotics sold in the United
States in 1950, and all had a good reputation within the medical com-munity (FTC 1958).
Lederle, the first company to launch a tetracycline formulation, de-
ployed a very aggressive marketing program for its tetracycline brandAchromycin. Coleman et al. (1966, pp. 44, 181) mention the “blanketexposure of all doctors to the detail man [i.e., pharmaceutical represen-tative visiting physicians].” Lederle’s direct mail budget for tetracyclinepermitted 105 mailings, an average of two per week, to every physicianin the United States during its first year of commercialization. Medicaljournal advertising for the first 12 months consisted of 26 insertions inJAMA and monthly insertions in the highly circulated Modern Medicineand Medical Economics, as well as in all state journals, 116 county jour-nals, and most specialty journals (FTC 1958). Tetracycline also receivedwide positive coverage in the professional media (Ben Gaffin and Asso-ciates [1956] 1961b). As a detail man remarked, “Lederle was interestedin bombarding physicians with the Achromycin name and we did justthat and got the name across. We swamped them with Achromycin” (FTC1958, p. 130). Pfizer was much less aggressive in pushing tetracycline,fearing that strongly promoting its own brand of tetracycline, Tetracyn,would undercut its sales of oxytetracycline. Only in January 1955, possiblyalarmed by the tremendous success of Lederle’s Achromycin, did Pfizerstart to market Tetracyn more aggressively (Mines 1978). We have nodetailed information on how aggressive the other three players marketedtheir own tetracycline brand. They did not face the same fear of productcannibalization as Pfizer did, and they appear to have been more ag-gressive than Pfizer, though they lacked the resources to be as aggressiveas Lederle (Pearson 1969).
Tetracycline was not only extensively promoted, but also aggressively
priced. Although the product was superior to other broad-spectrum an-tibiotics, its price to consumers was the same as that of the three othertypes of broad-spectrum antibiotics (FTC 1958). To the extent that phy-sicians took price into consideration in their prescription behavior, tet-racycline pricing would have favored rapid adoption.
In sum, tetracycline was marketed by a small group of companies en-
joying a solid reputation. The first company to enter the market, Lederle,deployed a very intensive marketing campaign. The product also enjoyeda large amount of free publicity. Although superior in therapeutic effects,the product did not carry a price premium. Such a market environmentis conducive to rapid initial diffusion (Bauer 1961; Hahn et al. 1994),irrespective of social influence among physicians.
Exposed to such intensive marketing efforts, physicians did not need
word of mouth from their colleagues to become aware of the product’sexistence and purported benefits. Coleman et al. (1966, pp. 13–14) argued
that the physicians’ problem was not too little but too much information. Social contagion, then, need not have operated by creating awareness butby physicians’ turning to their colleagues as a way to cope with infor-mation overload. Physicians who already had adopted may then have ledothers to evaluate the new drug positively. However, such a simplifyingcognitive strategy is necessary only if actors experience ambiguity or un-certainty, a condition that appears to have been unlikely. While there wasindeed a deluge of information, it all pointed in the same direction: infavor of adopting tetracycline.
A number of studies provide insight into the relative importance of thephysicians’ various sources of information about new drugs around thetime of the tetracycline study. Many of these studies were conducted inthe Midwest or in relatively small cities and can thus be expected to berepresentative of the four Illinois towns studied in Medical Innovation.
A 1952 survey of midwestern physicians reported that they found detail
men, direct mail, journal articles, and journal advertising to be muchmore important sources of information than their colleagues (Caplow andRaymond 1954). Menzel and Katz (1955) conducted the pilot study forMedical Innovation in a New England city of comparable size to the fourcities in the main study. They also found that physicians rated colleaguesas less important than detail men, articles in journals, and direct mail. Astudy of the diffusion of Lederle’s Achromycin brand in another smallmidwestern city found similar results (Ben Gaffin and Associates 1961b),as did Ferber and Wales (1958), using a sample of Chicago physicians,and Winick (1961) in a study of an ethical drug introduced in 1957. National scale studies by the National Opinion Research Center (Hawkins1959), Ben Gaffin and Associates (1959), and Harris (1966) reported similarfindings as well. All these studies indicate that physicians in the 1950stypically did not report peer influence as an important information sourcefor new pharmaceuticals but noted commercial communication effortsand medical journals to be more important and more valuable.
Overall, tetracycline’s product characteristics, the way it was marketed,and the sources of information physicians typically used for adoptiondecisions do not paint a case for strong contagion effects. Table 1, recon-structed from original reports on the Medical Innovation study, showsthat physicians considered colleagues to be a source of information andinfluence, but not a very important one.
Doctors’ Reported Sources When Adopting Tetracycline
Detail men . . . . . . . . . . . . . . . . .
Journal articles . . . . . . . . . . . .
Direct mail . . . . . . . . . . . . . . . .
Colleagues . . . . . . . . . . . . . . . . .
Meetings . . . . . . . . . . . . . . . . . . .
All other media . . . . . . . . . . .
* Based on Katz (1961, p. 77). A cross-check against the Medical Innovation network data set prepared
by Burt (1986) indicates that the base for these percentages are the 141 physicians (out of a total of 216interviewed after the 12 exploratory interviews) whose most recent adoption was tetracycline.
Based on Coleman et al. (1966, p. 59). Data were available for 87 adopters, who generated 131
mentions of sources intermediate to first and last source. Thus, the base for the percentages in the firstand third column is 87; for those in the middle the base is 131.
One might raise the following questions: If advertising and detailing
were indeed as important as our situational analysis suggests, would Cole-man et al. not have taken these factors into account? Does the fact thatthey did not include these factors in their analysis not reduce the facevalidity of our own conclusions? We do not believe so. In appendix A,we document that the way Medical Innovation came about may haveled its authors away from looking into the effects of detailing and journaladvertising. Appendix A also presents a reminiscence by Coleman indi-cating that he and his fellow authors may not have been very familiarwith the institutional details of their research site.
STATISTICAL ANALYSIS INCORPORATING MARKETING EFFORT
Our description of the medical community’s understanding of tetracyclineand of physicians’ sources of information indicates that marketing effortsby the drug manufacturers, and especially Lederle, may have been keydrivers of the diffusion process. Earlier analyses, however, have ignoredthis factor, and their results may therefore have been based on a confound. We investigate this possibility empirically below.
We assume that to adopt, physicians must both be aware of the innovationand evaluate it positively. Using insights from social network threshold
modeling, we assume that awareness and utility thresholds may vary asa function of physician characteristics (Erikson 1998; Granovetter 1978;Hedstro¨m 1994; Valente 1996). Awareness can be driven by marketingefforts (such as sales calls by detail men and advertising), free publicityin medical journals, and exposure to peers who have adopted previouslyand with whom one shares information on medical practice. Marketingefforts, free publicity, and social contagion can also affect evaluation.
