rich3/jgp-ajgp/jgp-ajgp/jgp99908/jgp0562-09z S؍1 7/18/09 7:24 Art: JGP200550 Input-us Change in Cognitive Functioning After Acute Antidepressant Treatment in Late-Life Depression Michelle Culang, B.S., Joel R. Sneed, Ph.D., John G. Keilp, Ph.D., Bret R. Rutherford, M.D., Gregory H. Pelton, M.D., D. P. Devanand, M.D., Steven P. Roose, M.D. Objective: Selective Serotonin Reuptake Inhibitors (SSRIs) are the most commonly prescribed medications for geriatric depression. The association of late-life depression and cognitive impairment has been well documented. However, there have been fewplacebo-controlled trials examining the impact of SSRIs on cognitive functioning. De- sign: Prepost neuropsychological (NP) data collected as part of an 8-week, double-blind, placebo-controlled trial of citalopram in depressed patients aged 75 years and older were used to examine change in cognitive functioning. Setting: University-affiliated outpa- tient psychiatry clinics. Participants: One hundred seventy-four community-dwelling men and women aged 75 years or older with nonpsychotic unipolar depression. Mea- surements: NP assessments included mental status (Mini-Mental State Examination), psychomotor speed (Wechsler Adult Intelligence Scale-III Digit Symbol Subtest), reaction time (Choice Reaction Time), visual-spatial skill (Judgment of Line Orientation), execu-tive functioning (Stroop Color/Word Test), and memory (Buschke Selective RemindingTest). Results: Differences in the pattern of change by treatment group depended on responder status. Citalopram nonresponders were the only group to decline on verbal learning and psychomotor speed. Citalopram responders showed significant improve-ment in visuospatial functioning, when compared with nonresponders in either condi-tion, but their improvement was not greater than responders on placebo. Citalopramresponders showed greater improvement on psychomotor speed than citalopram nonre-sponders, but their improvement was not greater than placebo responders or nonre-sponders. Conclusions: Medication may have a deleterious effect on some aspects of cognition among patients aged 75 years and older who have not responded. This suggests that patients should not be maintained on a medication if they have not had anadequate response. (Am J Geriatr Psychiatry 2009; ●:000 –000)
Key Words: Cognitive functioning, cognitive impairment, geriatric depression, late-life depression, citalopram
Received November 3, 2008; revised May 4, 2009; accepted June 1, 2009. From the Queens College, City University of New York (MC, JRS); and
Columbia University and the New York State Psychiatric Institute (MC, JRS, JGK, BRR, GHP, DPD, SPR), NY. Send correspondence and reprintrequests to Michelle Culang, B.S., Department of Psychology, Queens College of the City University of New York, 65-30 Kissena Blvd, Flushing,NY 11367. e-mail: michelle.culang@qc.cuny.edu
2009 American Association for Geriatric Psychiatry
Am J Geriatr Psychiatry ●:●, ●●● 2009
rich3/jgp-ajgp/jgp-ajgp/jgp99908/jgp0562-09z S؍1 7/18/09 7:24 Art: JGP200550 Input-us
SelectiveSerotoninReuptakeInhibitors(SSRIs)are been few placebo-controlled trials examining this is-
the first-line of treatment in the geriatric de-
sue. In one study, nortriptyline and phenelzine pro-
pressed due to the efficacy, safety, and tolerability of
duced no change in cognition in depressed older
its class. Cognitive impairment is common in late-life
adults, when compared with placebo, and this effect
depression (LLD), particularly in memory,1–3 vi-
did not depend on responder status.8 However, the
suospatial functioning,2,4 information processing
small sample size and limited number of responders
speed,5,6 and executive functioning.5,7 It is important
made it difficult to determine the impact of responder
to consider the impact that antidepressant treatment
status on change in cognition. Furthermore, this study
can have on cognition when treating depressed older
was restricted to the use of a TCA and MAO-I. In
another study, patients taking duloxetine showed sig-
Research that has examined the impact of SSRIs on
