Rehabilitation Institute of Texas RIT Patient Initial Visit Information Sheet
Patient Name: ____________________________ Age: _______ Gender: M F
Referring Physician: _______________________ Primary Care Physician: ___________________
Reason for the visit: _______________________________________________________________
1. When did your present problem start? _____________________________________________
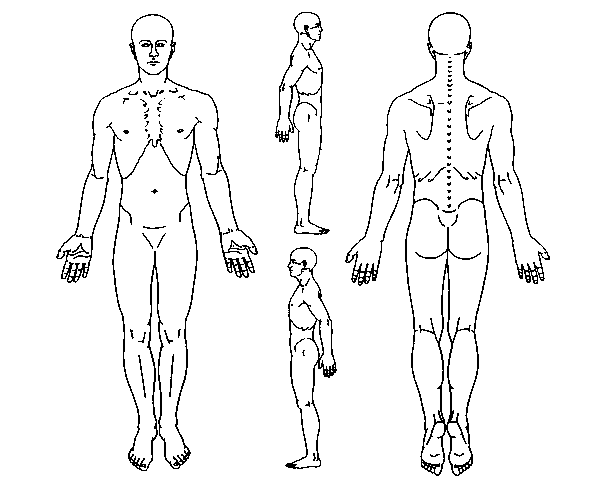
2. How did this problem start? 3. Pain Diagram ___________________________________ On the picture below, please mark all the area of your pain: ___________________________________
4. Pain level: (no pain: 0, worst pain: 10)
Pain right this moment: ________________
Average pain over last 24 hours: _________ 5. Pain quality: (Check below that best describe what you pain feels like)
-Throbbing -Shooting -Stabbing -Sharp -Cramping -Burning -Tingling -Aching
6. Pain pattern: -Continuous -Rhythmic -Comes and goes
7. What can make your pain worse?
-Sitting -Standing -Walking -Lifting -Cough/Sneeze -Lying flat on back -Others:
8. What can make your pain better?
9. Do you have any of following symptoms when you have pain?
-Nausea -Vomiting -Visual disturbance -Weakness -Incontinence -Shortness of breath -Others:
10. Do you have difficulty sleeping because of pain? -Yes -No How many hours a day on average can you sleep recently? ___________________________
11. Have you ever been treated for a different pain condition? -Yes -No If yes, please describe where and when: ___________________________________________________________________________
12. Previous treatment for your current pain -Yes -No Have you ever been to another pain clinic? If yes, Name of the clinic______________ Dr.’s name ________________ Name of the clinic______________ Dr.’s name ________________ Name of the clinic______________ Dr.’s name ________________
-Yes -No Have you had previous injection for your pain? If yes, what kind of injection? ________________________________ Did they help? _________________________________________ -Yes -No Have you had previous surgery for pain? If yes, please explain: _____________________________________
-Yes -No Have you had physical or occupational therapy for pain?
-Yes -No Have you tried acupuncture for pain relief? If yes, was this helpful? _____________
-Yes -No Have you seen a chiropractor for pain relief? If yes, was this helpful? ____________
13. Pain medications Please list all the pain medications you are taking currently (including any nonprescription Medications such as Tylenol, Bengay, etc.)
Please list all the pain medications you took before but for some reasons you have stopped taking these Medications (e.g. Ibuprofen, Naproxen, Motrin, Advil, Predinison, Medrol-dose pack, Vioxx, Celebrex, Bextra, Valium, Flexeril, Baclofen, Neurontin, Tegretol, Elavil, Celexa, Darvon, Darvocet, Roxicet, Percocet, Oxycodone, Oxycontin, Kadian, Ultram, Ultracet etc.).
14. Other medications Are you currently taking other medications for other non-pain health conditions? -Yes -No If yes, please list (be sure to include nonprescription, eye drops, topical drugs such as vitamins
How do you take (example: one tablet twice daily)
15. Please list any drug allergy
16. Past medical history (Please check any of the following problems that you have had)
___ High blood pressure ___ Tuberculosis ___ Diabetes/Hypoglycemia ___ Stomach ulcers
___ Heart Murmur ___ Hepatitis ___ Arrhythmia ___ HIV infection ___ Heart attack ___ Seizure ___ Chest pain ___ Stroke ___ Asthma ___ Fainting ___ Cancer ___ Bleeding disorders ___ Kindney infection/stone ___ Depression ___ Swelling of toe or finger joints ___ Psychosis ___ Thyroid disease ___ Others:
17. Past surgical History (Please list all previous surgeries)
Date (Month/Year) Procedures _______________ __________________________________________________________ _____________ __________________________________________________ _____________ __________________________________________________ _____________ __________________________________________________
18. Social History Are you currently: Single Married Widowed Divorced Separated -Yes -No Do you smoke cigarettes? If yes, ____ packs per day for ____ years? Quit____ -Yes -No Do you drink alcohol beverages? If yes, how much per day? ____ -Yes -No Do you use street drugs? -Yes -No Are you working? How many hours a day? 0 1 2 3 4 5 6 7 8 more If not, when was your last work? Date: _______________ -Yes -No Is this a worker’s compensation case? -Yes -No Are you involved in a lawsuit related to your pain condition? -Yes -No Are you interested to return to work soon, if you are not working currently?
19. Family History Do you have a family history of (Circle all that applies)? -Diabetes -Tuberculosis -Heart attacks -Rheumatoid arthritis -back problems -Others: ______________
20. Review of System Do you have any of the following symptoms recently? Constitutional: -Fever -Weight loss -Sleep difficulty Cardiovascular: -Chest pain -Shortness of breath Respiratory: -Cough -Wheezing -Asthma -Breathing difficulty Gastrointestinal: -Nausea -Vomiting -Abdominal pain -Constipation Genitourinary: -Urine incontinence -Urinary frequency -Pain on urination -Impotence Female reproduction: -Pregnant -Abnormal bleeding Skeletal muscle: -Back pain -Neck pain -Joint pain -Joint swelling Neurological: -Headache -Arm weakness -Hand/leg numbness -Leg weakness -Gait unsteadiness Vision: -Visual difficulty -Glaucoma -Eye pain ENT: -Ear infection -Ear pain Skin: -Rash -Ulcer -Skin cancer -Infection -Hypersensitivity -Color change -Temperature change Immunology: -Rheumatoid arthritis -SLE Psychological: -Depression -Anxiety -Pain attach -Suicidal ideation
Prima di iniziare a parlare della disfunzione erettile vale la pena di spendere alcune parole sul meccanismo dell’erezione . Fare in modo che essa avvenga e’ cosi’ incredibilmente complicato, da un punto di vista fisiologico, che se gli uomini fossero stati costretti a capirne il funzionamento, nessuno di noi sarebbe qui ora. Tuttavia, per fortuna, l’erezione è un processo totalmente
Einsatz des Internet-basierten Tools www.cancerdrugs.ch in der HausarztpraxisInsomnie bei Krebspatienten Insomnie (Schlafstörungen) ist ein häufi ges, aber oft unter- schätztes Symptom bei von Krebs betroffenen Patienten und kann deren Lebensqualität deutlich beeinträchtigen. en nnte Schlafh ygiene ; dar Gemäss ICD-10 spricht man von Insomnie als einem Zustands- vor dem Ei
 Rehabilitation Institute of Texas
Rehabilitation Institute of Texas