We assume that social contagion stems from exposure to alters who
have already adopted and that it operates over personal relationships. This social influence may take the form of information transfer, makingone aware of the existence of the drug or improving one’s evaluation ofthe drug’s therapeutic merits. Social influence may also consist of socialnormative pressure: to maintain attitudinal balance, one may feel com-pelled to adopt once many of one’s direct peers have done so. Our datawill not allow us to distinguish between these two “social cohesion” pro-cesses, but we will distinguish them from social influence operating ascompetitive mimicry of structurally equivalent colleagues who a physicianfeels compelled to imitate for fear of losing status in the community (cf. Burt 1987). Our inability to operationalize uniquely each social contagionmechanism is not important, as our purpose is not to distinguish betweenalternative theories positing each type of process, but rather to distinguishbetween social contagion and contextual effects, specifically marketingefforts measured through advertising volume.
We use discrete-time hazard modeling to relate explanatory variablesto adoption behavior (Allison 1982). Operationalizing social networkexposure through lagged endogenous autocorrelation terms (cf. Hedstro¨m1994; Strang 1991), we represent the hazard of adoption of physician i attime t as
p 0) p F(a x ϩ bS w y
where y p 1 if i has adopted by time t, and y p 0 otherwise; F is a
cumulative distribution function; x is a vector of variables affecting i’s
decision to adopt, irrespective of any influence from colleagues (the vectorincludes an intercept, a summer dummy, physician characteristics, andtwo advertising variables, which are described below); w is social ex-
posure of physician i to physician j (described below); a, b are a vectorof parameters and a parameter to be estimated, respectively. Discrete-time hazard models are appropriate here because several adoptions occurin each observation period. Van den Bulte and Lilien (1999) show thatthese statistical models also have the theoretically attractive property that
they can be derived from both random utility theory and random socialnetwork threshold models.
Coleman et al. (1966) provide a detailed description of the population,the sample, and data collection procedures. Burt (1986) placed the portionof the original data set that we use in the public domain. Since the dataare publicly available, we limit our discussion to the variables we usedor constructed for our own analysis. Physician characteristics.—We included five covariates to account for
heterogeneity in physicians’ tendency to adopt early. Professional age mea-sures (on a 1–6 scale) how long ago the physician graduated from medicalschool. We included both a linear and a quadratic term to account for apossible inverse U-shaped relationship between professional age and in-clination toward adoption: compared to midcareer physicians, older phy-sicians may be more conservative and very inexperienced physicians moreaverse to risk. We mean-centered age to reduce collinearity. We used thenumber of journals a physician receives or subscribes to as a measure ofmedia exposure. Journals included both newsletters sent by pharmaceu-tical companies and scientific and professional publications. We used thelogarithm to reflect decreasing returns to scale. We expected physicianshaving a chief or honorary position in their hospital, captured as a dummyvariable, to be less involved in actual medical practice than were activeor regular staff, and hence more likely to adopt later. We also includedan attitudinal measure, scientific orientation, coded as “1” if the physicianagreed with the statement that it is more important for a physician to“keep himself informed of new scientific developments [than to] devotemore time to his patients,” and “0” otherwise.
We also estimated models including the number of nominations a phy-
sician received as advisor or as discussant as measures of status. Althoughsociometric status figures prominently in the analysis by Coleman and hisassociates, it did not contribute significantly to model fit, nor did it changethe coefficients of the contagion variables once we controlled for the num-ber of journals received. Burt (1987), Marsden and Podolny (1990), andStrang and Tuma (1993) reported similar findings. It appears that opinionleaders adopted early as a result of their cosmopolitan perspective andmedia habits rather than due to pressure to maintain their status amongtheir colleagues. We report results only for models excluding sociometricstatus variables. Seasonal effects.—We included a seasonal dummy variable for the sum-mer months of July and August. We expected fewer adoptions of a newantibiotic in these two months because the weather is warmer and schools
are closed, limiting the spread of contagious diseases and in turn thedemand for antibiotics (Cliff et al. 1981). Advertising volume.—The Medical Innovation data do not contain in-
formation on the amount of marketing effort targeted toward the phy-sicians whose prescriptions were tracked. We use the number of adver-tising pages in three leading advertising outlets, Modern Medicine,Medical Economics, and GP, as our measure of marketing effort. Thesethree publications were preferred by pharmaceutical advertisers and werewidely read by physicians in the 1950s (Ben Gaffin and Associates [1953]1961a, 1961b). Our attempts to collect data on the number of ads ap-pearing in JAMA were unsuccessful, as librarians removed the advertisingsupplement before binding the issues for storage.
We distinguish between the marketing efforts by the first entrant, Led-
erle, and those of the later entrants. We do so for two reasons. First, thefirst entrant’s marketing efforts are often more effective than those oflater entrants when the latter do not offer an important therapeutic ad-vantage (Bond and Lean 1977; Hurwitz and Caves 1988; Shankar, Car-penter, and Krishnamurthi 1998). Second, Lederle had a very large salesforce and was strongly committed to building a dominant position ag-gressively while other companies were less well endowed and lessaggressive.
We matched the number of advertisements in each issue to the four-
week sampling periods in the data set prepared by Burt (1986). Becausethe data are monthly observations and because previous research in thepharmaceutical industry documents the presence of sizable spillover ef-fects over time (Berndt et al. 1997; Montgomery and Silk 1972; Rangas-wamy and Krishnamurthi 1991), we expected marketing communicationeffects to span multiple periods. We therefore constructed measures ofdepreciation-adjusted stock of marketing effort (Berndt et al. 1997; Kalishand Lilien 1986; Rizzo 1999). Let m be the amount of advertising in
month t (in hundreds of pages), and let d be the monthly decay rate(0 ≤ d ≤ )
1 . The stock of marketing effort M is then defined as
We constructed one such variable for Lederle and one for all other com-petitors combined. We assumed that the decay parameter d (to be esti-mated) was equal across companies.
We have not been able to locate data on the amount of detailing effort
by various companies marketing tetracycline, but we do not believe thisto be a problem. Detailing effort and journal advertising are so highlycorrelated in pharmaceutical markets that either variable can be used to
represent overall marketing effort (Berndt et al. 1997; Gatignon, Weitz,and Bansal 1990; Lilien, Rao, and Kalish 1981; Rangaswamy and Krish-namurthi 1991; Rizzo 1999).