nificant improvement in verbal learning and memory,
the cognitive functioning of depressed older adults
when compared with the placebo group.15 Therefore, it
has been inconclusive because most studies have
is unclear what impact medication, SSRIs in particular,
been limited by methodological constraints includ-
ing small sample size or lack of an age-matched
The purpose of this study was to examine the
control group for comparison.8–11 For instance, treat-
impact of antidepressant treatment on change in cog-
ment of LLD with sertraline led to an improvement
nitive functioning. To accomplish this aim, we used
in short- and long-term memory storage and re-
neuropsychological (NP) data collected as part of the
trieval and speed of processing.11 Although these
Old-Old Depression Study,16 a large (N ϭ 174), ran-
results suggest that some aspects of cognition (i.e.,
domized, double-blind, placebo-controlled trial of
memory and processing speed) improve with anti-
citalopram in depressed older adults (age Ͼ75
depressant treatment, it is difficult to determine
years). These data provided us with the methodolog-
whether the improvement was a function of repeat
ical strength to address two questions: 1) do patients
testing or medication because the design lacked a
treated with citalopram show differential change in
cognitive functioning over the 8 weeks, when com-
Studies using age-matched controls have shown
pared with patients treated with placebo? 2) Does
that cognitive functioning of depressed older adults
change in cognitive performance depend on re-
does not improve beyond the expected practice effect
sponder status? To our knowledge, this is the first
(practice effects refer to improvement due to repeat
attempt to approach these issues using a placebo-
testing and are defined by the performance of a
controlled trial of an SSRI in an old-old (Ͼ75 years)
comparison condition, either an age-matched control
group12–14 or a placebo comparison group,8,15 that is
not being treated with medication).12–14 For example,working and episodic memory, attention shifting,and processing speed did not improve after treat-
ment with paroxetine to a greater degree than nor-mal controls did with practice, regardless of re-
The procedures used in the multisite, randomized,
sponder status.14 Similarly, cognitive functioning
placebo-controlled trial (RCT) have been previously
showed no improvement beyond a practice effect
described.16–18 Briefly, 174 community-dwelling men
among responders to either nortriptyline or parox-
and women aged 75 years or older meeting Diagnos-
etine.13 These studies suggest that depressed older
tic and Statistical Manual of Mental Disorders,
adults show little improvement as a function of treat-
Fourth Edition criteria (based on Structured Clinical
ment and cognitive impairment persists after an ad-
Interview for Diagnostic and Statistical Manual of
equate trial of antidepressant medication.
Mental Disorders-III-R interview) for nonpsychotic
Although such designs allow us to determine
unipolar depression (single or recurrent) with a base-
whether cognition changes as a function of antide-
line 24-item Hamilton Rating Scale for Depression
pressant treatment, it does not allow us to conclude
(HRSD) score Ն20 participated in this 8-week RCT.
that the change (if any) is a result of treatment due to
All patients began the trial with a 1-week single-
a lack of a placebo condition. However, there have
blind placebo lead-in with the baseline visit con-
Am J Geriatr Psychiatry ●:●, ●●● 2009
rich3/jgp-ajgp/jgp-ajgp/jgp99908/jgp0562-09z S؍1 7/18/09 7:24 Art: JGP200550 Input-us
ducted at the end of the lead-in. Patients were ran-
reflect uncertainty due to missing values and im-
domized to citalopram 20 mg/day or matched
placebo only if they continued to meet inclusion andexclusion criteria at the end of the placebo lead-in. At
Statistical Analyses
the end of Week 4, patients with a HRSD score Ͼ10had the dose increased to two pills per day, i.e., 40
Before testing for differences in change in NP test
mg of citalopram or 2 placebo pills.
performance, we used the PROC REG and PROCLOGISTIC procedures in SAS to test for differences
NP Test Battery
at baseline between the two treatment conditionsand the four treatment condition by responder status
The test battery was designed to assess a number
groups (see later). There were no differences on age,
of cognitive functions pertinent to aging and major
education, gender, baseline depression severity, re-
depression including mental status, psychomotor
sponder status, or on any of the NP tests with the
speed, reaction time, visual-spatial skill, attention,
exception of baseline scores on the MMSE and Digit
and memory. Three of the tests (Choice Reaction
Symbol subtest of the Wechsler Adult Intelligence
Time [CRT], Judgment of Line Orientation [JOLO],
Scale-III. Therefore, we adjusted for baseline Digit
and Stroop) were presented on a Macintosh laptop
Symbol and MMSE scores in the two treatment
computer and were written in the PsyScope pro-
group analyses. When comparing the four patient
gramming language,19 whereas the other three tests
groups (responder status by treatment condition),
(Mini-Mental State Exam, Buschke Selective Remind-
we found differences on education and baseline
ing Test [SRT], and Digit Symbol) were administered
MMSE, CRT, and Buschke SRT scores. Therefore, we
by hand. The tests included the 30-item Folstein
included these variables as covariates in the four
Mini-Mental State Examination (MMSE)20 to esti-
group analyses. We also adjusted for site of study in
mate global cognitive functioning, the Wechsler
all analyses, which we know from previous reports
Adult Intelligence Scale-III Digit Symbol Subtest21 as
a measure of psychomotor speed, the CRT test
To test for differences in change in NP test perfor-
adapted from Thorne et al.,22 the Stroop Color/Word
mance, we used data from the multiply imputed
Test23 to assess the response inhibition component of
datasets and adopted a partial or regressed change
executive functioning, the JOLO24 as a measure of
approach to analyzing two time-point data29 using
spatial judgment, and the Buschke SRT25 as a mea-
the PROC REG procedure in SAS. According to this
approach, the endpoint NP test score is treated as theoutcome variable, and the baseline test score istreated as a covariate. This effectively removes all
Missing Data
correlation of the endpoint score from the baseline
Missing data at baseline ranged from 0.6% on the
score and represents an improvement over simple
MMSE and Buschke SRT to 9.8% on the JOLO and
change scores (subtracting baseline from endpoint),
from 11.5% on the MMSE to 19.0% on the Stroop at
which tend to overcorrect the endpoint score by the
follow-up. To accommodate missing data, we used
baseline score due to unreliability of measurement.29
multiple imputation using the PROC MI and
We first tested for differences in endpoint scores
MIANALYZE procedures in SAS. Multiple imputa-
between treatment conditions using a dummy coded
tion is a simulation technique that replaces each
(citalopram ϭ 1 and placebo ϭ 0) variable. To test
missing datum with a set of m Ͼ1 plausible values.26
whether change in NP test performance depends on
This report is based on five imputed datasets (m ϭ 5),
responder status (50% reduction from baseline
which is sufficient to obtain excellent results unless
HRSD score), we again used a dummy coded vari-
rates of missing data are exceptionally high.27 The
able to designate the four patient groups (citalopram
imputed datasets are analyzed using standard statis-
responders, citalopram nonresponders, placebo re-
tical analyses, and results from the analyses from the
sponders, and placebo nonresponders). Each covari-
m complete datasets are combined using Rubin’s
ate was centered at its respective mean, so the inter-
rules26,28 to generate valid statistical inferences that
cept corresponded to the mean of the reference
Am J Geriatr Psychiatry ●:●, ●●● 2009
rich3/jgp-ajgp/jgp-ajgp/jgp99908/jgp0562-09z S؍1 7/18/09 7:24 Art: JGP200550 Input-us
group at endpoint and the unstandardized regres-
Hypothesis Testing
sion weights reflected the difference between thegroups included in the model and the reference
Table 2 shows the unadjusted means and standard
group (excluded from the model). All significance
deviations for all NP tests both pre and posttreat-
tests were evaluated at the 5% level.
ment for the citalopram and placebo groups and thefour patient groups (treatment group by responderstatus). Adjusting for site and baseline MMSE and
Digit Symbol, there was a statistically significant dif-ference between the placebo and citalopram condi-
Descriptive Statistics
tions at endpoint on the Buschke SRT. Specifically,patients treated with citalopram scored lower at end-
Table 1 presents baseline demographic and clinical
point than patients treated with placebo (B ϭ Ϫ2.74,
characteristics of the total sample, placebo and cita-
SE ϭ 1.41, t[1,087] ϭ Ϫ1.94, 95% CI: Ϫ5.52 to 0.03,
lopram groups, and the four groups of patients clas-
sified by treatment condition and responder status.