We do not include interaction effects between marketing effort and the
number of journals received. While such interactions would normallyprovide a sharper test of advertising effects, they would be unlikely todo so in this case because the journal subscription variable does notdiscriminate between exposure to commercial and scientific content. Nordoes it distinguish scientific journals, Lederle’s newsletter, and competi-tors’ newsletters from one another. We see no reason why a physicianwith above-average exposure to the scientific information in medical jour-nals and company-specific newsletters would have been differentially sen-sitive to advertising or visits by detail men. Nor do we see a reason whythe effectiveness of Lederle’s advertising would have been boosted amongphysicians who received many newsletters or were exposed to many jour-nal advertisements, not only from Lederle but also from its competitorshaving a stake in promoting other broad-spectrum antibiotics. A similarargument applies for the later entrants. Another reason not to expect asignificant interaction between journal subscriptions and later entrants’marketing efforts is that the latter’s effectiveness is likely to be low overall(Bond and Lean 1977; Hurwitz and Caves 1988; Shankar et al. 1998),resulting in a floor effect precluding the detection of significant interactioneffects.6
Contagion variables.—We define the social influence that physician i
is subject to at time t as a function of whether other physicians ( j) haveadopted previously (indicated by yj is to i (indicated by the social weight w ). The extent of social network
exposure i is experiencing can then be expressed as a lagged networkautocorrelation variable S w y
Strang 1991). The actual social contagion, that is, influence on adoptionbehavior, is then bS w y
Coleman et al. (1966) had 228 physicians interviewed. Each physician
was asked to name up to three other physicians with whom he discussedmedical practice, and up to three physicians from whom he sought adviceabout medical practice. However, Coleman et al. had prescription datacollected only for general practitioners (N p 125) and not for specialists. There are two approaches to this missing data problem. Burt (1987) and
6 To check these a priori reservations, we performed analyses including interactionterms between number of journals received and marketing stock of both Lederle andthe other entrants. As expected, the interaction terms were not significant (P 1
The point estimates and significance test of all the other parameters were strikinglysimilar to those reported below in this article. Detailed results of these additionalanalyses are not reported here but are available on request from the authors.
Marsden and Podolny (1990) assumed that the adoption of tetracyclineby specialists affected generalists’ decision to adopt; consequently theseauthors imputed adoption dates for specialists (though they only analyzedthe generalists’ adoptions). In contrast, Coleman et al. (1966) and Strangand Tuma (1993) assumed that generalists did not take specialists’ adop-tion behavior into account; these authors thus do not consider the latter’smissing adoption data when constructing the social influence variables. We used both approaches, as Strang and Tuma (1993) suggested thatdifferent assumptions about the effects of specialists on generalists mayhave caused different reanalyses to find evidence of social contagion ornot.
We constructed two types of exposure variables, each assuming a dif-
ferent influence mechanism represented by the w weights. The direct ties
weights reflect whether i nominated j as an interaction partner for adviceor discussions, such that i might have gained information or experiencedsocial normative pressure from j. We also constructed weights of structuralequivalence indicating whether i might mimic j out of fear of losing outin the competition for status. We operationalized structural equivalenceas the proportion of exact matches between two physicians’ set of rela-tionships with third parties: thus, the more their portfolio of relationshipsoverlap, the higher the weight they give to one another. Appendix B detailshow we constructed the network exposure variables S w y
We also used the network exposure variables constructed by Burt
(1986): one captures word of mouth operating over direct ties and onecaptures competition for status between structurally equivalent physi-cians. Burt incorporated specialists’ imputed adoption data in his exposurevariables. He also used different operationalizations of the influenceweights than we did. Because of imputation problems, Burt could notcompute exposure to structurally equivalent colleagues for seven physi-cians. For one of these seven, Burt was also unable to compute a measureof social cohesion influence. For these few physicians, we substituted ourmeasures of influence through structural equivalence and direct ties forBurt’s missing values.
After constructing the variables, we deleted four physicians, due to
missing covariates. The data set for estimation contains 17 monthly ob-servations for 121 individuals, 105 of whom had adopted by the lastobservation period. Table 2 presents descriptive statistics for the data,after excluding postadoption observations irrelevant to explain adoption.
Figure 1 graphs the cumulative proportion of physicians having
adopted in each period (p S w y , assuming perfect social mixing, i.e.,
w p 1/N for all i and j where N is the number of actors) as well as the
marketing stock M of Lederle and the other entrants. The graph shows
that the cumulative fraction of adopters, a rough proxy for average net-
Descriptive Statistics of Model Variables
1. y (adoption indicator) . . . . . . . . . . . . .
2. Summer . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3. Age . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4. Age2 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5. Journals (log) . . . . . . . . . . . . . . . . . . . . . .
6. Science . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7. Chief . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8. Direct ties . . . . . . . . . . . . . . . . . . . . . . . . . .
9. Structural equivalence . . . . . . . . . . . .
10. Direct ties (Burt) . . . . . . . . . . . . . . . . .
11. Structural equivalence (Burt) . . .
12. Advertising by Lederle . . . . . . . . . .
.12 Ϫ.17 Ϫ.19 .05 .68 .80 .69 .75 . . .
13. Advertising by others . . . . . . . . . . . .
Note.—Items 8 and 9 utilize our data; items 10 and 11 utilize data from Burt (1986).
Fig. 1.—Adoptions and marketing stock; marketing stock is defined as the depreciation-
adjusted cumulative advertising volume (see eq. [2]).
work exposure, closely tracks Lederle’s marketing stock, hence suggestingthe threat of a confound. Figure 2 graphs the empirical hazard rate, thatis, the number of physicians adopting in period t divided by the numberof physicians not having adopted prior to period t, together with the twomarketing stock variables. The hazard rate increases with Lederle’s mar-keting stock between periods 2 and 7. As Lederle’s marketing stock flat-tens, the hazard begins to behave more erratically. It even drops in periods9 and 10 (July–August 1954), possibly due to the summer effect. Thehazard rate picks ups again between periods 10 and 15, which coincideswith increased marketing efforts by later entrants, but the increase isirregular and not sustained after period 15. Figure 2 suggests that mar-keting efforts, especially by Lederle, may have been associated withadoption.
We used both logit and probit specifications and estimated our modelsusing maximum likelihood, with one exception. We estimated the mar-keting effort decay parameter d using a grid search (cf. Berndt et al. 1997)in a model that did not feature social network exposure variables. A valueof d p 0.25 led to the highest model likelihood. Model fit was not verysensitive to changes in the range between 0.15 and 0.30. In subsequentanalyses of models featuring both marketing effort and social networkexposure, we kept d fixed at 0.25.
We checked for unobserved heterogeneity in both probit and logit mod-
Fig. 2.—Empirical hazard rate and marketing stock. The broken lines around the em-
pirical hazard rate indicate the SE interval (ϩ/ Ϫ 1). We computed SEs using a logit hazardmodel. The interval is not symmetric because the logit model is linear in the log odds ofthe hazard rate, not in the hazard rate itself.
els. In the probit models, we estimated a normal mixture while allowingthe base hazard to vary freely every three months (cf. Han and Hausman1990). In the logit models, we used the score tests developed by Hamerle(1990) and Commenges et al. (1994). None of these tests suggested thepresence of significant unobserved heterogeneity (P 1 0.10). We presentthe results for the logit specification only and omit the test statistics forunobserved heterogeneity.