We next compared the four groups of patients
The average study participant was 79.57 years and
classified according to treatment condition and re-
completed about 2 years of college. Approximately
sponder status on endpoint NP test performance. As
58% of the sample were women, average baseline
can be seen in Table 2, citalopram responders scored
depression severity was 24.32 on the 24-item HRSD,
significantly higher than both citalopram nonre-
and 40% of the sample was classified as responders.
sponders (B ϭ Ϫ2.54, SE ϭ 0.97, t[80.46] ϭ Ϫ2.54,
The average MMSE score of the sample at baseline
95% CI: Ϫ4.38 to Ϫ0.53, p ϭ 0.01) and placebo non-
was 27.99, and 6.9% had a score of 24 or below.
responders (B ϭ Ϫ2.47, SE ϭ 0.89, t(217.31) ϭ Ϫ2.77,
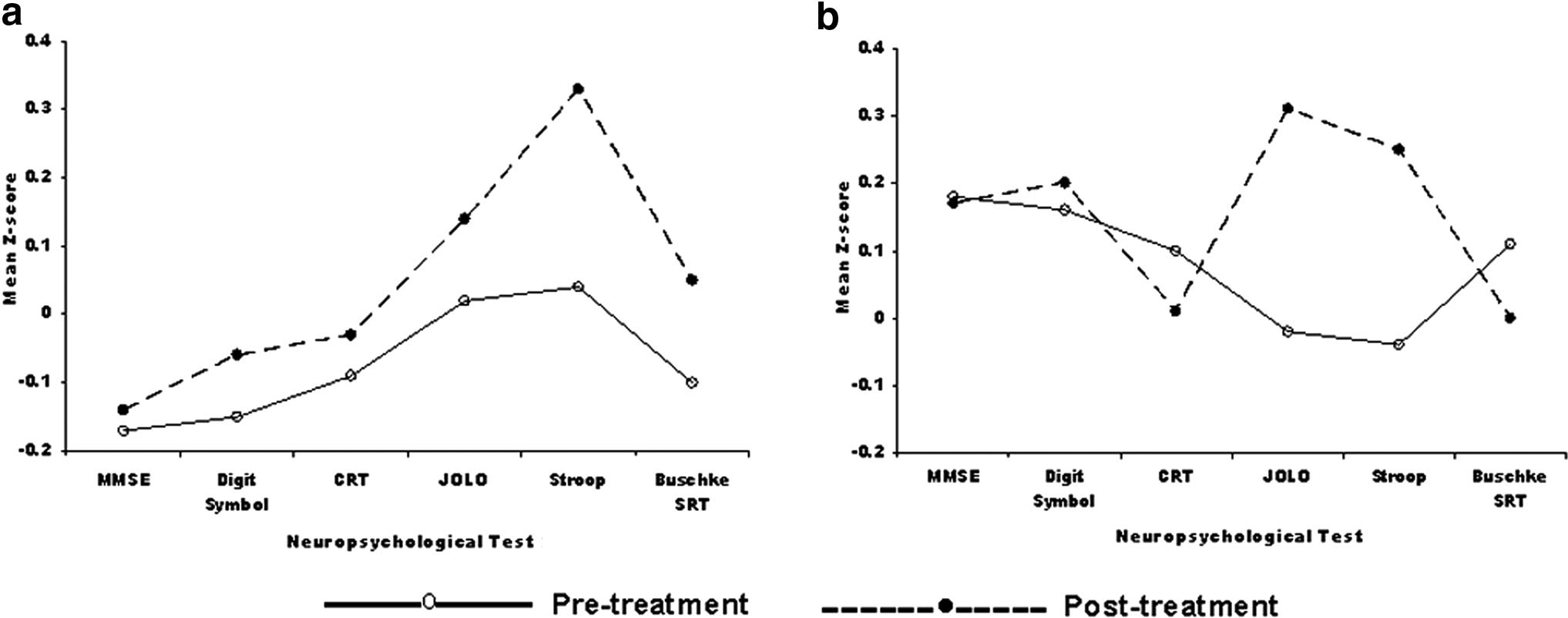
To facilitate interpretation of the pattern of change
95% CI: Ϫ4.23 to Ϫ0.71, p ϭ 0.01) on the JOLO at
in NP test performance as a function of treatment
endpoint. However, citalopram responders were not
group, all NP scores were converted to z-scoresbased on mean values at baseline in the total sample.
statistically significantly different than placebo re-
As can be seen in Fig. 1, NP test performance im-
sponders at endpoint (B ϭ Ϫ1.81, SE ϭ 1.02, t[111.56] ϭ
proved on each test in the placebo group, which is
Ϫ1.78, 95% CI: Ϫ3.83 to 0.20, p ϭ 0.08). Looking at
consistent with a practice effect. For the purposes of
endpoint performance on the Buschke SRT, citalo-
this report, practice effects refer to improvement in
pram nonresponders were the only group to decline
performance due to repeat testing and are defined on
from pretest to posttest. Specifically, citalopram non-
the basis of the performance of the placebo group.
responders scored lower (3.64 points) than placebo
Differences from the placebo group (both positive and
nonresponders at study end (B ϭ Ϫ3.64, SE ϭ 1.83,
negative) reflect deviations from a practice effect and
t(472.15) ϭ Ϫ1.99, 95% CI: Ϫ7.23 to Ϫ0.05, p ϭ 0.05).
represent either improvement beyond a practice effect
Similarly, citalopram nonresponders were the only
or the absence of a practice effect, possibly even de-
group to decline from pretest to posttest on the Digit
cline. As can be seen in Fig. 1, the citalopram group
Symbol. In particular, citalopram nonresponders
improved on some tests and declined on others.
scored lower than citalopram responders at endpoint
Baseline Clinical and Demographic Characteristics of the Total Sample, the Citalopram and Placebo Conditions, and the Four Patients Groups Classified by Treatment Condition and Responder Status Total Sample Citalopram Citalopram Citalopram Variable (n ؍ 174) Responders Nonresponders Responders Nonresponders
Am J Geriatr Psychiatry ●:●, ●●● 2009
rich3/jgp-ajgp/jgp-ajgp/jgp99908/jgp0562-09z S؍1 7/18/09 7:24 Art: JGP200550 Input-us FIGURE 1. Change in Cognitive Performance From Pre to Posttreatment in the (a) Placebo Condition and (b) Citalopram Condition Across Six Neuropsychological Tests
(B ϭ Ϫ5.62, SE ϭ 2.65, t(233.31) ϭ Ϫ2.12, 95% CI:
nonresponders on medication. Therefore, these find-
ings suggest that patients should not be maintainedon a medication if they have not had an adequateresponse.
One possible explanation for the observed decline
DISCUSSION
in verbal learning and psychomotor speed is that the
This was the first study to examine the impact of
overall level of cognitive functioning in the sample
antidepressant treatment on change in cognitive
was low and the citalopram group had a dispropor-
functioning in depressed adults aged 75 years and
tionately high number of cognitively impaired pa-
older using data from an 8-week RCT. Although the
tients. This might explain why there was inconsistent
placebo group showed a distinct practice effect from
improvement in the citalopram condition and why
baseline to endpoint on all NP tests, the citalopram
this study differs from previous placebo-controlled
group improved on some tests but declined on oth-
trials.8,15 However, the average MMSE score at base-
ers. However, the pattern of change depended on
line for the sample was 28, which is well within
responder status. Specifically, citalopram nonre-
normal limits. Moreover, although there was a sig-
sponders were the only group to decline in perfor-
nificant difference in MMSE scores between the treat-
mance on verbal learning (Buschke SRT) and psy-
ment groups at baseline, it was the citalopram group
that scored higher at baseline than the placebo
responders showed significant improvement in
visuospatial functioning (JOLO), when compared
Another possibility is that brain lesions, which are
with nonresponders in either condition, but their
associated with age30 and other risk factors such as
improvement was not greater than responders on
hypertension and diabetes,31 were disproportion-
placebo. Similarly, citalopram responders showed
ately represented in the citalopram condition. White
greater improvement on psychomotor speed (Digit
matter hyperintensities (WMH) that are characteris-
Symbol) than citalopram nonresponders, but their
tic of LLD may interrupt frontal-striatal pathways
improvement was not greater than placebo respond-
that mediate cognitive functions that are commonly
ers or nonresponders. The findings indicate that the
impaired in LLD. Furthermore, cognitive impair-
practice effect is impaired in some domains among
ment is associated with the presence of WMH in LLD
Am J Geriatr Psychiatry ●:●, ●●● 2009
rich3/jgp-ajgp/jgp-ajgp/jgp99908/jgp0562-09z S؍1 7/18/09 7:24 Art: JGP200550 Input-us
and deficits worsen as the lesions become more se-
vere.2,5 However, there were no statistically signifi-
cant differences in the percentage of patients in the
citalopram group and the placebo group classified as
having high lesion load, which was defined as a deep
Nonresponders
WMH rating of 2 or a subcortical gray matter rating
of 3 on the Fazekas modified Coffey Rating Scale for
The decline in verbal learning may be particularly
attributed to the anticholinergic effects of SSRIs. SSRIs
have unique nonserotonergic pharmacologic profiles
Subsamples
that are associated with distinct effects on cognitive
Responders
functioning.33 Paroxetine, for example, may cause
impairment in delayed verbal recall in healthy mid-
dle-aged adults and elderly subjects, whereas sertra-
line is associated with improvement in immediateand
ncy.34,35 Although administration of citalopram is
Citalopram
associated with improvement in working memory in
depressed adults36 and increased memory consolida-
Citalopram Nonresponders
tion in healthy adults,37 it is still unclear what effect