Table 3 reports the results for each of the four social network exposurevariables: two for exposure through direct ties (both our own and Burt’smeasure) and two for exposure through structural equivalence (again ourown and Burt’s measure). The four first columns (1a–4a) report the logitcoefficients in models without marketing effort. Social contagion is sig-nificant in all four cases. Exponentiating the social contagion coefficientsreported in table 3 indicates that the odds of adoption by someone withmaximum exposure was two to three times the odds of adoption by some-one without any social network exposure. Also, the coefficients of allphysician characteristics except for age have the expected sign and aresignificant at 90% confidence or higher. Age does not have the expected
Empirical Proof That Marketing Effort, Not Social Contagion, Is Associated with Adoption Behavior
Intercept . . . . . . . . . . . . . . . . . . . . . . .
Ϫ3.48**** Ϫ3.69**** Ϫ3.82**** Ϫ3.78**** Ϫ4.46**** Ϫ4.31**** Ϫ4.14**** Ϫ4.14**** Ϫ4.42****
Summer . . . . . . . . . . . . . . . . . . . . . . . .
Professional age . . . . . . . . . . . . . . .
Professional age2 . . . . . . . . . . . . . . N of journals (log) . . . . . . . . . . . .
Scientific orientation . . . . . . . . . .
Social contagion . . . . . . . . . . . . . . . . .
Lederle . . . . . . . . . . . . . . . . . . . . . . . . .
Others . . . . . . . . . . . . . . . . . . . . . . . . . .
Note.—Results are logit coefficients from discrete-time hazard models. Models are defined as follows: 1a, 2a, 1b, and 2b contain direct ties; 3a, 4a, 3b, and 4b contain
structural equivalency; 5 contains no contagion. Models 2a, 2b, 4a, and 4b use Burt’s measure; remaining models use our measure.
* P ! .10, two-sided test. ** P ! .05. *** P ! .01. **** P ! .001.
positive sign, suggesting that younger physicians did not delay adoption. The summer dummy variable has the expected negative sign, but is notor is only marginally significant.
The next four columns (1b–4b) report the results for models incorpo-
rating marketing efforts. Adding the marketing variables improves modelfit substantially in all four cases. The coefficients of the physician char-acteristics barely change, but the social contagion effects are now allinsignificant. As expected from our situational analysis, marketing effortsby Lederle affect adoption more than peer influence or marketing effortsby later entrants, neither of which show a significant effect. Finally, amodel with marketing effort but without social network exposure fitsabout equally well as models with both types of variables (col. 5). Overall,the results indicate that Lederle’s marketing efforts, not social contagion,was the dominant driver increasing physicians’ hazard of adoption overtime.
Though we believe that our description of the physicians’ situation at thetime the data were collected is accurate and that our statistical analysissupports its predictions, the latter involves both modeling compromisesand data restrictions. First, we limited our analysis to interpersonal in-fluence associated with others’ past behavior and did not consider others’contemporaneous or anticipated future actions. By ignoring contempo-raneous actions, we fail to capture possible joint decision making amongphysicians. By ignoring how physicians may have anticipated adoptionsof their peers and how this in turn may have led them to adopt preemp-tively to maintain their status within their community, we may not havecaptured competitive contagion fully. Even though our descriptive anal-ysis suggests contemporaneous social contagion and prospective behaviorwere unlikely to be important for tetracycline, we did not assess theseeffects in the statistical analysis. There are both statistical (Besag 1975)and theoretical problems (Coleman 1990) that need to be resolved beforeconsidering empirically analyzing the effects of contemporaneous and an-ticipated actions in complex, nonrandom network structures.7
Second, our analysis is constrained by the lack of richness in the data
7 Strang and Tuma (1993) do model contemporaneous contagion. Their estimationprocedure, however, does not account for the interdependence among observationsexplicitly present once one allows for contemporaneous contagion. Traditional likeli-hood functions for binary dependent variable models, which include discrete-timehazard models used in the present study, do not account for this endogeneity. Includinga contemporaneous network exposure variable, S w y , would lead to invalid results
about what gets communicated through the network. We assume thatsocial interaction informs potential adopters only about others’ adoption,not their expected or achieved utility, attitudes, or other evaluations. Thisis defensible when actors do not discern internal states or outcomes ofothers. Sometimes, however, outcomes are actually communicated byadopters (e.g., satisfaction) or can be observed (e.g., market share gainsor increased fundraising by organizations that implement a new tech-nology). Researchers having such data available can modify the modelquite easily by substituting the relevant variable (say, q ) for the y
indicator and compute network exposure as S w q .
Third, our hazard models do not distinguish between two important
stages in the adoption process: awareness followed by evaluation that isitself conditional upon awareness (Rogers 1995). Such separation may helpgain a better understanding of the differential effects of advertising andsocial contagion, as the former is believed to operate mainly early in thedecision process and the latter mainly in later stages (Rogers 1995). Mod-eling the effect of marketing efforts and social contagion without distin-guishing between awareness and evaluation might produce misleadingresults when marketing efforts are quite important in creating awarenessand when social contagion is moderately—though still sizably—importantin persuading actors to adopt the innovation. When both explanatoryvariables are forced into a single-stage model, the weaker social contagioneffect may be washed out by the marketing effort, erroneously suggestingthat social contagion was not at work.
These three caveats mean that both our analysis and those that preceded
it may not have been able to identify very subtle social contagion processesaffecting the diffusion of tetracycline. Yet, the caveats apply to our ownanalysis as well as earlier ones and hence do not affect the main impli-cation of our statistical analysis: prior evidence of social contagion in theMedical Innovation data was based on confounding the contextual effectof Lederle’s aggressive marketing efforts with social contagion.
Our results about the absence of network effects once one controls for
advertising clearly contradict the received view of strong network effectsin Medical Innovation (Rogers 1995). At the same time, they also explainthe “weak” results obtained by Marsden and Podolny (1990) and Strangand Tuma (1993). Marsden and Podolny estimated a Cox proportionalhazard model, which is very similar to a discrete-time logit hazard modelwith a dummy variable for each time period. These dummies capture allcross-temporal variation in the mean adoption hazard and leave onlyvariance within particular time periods to be explained by network ex-posure. Strang and Tuma incorporate lagged penetration as a covariate,besides lagged network terms. Lagged penetration assumes that any phy-sician interacts with any other physician (i.e., a constant w for all i and
j), ignoring network structure but capturing the cross-temporal variationin average network exposure. Similarly, our marketing variables vary overtime but not across physicians. Hence, all three studies show that differ-ences in adoption across physicians within any particular time period arenot statistically significantly associated with differences in lagged socialnetwork exposure. Our study, however, is the only one to provide anexplanation for this finding grounded in a detailed situational analysis.