citalopram can have on cognitive functioning of the
geriatric depressed, a population that is especially
Endpoint
vulnerable to the adverse effects of antidepressant
The observed decline in verbal learning and psy-
chomotor speed in the citalopram group is consistent
Baseline Citalopram Responders
with a recent report from an epidemiological study
Responder
of elderly depressed patients examining the relation-
ship among depressive symptoms, cognitive impair-
ment, and antidepressant use.39 Findings revealed
that baseline depression scores predicted future mild
cognitive impairment (MCI) but only among those
Condition
using antidepressant medications at baseline. Taken
Performance
together, these findings support the contention that
nonresponders should not be maintained on medi-
Treatment
cation that may have a negative impact on some
aspects of cognitive functioning, which may facilitatethe development of MCI.40
This study should be interpreted in the context of
According
several limitations. First, there were statistically sig-
nificant differences between the two treatment con-
Neuropsychological
ditions and the four patient groups at baseline on
Classified Citalopram
several NP tests. However, these differences were
adjusted for in the statistical models by including
Unadjusted
those tests as covariates. Second, it may be possible
that including a small number of MCI patients
(MMSE Յ24) in this study (N ϭ 12) might have
influenced our results. However, we ran the analyses
Am J Geriatr Psychiatry ●:●, ●●● 2009
rich3/jgp-ajgp/jgp-ajgp/jgp99908/jgp0562-09z S؍1 7/18/09 7:24 Art: JGP200550 Input-us
with and without this group of patients, and the
respond on medication. Although responders on
results were not different. Third, there was missing
medication may improve in some domains, their
data, as is typically the case in clinical trials, and we
improvement does not exceed the expected practice
accommodated for missing data using multiple im-
effect observed in patients randomized to placebo.
putation, a far superior method compared with tra-
This raises the important clinical issue that, although
ditional approaches using mean substitution or com-
two treatments may be equivalent with regard to
plete case analysis. Fourth, a somewhat limited NP
response, they may have differential effects on cog-
battery was used. Only one aspect of executive func-
nitive functioning, especially in a cognitively vulner-
tioning (i.e., response inhibition) was evaluated, and
able population. Our findings suggest that nonre-
no formal test of attention was included in the study.
sponders should not be maintained on medication
However, these limitations are balanced by using
that may have a negative effect on some aspects of
data from the only randomized, placebo-controlled
clinical trial of antidepressant treatment among de-pressed patients aged 75 years or older. Moreover,
This work was supported by a grant from Forest
unlike other studies, there were an approximately
Laboratories and National Institute of Mental Health
equal number of responders in both treatment con-
grants T32 MH20004 (to SPR) and K23 MH075006 (to
ditions, allowing for an adequate test of whether
JRS) and from Eli Lilly and Novartis (to DPD).
change in cognitive function across two treatments
SPR has received consultant fees from Forest Labo-ratories, Wyeth Pharmaceuticals, Sanofi-Anventis, Pfizer,
Our findings indicate that citalopram may inter-
and Sierra Pharmaceuticals and DPD has received con-
fere with the normal practice effect in verbal learning
sultant fees from Glaxosmithkline, Acadia, and Sanofi-
and psychomotor speed among patients who do not
References
1. Salloway S, Malloy P, Kohn R, et al: MRI and neuropsychological
11. Doraiswamy PM, Krishnan KR, Oxman T, et al: Does antide-
differences in early- and late-life-onset geriatric depression. Neu-
pressant therapy improve cognition in elderly depressed pa-
tients? J Gerontol A Biol Sci Med Sci 2003; 58:M1137–M1144
2. Kramer-Ginsberg E, Greenwald BS, Krishnan KRR, et al: Neuro-
12. Portella MJ, Marcos T, Rami L, et al: Residual cognitive impair-
psychological functioning and mri signal hyperintensities in geri-
ment in late-life depression after a 12-month period follow-up. Int
atric depression. Am J Psychiatry 1999; 156:438 – 444
J Geriatric Psychiatry 2003; 18:571–576
3. Gallassi R, Di Sarro R, Morreale A, et al: Memory impairment in
13. Butters MA, Becker JT, Nebes RD, et al: Changes in cognitive
patients with late-onset major depression: the effect of antide-
functioning following treatment of late-life depression. Am J Psy-
pressant therapy. J Affect Disord 2006; 91:243–250
4. Butters MA, Whyte EM, Nebes RD, et al: The nature and determi-
14. Nebes RD, Pollock BG, Houck PR, et al: Persistence of cognitive
nants of neuropsychological functioning in late-life depression.
impairment in geriatric patients following antidepressant treat-
ment: a randomized, double-blind clinical trial with nortriptyline
5. Lesser I, Boone K, Mehringer C, et al: Cognition and white matter
and paroxetine. J Psychiatr Res 2003; 37:99 –108
hyperintensities in older depressed patients. Am J Psychiatry
15. Raskin J, Wiltse CG, Siegal A, et al: Efficacy of duloxetine on
cognition, depression, and pain in elderly patients with major
6. Nebes RD, Butters MA, Mulsant BH, et al: Decreased working
depressive disorder: an 8-week, double-blind, placebo-controlled
memory and processing speed mediate cognitive impairment in
trial. Am J Psychiatry 2007; 164:900 –909
geriatric depression Psychol Med 2000; 30:679 – 691
16. Roose SP, Sackeim HA, Krishnan KRR, et al: Antidepressant phar-
7. Lockwood KA, Alexopoulos GS, van Gorp WG: Executive dys-
macotherapy in the treatment of depression in the very old: a
function in geriatric depression.[see comment]. Am J Psychiatry
randomized, placebo-controlled trial. Am J Psychiatry 2004; 161:
8. Georgotas A, McCue RE, Reisberg B, et al: The effects of mood
17. Sneed JR, Roose SP, Keilp JG, et al: Response inhibition predicts
changes and antidepressants on the cognitive capacity of el-
poor antidepressant treatment response in very old depressed
derly depressed patients. Int Psychogeriatr 1989; 1:135–143
patients. Am J Geriatr Psychiatry 2007; 15:553–563
9. Nebes RD, Pollock BG, Mulsant BH, et al: Cognitive effects of
18. Sneed JR, Keilp JG, Brickman AM, et al: The specificity of neuro-
paroxetine in older depressed patients. J Clin Psychiatry 1999;
psychological impairment in predicting antidepressant non-re-
sponse in the very old depressed. Int J Geriatr Psychiatry 2008;
10. Bondareff W, Alpert M, Friedhoff AJ, et al: Comparison of sertra-
line and nortriptyline in the treatment of major depressive disor-
19. Cohen JD, MacWhinney B, Flatt M, et al: PsyScope: an interactive
der in late life. Am J Psychiatry 2000; 157:729 –736
graphic system for designing and controlling experiments in the
Am J Geriatr Psychiatry ●:●, ●●● 2009
rich3/jgp-ajgp/jgp-ajgp/jgp99908/jgp0562-09z S؍1 7/18/09 7:24 Art: JGP200550 Input-us
psychology laboratory using Macintosh computers. Behav Res
31. Murray AD, Staff RT, Shenkin SD, et al: Brain white matter hyper-
Methods Instruments Comput 1993; 25:257–271
intensities: relative importance of vascular risk factors in nonde-
20. Folstein MF, Folstein SE, McHugh PR: Mini-mental state: a practi-
mented elderly people. Radiology 2005; 237:251–257
cal method for grading the state of patients for the clinician.