Based on a situational analysis of the medical community’s understandingof tetracycline in the mid-1950s and on a new statistical analysis, weconclude that Medical Innovation (Coleman et al. 1966) and several sub-sequent studies that analyze the diffusion of tetracycline have confoundedsocial contagion with marketing effects. Our analysis of the drug’s char-acteristics, the way it was marketed, and the typical sources of informationwithin the medical community, suggest that it is unlikely that social con-tagion processes were important in physicians’ decision to adopt, but thataggressive marketing efforts by Lederle may have had a significant im-pact. A new statistical analysis of the Medical Innovation data set, sup-plemented with newly collected data on advertising volume (a measureof marketing effort), shows that contagion effects disappear once we con-trol for marketing effort. Hence, we conclude that the data do not doc-ument that diffusion was driven by contagion operating over social net-works and that earlier analyses confounded social contagion with theeffect of marketing effort.
The danger of confounding common contextual effects with social con-
tagion has been repeatedly discussed in the literature. Yet, given the prom-inence of the original Medical Innovation study and subsequent reana-lyses of the data (esp. Burt 1987) in the diffusion and social networkliteratures, our results are particularly noteworthy: they underscore, morecompellingly than general methodological admonitions, that the dangerof confounds when studying the role of social contagion in innovationdiffusion must not be taken lightly. Medical Innovation’s Silence Does Not Mean Marketing Efforts WereIrrelevant
The authors of Medical Innovation did not pay much attention to mar-keting factors in their analysis. This oversight does not reduce the facevalidity of the conculsions of our situational analysis: Medical Innova-tion’s genesis may have led its authors away from looking into the effectsof detailing and journal advertising, and the authors may not have beenvery familiar with all the institutional details of their research site. The genesis of the original study.—Medical Innovation started off as
an advertising effectiveness study for Pfizer, one of the sponsors of PaulLazarsfeld’s Bureau of Applied Social Research at Columbia University. As reported by a former affiliate to the bureau, Pfizer “wanted to find outwhether or not it should continue to advertise a new drug in the Journalof the American Medical Association” (Glock 1979, p. 27). Typical of thescholarly entrepreneurship with which Lazarsfeld funded his institute,this rather humdrum marketing question was converted into a sociologicalstudy of scholarly interest showing very little surface traces of its mer-cantile origins (Rogers 1994). It is important to note that, in those days,Pfizer did not place ads in the regular advertising section in JAMA, buthad its own newsletter, Spectrum (that contained both ads and articles),inserted in each issue of JAMA. This, we believe, explains why the studyincludes multiple questions about specific newsletters and about JAMAbut none about regular journal advertising or other medical journalsmentioned by name (the questionnaire is reprinted in Coleman et al. 1966,pp. 195–205). The genesis of Medical Innovation as a study on the ef-fectiveness of drug house newsletters redefined into a diffusion study alsoexplains the rather small amount of attention given to detailing as a sourceof influence. Familiarity with the research setting.—Consider the following 1993
reminiscence by James Coleman of the Medical Innovation project:
I never saw the communities. It [Medical Innovation] was one of thoseresearch projects that happens while you are busy with more importantprojects. I designed the research with Herb [Menzel] and Elihu [Katz]. Herband Elihu reviewed the literature on medical innovation. A team of inter-viewers came out to Illinois from the Bureau to talk to the doctors, andSidney Spivik searched the prescription records. The questionnaires wentback to Columbia to be keypunched, a set of cards were sent to me foranalysis, and the research report was published in Sociometry [1957]. (Ascited in Burt 1997; square brackets added by Burt)
This recollection indicates that neither Coleman nor his two coauthorshad firsthand knowledge of medical practice in the four Illinois com-munities. Hence, the fact that Medical Innovation does not emphasizethe role of marketing efforts in the diffusion of tetracycline cannot beused to infer that those efforts were unimportant.
Procedures Used to Create Social Influence Weights
Our analysis uses both discussion and advice relationships. Using thenetwork data of all 228 physicians, we constructed the social weight ma-trices for each of the four cities separately in a series of steps. Step 1.—First, we created adjacency matrices with element a p 1 if
i mentions j; 0 otherwise. We created two such adjacency matrices foreach city: one for discussion ties and one for advice ties. Step 2.—Since being discussion partners is a naturally reciprocal re-
lationship, we symmetrized the discussion adjacency matrix (Alba andKadushin 1976). Step 3.—We constructed a pooled adjacency matrix by adding the sym-
metrized discussion matrix and the advice matrix, treating discussion andadvice as indicators of a common underlying variable “interacting with.”We also performed analyses (not reported here) keeping discussion andadvice separate. This separation did not affect the results. Step 4.—We constructed two different weight matrices to account for
various network contagion mechanisms. Direct tie matrices are identicalto the adjacency matrices. We computed structural equivalence weightsas the proportion of exact matches between two physicians’ set of rela-tionships with third parties. A valid match required that the physicianshad at least one common third party, which implies that actors withoutany common third party did not put any weight on each other’s actions. Step 5.— We deleted all rows and columns referring to physicians who
were not among the 125 included in the prescription sample. Step 6.—We put all diagonals to zero and normalized all rows such
S w p 1, if and only if w ( 0 for some j, and
S w p 0 otherwise. This row normalization implies that physicians are
sensitive to the proportion rather than the number of relevant others whohave adopted, and it ensures that each network exposure variable isbounded between zero and one.
After performing these six steps, actor i’s social network exposure at
time t can be computed as S w y
Alba, Richard D., and Charles Kadushin. 1976. “The Introduction of Social Circles:
A New Measure of Social Proximity in Networks.” Sociological Methods andResearch 5:77–102.
Allison, Paul D. 1982. “Discrete-Time Methods for the Analysis of Event Histories.”
Pp. 61–98 in Sociological Methodology, edited by Samuel Leinhardt. San Francisco:Jossey-Bass.
Bagozzi, Richard P. 1986. Principles of Marketing Management. Chicago: Science
Bandura, Albert. 1986. Social Foundations of Thought and Action: A Social CognitiveTheory. Englewood Cliffs, N.J.: Prentice-Hall.
Bauer, Raymond A. 1961. “Risk Handling in Drug Adoption: The Role of Company
Preference.” Public Opinion Quarterly 25:546–59.
Bemmaor, Albert C. 1994. “Modeling the Diffusion of New Durable Goods: Word-of-
Mouth Effect versus Consumer Heterogeneity.” Pp. 201–23 in Research Traditionsin Marketing, edited by G. Laurent, G. L. Lilien, and B. Pras. Boston: KluwerAcademic Publishers.