32. Krishnan KR, Hays JC, Blazer DG: MRI-defined vascular depres-
sion. Am J Psychiatry 1997; 154:497–501
21. Wechsler D: Wechsler Adult Intelligence Scale 3rd Revision
33. Chew ML, Mulsant BH, Pollock BG, et al: Anticholinergic activity
(WAIS-III). San Antonio, Psychological Corporation, 1997
of 107 medications commonly used by older adults. J Am Geriatr
22. Thorne DR, Genser SG, Sing HC, et al: The Walter reed perfor-
mance assessment battery. Neurobehav Toxicol Teratol 1998;
34. Schmitt JAJ, Kruizinga MJ, Riedel WJ: Non-serotonergic pharma-
cological profiles and associated cognitive effects of serotonin
23. MacLeod C: A half-century of research on the Stroop effect: an
reuptake inhibitors. J Psychopharmacol 2001; 15:173–179
integrative review. Psychol Bull 1991; 109:163–203
35. Furlan PM, Kallan MJ, Ten Have T, et al: Cognitive and psychomo-
24. Benton AL, Sivan AB, Hamsher K, et al: Contributions to Neuro-
tor effects of paroxetine and sertraline on healthy elderly volun-
psychological Assessment. New York, Oxford, 1983
teers. Geriatr Psychiatry 2001; 9:429 – 438
25. Buschke H, Fuld P: Evaluating storage, retention, and retrieval in
36. Zobel AW, Schulze-Rauschenbach S, von Widdern OC, et al:
disordered memory and learning. Neurology 1974; 24:1019 –1025
Improvement of working but not declarative memory is corre-
26. Schafer JL, Olsen MK: Multiple imputation for multivariate miss-
lated with HPA normalization during antidepressant treatment.
ing-data problems: a data analyst’s perspective. Multivariate Be-
37. Harmer CJ, Bhagwagar Z, Cowen PJ, et al: Acute administration of
27. Schafer JL: Multiple imputation: a primer. Stat Methods Med Res
citalopram facilitates memory consolidation in healthy volun-
teers. Psychopharmacology 2002; 163:106 –110
28. Schafer JL, Graham JW: Missing data: our view of the state of the
38. Baldwin D, Johnson FN: Tolerability and safety of citalopram. Rev
29. Cohen J, Cohen P, West SG, et al: Applied Multiple Regression/
39. Ravaglia G, Forti P, Lucicesare A, et al: Prevalent depressive
Correlation for the Behavioral Sciences. 3rd ed. Mahwah, NJ,
symptoms as a risk factor for conversion to mild cognitive im-
Lawrence Erlbaum Associates Publishers, 2003
pairment in an elderly Italian cohort. Am J Geriatr Psychiatry
30. Taylor WD, MacFall JR, Steffens DC, et al: Localization of
age-associated white matter hyperintensities in late-life depres-
40. Devanand DP, Pelton GH, Marston K, et al: Sertraline treatment of
sion. Prog Neuropsychopharmacol Biol Psychiatry 2003; 27:
elderly patients with depression and cognitive impairment. Int J
Am J Geriatr Psychiatry ●:●, ●●● 2009
JOBNAME: AUTHOR QUERIES PAGE: 1 SESS: 1 OUTPUT: Sat Jul 18 07:24:17 2009
/rich3/jgpϪajgp/jgpϪajgp/jgp99908/jgp0562Ϫ09z
AUTHOR PLEASE ANSWER ALL QUERIES
1—Kindly check whether the minor edit made to the article title is appropriate.
2—Kindly spell out the first name of the author “D.P. Devanand.”
3—Please note that the page foot note has been moved to the text as per journal style.
4 —Kindly spell out TCA and MAO-I.
5—Kindly check whether tables are OK as typeset.
6 —Kindly check whether the grant information and the disclosure are OK as typeset.
7—Please note that Ref. 19 (original number) has been deleted as it seemed to be repetition of Ref.
16 and also the corresponding references have been renumbered as to make it sequential perjournal style.
8 —Kindly provide department/division name (if any) for the affiliations.
Question Response Some patients with heart or other problems, who cannot be treated with IVIg anymore, are treated with plasmapheresis. But after some plasmapheresis sessions If immunosuppressant drugs and steroids prove not sufficient, rituximab they developed allergy. What is the choice of therapy available?Allergy to these treatments are extremely rare in my experience (to say the truth
Dear Sir We read with interest the article ‘HotMoreover, the type of headache that they describebath-related headache controlled by topiramate’ byin their patient following a hot bath also seems toLee et al. (1) and wish to comment on some omis-have some features of migraine in terms of sever-sions in their article and also seek their response toity, throbbing nature, and the presence
 rich3/jgp-ajgp/jgp-ajgp/jgp99908/jgp0562-09z
rich3/jgp-ajgp/jgp-ajgp/jgp99908/jgp0562-09z