Ben Gaffin and Associates. (1953) 1961a. “Report on a Study of Advertising and the
American Physician. Part I. The Advertisers’ Viewpoint.” Pp. 490–520 in DrugIndustry Antitrust Act, Hearings before the Senate Subcommittee on Antitrust andMonopoly of the Committee on the Judiciary. Washington, D.C.: GovernmentPrinting Office.
———. (1956) 1961b. “The Fond du Lac Study. A Basic Marketing Study Made for
the American Medical Association.” Pp. 697–806 in Drug Industry Antitrust Act,Hearings before the Senate Subcommittee on Antitrust and Monopoly of theCommittee on the Judiciary. Washington, D.C.: Government Printing Office.
———. 1959. Attitudes of U.S. Physicians toward the American PharmaceuticalIndustry. Chicago: American Medical Association.
Berndt, Ernst R., Linda T. Bui, David H. Lucking-Reiley, and Glen L. Urban. 1997.
“The Roles of Marketing, Product Quality, and Price Competition in the Growthand Composition of the U.S. Antiulcer Drug Industry,” Pp. 277–328 in TheEconomics of New Goods, edited by Timothy F. Bresnahan and Robert J. Gordon. Chicago: University of Chicago Press.
Besag, J. E. 1975. “The Statistical Analysis of Non-Lattice Data.” Statistician 24:
Bond, Ronald S., and David F. Lean. 1977. “Sales, Promotion, and Product
Differentiation in two Prescription Drug Markets.” Economic Report, Federal TradeCommission.
Bonus, Holger. 1973. “Quasi-Engel Curves, Diffusion, and the Ownership of Major
Consumer Durables.” Journal of Political Economy 81:655–77.
Brown, Lawrence A. 1981. Innovation Diffusion: A New Perspective. New York:
Burt, Ronald S. 1986. “The Medical Innovation Network Data.” Technical Report no.
3. Columbia University, Center for the Social Sciences.
———. 1987. “Social Contagion and Innovation: Cohesion versus Structural
Equivalence.” American Journal of Sociology 92:1287–1335.
———. 1997. “Neo-Classical Contagion: Recent Developments in the Network
Structure of Diffusion.” Unpublished note, University of Chicago.
Burt, Ronald S., and Gregory A. Janicik. 1996. “Social Contagion and Social Structure.”
Pp. 32–49 in Networks in Marketing, edited by Dawn Iacobucci. Thousand Oaks,Calif.: Sage.
Caplow, Theodore, and John J. Raymond. 1954. “Factors Influencing the Selection of
Pharmaceutical Products.” Journal of Marketing 19 (July): 18–23.
Chatterjee, Rabikar, and Jehoshua Eliashberg. 1990. “The Innovation Diffusion
Process in a Heterogeneous Population: A Micromodeling Approach.” ManagementScience 36:1057–79.
Cliff, A. D., P. Haggett, J. K. Ord, and G. R. Versey. 1981. Spatial Diffusion: AnHistorical Geography of Epidemics in an Island Community. Cambridge: CambridgeUniversity Press.
Coleman, James S. 1990. Foundations of Social Theory. Cambridge, Mass.: Harvard
Coleman, James S., Elihu Katz, and Herbert Menzel. 1966. Medical Innovation: ADiffusion Study. Indianapolis: Bobbs-Merrill.
Collier, David, and Richard E. Messick. 1975. “Prerequisites versus Diffusion: Testing
Alternative Explanations of Social Security Adoption.” American Political ScienceReview 69:1299–1315.
Commenges, Daniel, Luc Letenneur, He´le`ne Jacqmin, Thierry Moreau, and Jean-
Franc¸ois Dartigues. 1994. “Test of Homogeneity of Binary Data with ExplanatoryVariables.” Biometrics 50:613–20.
Davis, Fred D., Richard P. Bagozzi, and Paul R. Warshaw. 1989. “User Acceptance
of Computer Technology: A Comparison of Two Theoretical Models.” ManagementScience 35:982–1003.
Delacroix, Jacques, and Hayagreeva Rao. 1994. “Externalities and Ecological Theory:
Unbundling Density Dependence.” Pp. 255–68 in Evolutionary Dynamics ofOrganizations, edited by Joel A. C. Baum and Jitendra V. Singh. New York: OxfordUniversity Press.
DiMaggio, Paul J., and Walter W. Powell. 1983. “The Iron Cage Revisited: Institutional
Isomorphism and Collective Rationality in Organizational Fields.” AmericanSociological Review 48:147–60.
England, Paula. 1998. Concluding remarks to the Conference on Economic and
Organizational Sociology, University of Pennsylvania, December.
Erbring, Lutz, and Alice A. Young. 1979. “Individuals and Social Structure: Contextual
Effects as Endogenous Feedback.” Sociological Methods and Research 7:396–430.
Erikson, Robert. 1998. “Thresholds and Mechanisms: A Comment on Hedstro¨m and
Swedberg’s Chapter.” Pp. 88–93 in Rational Choice Theory and Large-Scale DataAnalysis, edited by Hans-Peter Blossfeld and Gerald Prein. Boulder, Colo.: WestviewPress.
Ferber, Robert, and Hugh G. Wales. 1958. The Effectiveness of PharmaceuticalPromotion. Urbana: University of Illinois, Bureau of Economic and BusinessResearch. Fortune. 1953. “Shock Therapy for Parke, Davis.” 48 (September): 108–13, 208–14. FTC (Federal Trade Commission). 1958. Economic Report on Antibiotics Manufacture.
Washington, D.C.: Government Printing Office.
Gatignon, Hubert, Barton Weitz, and Pradeep Bansal. 1990. “Brand Introduction
Strategies and Competitive Environments.” Journal of Marketing Research 27:390–401.
Glock, Charles Y. 1979. “Organizational Innovation for Social Research and Training.”
Pp. 23–36 in Qualitative and Quantitative Social Research: Papers in Honor of PaulF. Lazarsfeld, edited by Robert K. Merton, James S. Coleman, and Peter H. Rossi. New York: Free Press.
Granovetter, Mark S. 1978. “Threshold Models of Collective Action.” American Journal
Hahn, Minhi, Sehoon Park, Lakshman Krishnamurthi, and Andris A. Zoltners. 1994.
“Analysis of New Product Diffusion Using a Four-Segment Trial-Repeat Model.”Marketing Science 13:224–47.
Hamerle, Alfred. 1990. “Simple Test for Neglected Heterogeneity in Panel Studies.”
Han, Aaron, and Jerry A. Hausman. 1990. “Flexible Parametric Estimation of Duration
and Competing Risk Models.” Journal of Applied Econometrics 5:1–28.
Hannan, Timothy H., and John M. McDowell. 1987. “Rival Precedence and the
Dynamics of Technology Adoption: An Empirical Analysis.” Economica 54:155–71.
Harris, Jerome J. 1966. “Survey of Medical Communication Sources Available for
Continuing Physician Education.” Journal of Medical Education 41:737–55.
Haunschild, Pamela R., and Anne S. Miner. 1997. “Modes of Interorganizational
Imitation: The Effects of Outcome Salience and Uncertainty.” AdministrativeScience Quarterly 42:472–500.
Hawkins, Norman G. 1959. “The Detailman and Preference Behavior.” SouthwesternSocial Science Quarterly 40 (December): 213–24.
Hedstro¨m, Peter. 1994. “Contagious Collectivities: On the Spatial Diffusion of Swedish
Trade Unions, 1890–1940.” American Journal of Sociology 99:1157–79.
Hurwitz, Mark A., and Richard E. Caves. 1988. “Persuasion or Information? Promotion
and the Shares of Brand Name and Generic Pharmaceuticals.” Journal of Law andEconomics 31:299–320.
Kalish, Shlomo, and Gary L. Lilien. 1986. “Applications of Innovation Diffusion
Models in Marketing.” Pp. 235–79 in Innovation Diffusion Models of New ProductAcceptance, edited by Vijay Mahajan and Yoram Wind. Cambridge, Mass.:Ballinger.
Katz, Elihu. 1961. “The Social Itinerary of Technical Change: Two Studies on the
Diffusion of Innovation.” Human Organization 20 (Summer): 70–82.
Katz, Elihu, and Paul F. Lazarsfeld. 1955. Personal Influence. Glencoe, Ill.: Free Press. Katz, Michael L., and Carl Shapiro. 1994. “Systems Competition and Network Effects.”
Journal of Economic Perspectives 8:93–115.
Lilien, Gary L., Ambar Rao, and Shlomo Kalish. 1981. “Bayesian Estimation and
Control of Detailing Effort in a Repeat Purchase Diffusion Environment.”Management Science 27:493–506.
Marsden, Peter V., and Noah E. Friedkin. 1994. “Network Studies of Social Influence.”
Pp. 3–25 in Advances in Social Network Analysis: Research in the Social andBehavioral Sciences, edited by Stanley Wasserman and Joseph Galaskiewicz. Thousand Oaks, Calif.: Sage.
Marsden, Peter V., and Joel Podolny. 1990. “Dynamic Analysis of Network Diffusion
Processes.” Pp. 197–214 in Social Networks through Time, edited by Jeroen Weesieand Henk Flap. Utrecht: ISOR/Rijksuniversiteit Utrecht.
Menzel, Herbert, and Elihu Katz. 1955. “Social Relations and Innovation in the Medical
Profession: The Epidemiology of a New Drug.” Public Opinion Quarterly 19:337–52.
Mines, Samuel. 1978. Pfizer . . . An Informal History. New York: Pfizer. Montgomery, David B., and Alvin J. Silk. 1972. “Estimating Dynamic Effects of Market
Communications Expenditures.” Management Science, ser. B, 18:485–501.
Montgomery, Mark R., and John B. Casterline. 1996. “Social Learning, Social Influence,
and New Models of Fertility.” Population and Development Review 22 (suppl.):151–75.
Pearson, Michael. 1969. The Million-Dollar Bugs. New York: G.P. Putnam’s Sons. Peterson, Osler L., Leon P. Andrews, Robert S. Spain, and Bernard G. Greenburg.
1956. “An Analytical Study of North Carolina General Practice: 1953–54.” Journalof Medical Education 31 (December): 1–165.
Rangaswamy, Arvind, and Lakshman Krishnamurthi. 1991. “Response Function
Estimation Using the Equity Estimator.” Journal of Marketing Research 28:72–83.
Rizzo, John A. 1999. “Advertising and Competition in the Ethical Pharmaceutical
Industry: The Case of Antihypertensive Drugs.” Journal of Law and Economics 42:89–116.
Roberts, John H., and Glen L. Urban. 1988. “Modeling Multiattribute Utility, Risk,
and Belief Dynamics for New Consumer Durable Brand Choice.” ManagementScience 34:167–85.
Rogers, Everett M. 1994. A History of Communication Study: A BiographicalApproach. New York: Free Press.
———. 1995. Diffusion of Innovations, 4th ed. New York: Free Press. Shankar, Venkatesh, Gregory S. Carpenter, and Lakshman Krishnamurthi. 1998. “Late
Mover Advantage: How Innovative Late Entrants Outsell Pioneers.” Journal ofMarketing Research 35:54–70.
Strang, David. 1991. “Adding Social Structure to Diffusion Models: An Event History
Framework.” Sociological Methods and Research 19:324–53.
Strang, David, and Nancy Brandon Tuma. 1993. “Spatial and Temporal Heterogeneity
in Diffusion.” American Journal of Sociology 99:614–39.
Taibleson, Mitchell H. 1974. “Distinguishing between Contagion, Heterogeneity, and
Randomness in Stochastic Models.” American Sociological Review 39:877–80.
Thirtle, Colin G., and Vernon W. Ruttan. 1987. The Role of Demand and Supply inthe Generation and Diffusion of Technical Change. Chur: Harwood Academic.
Valente, Thomas W. 1996. “Social Network Thresholds in the Diffusion of
Innovations.” Social Networks 18:69–89.
Van den Bulte, Christophe, and Gary L. Lilien. 1999. “Integrating Models of Innovation
Adoption: Social Contagion, Utility Maximization, and Hazard Models.” WorkingPaper 99-021. University of Pennsylvania, Wharton School, Marketing Department.
van Waterschoot, Walter, and Christophe Van den Bulte. 1992. “The 4P-Classification
of the Marketing Mix Revisited.” Journal of Marketing 56 (October): 83–93.
Weber, Max. (1921) 1968. Economy and Society. Translated by G. Roth and C. Wittich.
Winick, Charles. 1961. “The Diffusion of an Innovation among Physicians in a Large
City.” Sociometry 24:384–396.
How to grow Marijuana courtesy of the Jolly Roger MARIJUANA Marijuana is a deciduous plant which grows from seeds. The fibrous section of the plant was (has been replaced by synthetics) used to make rope. The flowering tops, leaves, seeds, and resin of the plant is used by just about everyone to get HIGH. Normally, the vegetable parts of the plant are smoked to produce this "high," bu
Templeogue Utd FC Fixtures for 6th and 7th April 2013 Club Team League Division Sean Murphy Dodder Valley Seamus McGrath Esker Celtic D Culliton John Hewitt D Culliton Pat Cooney D Culliton Stephen Collier Firhouse Carmel Firhouse CC Trevor McDonagh Malahide Utd D Culliton Brian Donohoe Bushy Park Rob Flanagan St Kevins Boys 12B
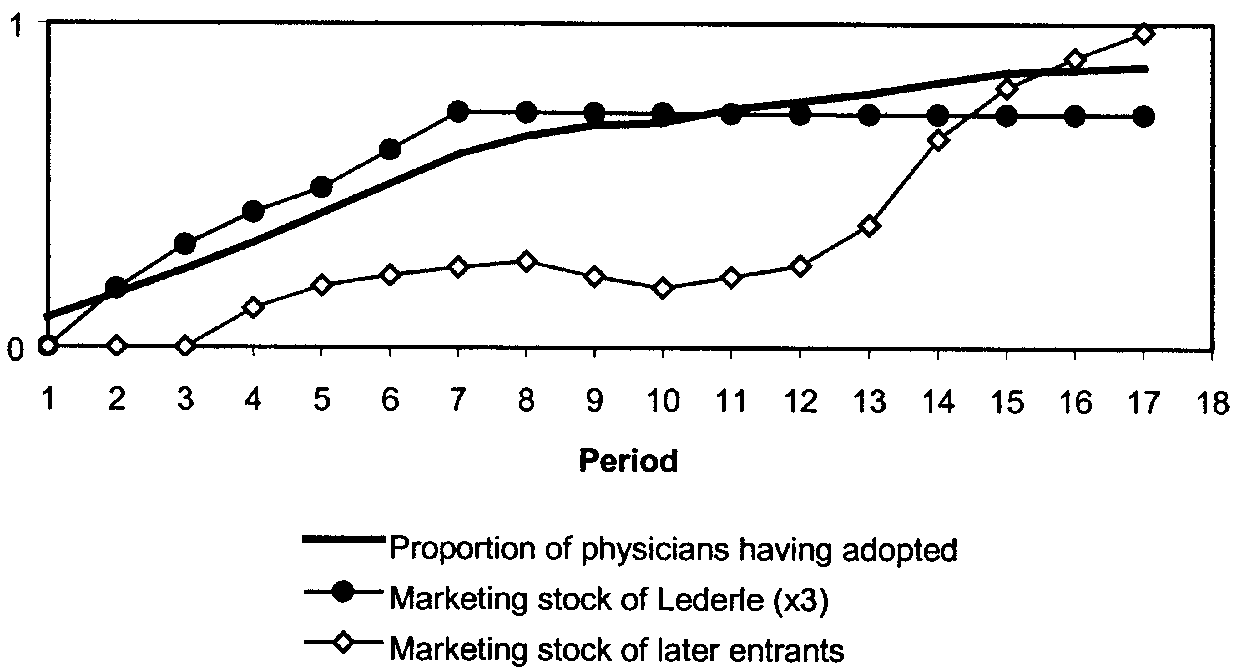 Fig. 1.—Adoptions and marketing stock; marketing stock is defined as the depreciation-
adjusted cumulative advertising volume (see eq. [2]).
Fig. 1.—Adoptions and marketing stock; marketing stock is defined as the depreciation-
adjusted cumulative advertising volume (see eq. [2]).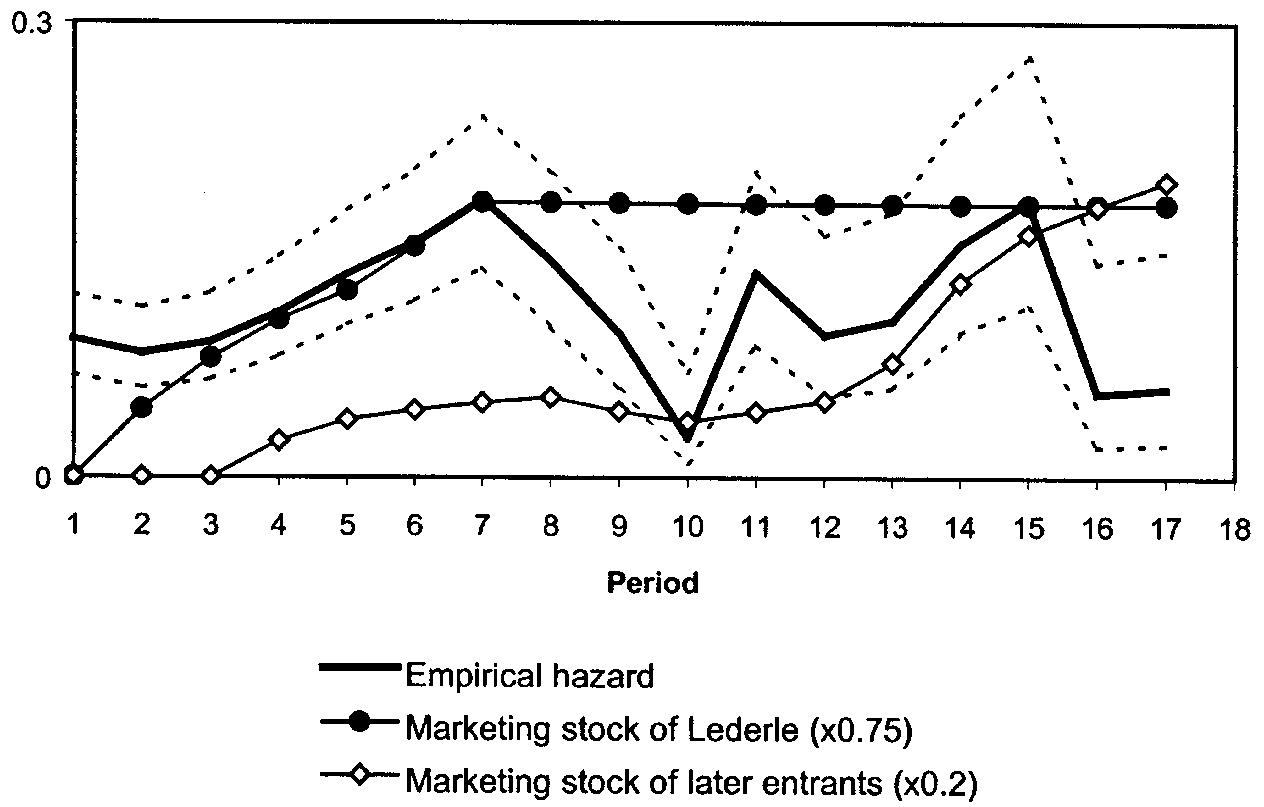 Fig. 2.—Empirical hazard rate and marketing stock. The broken lines around the em-
pirical hazard rate indicate the SE interval (ϩ/ Ϫ 1). We computed SEs using a logit hazardmodel. The interval is not symmetric because the logit model is linear in the log odds ofthe hazard rate, not in the hazard rate itself.
Fig. 2.—Empirical hazard rate and marketing stock. The broken lines around the em-
pirical hazard rate indicate the SE interval (ϩ/ Ϫ 1). We computed SEs using a logit hazardmodel. The interval is not symmetric because the logit model is linear in the log odds ofthe hazard rate, not in the hazard rate itself.