For a CME/CEU version of this article please go to http://www.namcp.org/cmeonline.htm, and then click the activity title.
Multiple sclerosis (MS) is a common cause of disability in young adults. Although
not curable, effective immunomodulators, which alter the development of disabil-ity, are available and should be initiated early in the disease process. Optimizingcare of patients with MS requires frequent assessment and a team approach.
• MS is the most common neurological disease that causes disability in young adults. • Therapy with an immunomodulator should be started as soon as possible fol-lowing a definite diagnosis of relapsing remitting MS to slow the developmentof disability. • The goals of MS management are to treat relapses, manage symptoms, mod-ify or reduce relapses, delay progression to disability, and facilitate an accept-able quality of life.
The relapsing remitting stage is where medications
not the most common neurological disease in young
are most effective. In the secondary progressive
adults, it is the most common neurological disease that
phase, there is a loss of brain volume and increasing
causes disability in young adults. It is a chronic illness
evidence of neuron loss on MRI scans. In the earlier
with no cure, but it does not shorten one’s lifespan.
phases, the patient will return back or nearly back to
There are an estimated 350,000 to 500,000 people
baseline after an attack or relapse. As the disease pro-
in North America with MS. About 10,000 new cases
gresses, the patient accumulates damage.
are diagnosed annually.The highest prevalence in the
MRI scanning is very important in diagnosis and
U.S. is among Caucasians, and the female-to-male
in following patients. An MRI scan will demonstrate
ratio is at least 2-to-1 and possibly higher.The usual
approximately 90 to 95 percent of white matter
age of onset is between 15 and 55. The average age
lesions in the brain and 50 to 75 percent of lesions in
the spinal cord. Cost and availability are limiting fac-
Because this disease disables young people, the
tors in repeated MRI scans in the clinical setting.
costs of MS to society are enormous. This was esti-
The National Multiple Sclerosis Society states that
mated at 27 billion dollars about 10 years ago.1
initiation of therapy with an immunomodulator is
MS is an immune mediated disease in genetically
advised as soon as possible after a definite diagnosis
susceptible individuals. It has two aspects, inflamma-
of MS with a relapsing course.2 Therapy may be con-
tory and degenerative, which leads to progressive
sidered for selected patients with a first attack who
neurological dysfunction with lesions in all areas of
are high risk for RRMS.2 Early therapy is intended
the central nervous system, brain, and spinal cord.
to slow both the inflammatory and degenerative
Exhibit 1 illustrates the clinical progression of MS.
aspects of the disease. Treating patients early has a
Initially, there is a preclinical phase where changes
better chance to affect and modulate the immune
can be seen on magnetic resonance imaging (MRI)
system. The goals of pharmacologic therapy in MS
scans. The next stage is a relapsing remitting phase
are given in Exhibit 2. Importantly, control of dis-
where patients will have an attack and get better.
Acute attacks are relapses or episodes with acute
Immunomodulators that are approved for relapsing
neurological dysfunction that last at least 48 hours.
remitting multiple sclerosis (RRMS) include glati-
Journal of Managed Care Medicine | Vol. 10, No. 4 | www.namcp.org
ramer acetate (Copaxone®), interferon beta-1a
different symptoms that also require treatment.
Symptoms of MS occur depending on the locations
(Betaseron“), and natalizumab (Tysabri®) (Exhibit 3).
of the demyelinating plaques in the brain (Exhibit 7).
Natalizumab was briefly withdrawn from the market
For example, plaques in the cerebellum can cause
because of several cases of progressive multi-focal
ataxia or tremors. The typical symptoms of MS
leukoencephalopathy, which can be fatal. It was
include fatigue, spasticity, pain, bowel & bladder
recently reintroduced to the market. Mitoxantrone
problems, memory loss, swallowing difficulties,
(Novantrone®), a chemotherapeutic agent, and corti-
tremors, visual changes, sexual dysfunction, speech
costeroids are used as immunosupressants in relapsing
disorders, balance and mobility dysfunction, and
forms of MS. Patients at times will respond to one
depression. Treating these symptoms improves the
agent and not to another. All of the FDA-approved
patient’s quality of life. Symptom management
immunomodulators reduce the number of relapses.
includes nonpharmacologic therapies, pharmacolog-
Among untreated patients, 50 percent will reach a
ic therapies, and psychological support.
level of disability, requiring assistance with walking,
Fatigue is a common symptom that may require
within 15 years (expanded disability status scale [EDSS]
lifestyle changes. For example, patients are taught to
score of 6, Exhibit 4).3 Data shows glatiramer acetate
integrate rest times during their daily activities.
and interferons alter the natural history of this disease.4-
6 For example, in one glatiramer study, only 8 percent
(Symmetrel®), modafinil (Provigil®), and antidepres-
of patients progressed to an EDSS of 6 at 10 years.7
sants. None of these agents are FDA approved for
Although these medications can decrease disability,
treating fatigue of multiple sclerosis.
they are not without side effects. The major adverse
Spasticity affects 60 to 80 percent of patients.
effects of the agents are given in Exhibit 5.
Nonpharmacologic interventions to manage spastic-
Glatiramer acetate causes less significant adverse
ity include stretching, bed and chair positioning, and
events, which is very important for patient quality of
physical therapy. Pharmacologic interventions, in
life. Additionally, glatiramer has a pregnancy catego-
addition to monpharmacologic measures, are most
ry B labeling (safe in animals, no human data) versusC (adverse events in animals) or D (known fetal risk)for the other agents. Since women are diagnosed
with MS more often than men, this distinction
• Affect the neurodegenerative & inflammatory
Untreated, almost half of the patients will not fully
recover from an acute attack. It is very important to
• Early intervention: initiate therapy as soon as possible
treat acute attacks to prevent or reduce long-term dis-
for the best chance of controlling damage
ability. High dose intravenous corticosteroids are the
• Reduction of disease activity as measures by relapses,
standard treatment. In the past, this treatment would
have required a three-to-five-day hospital stay. Now,
• Provision of therapy that is well tolerated & safe
this treatment is almost exclusively given in the home.
In addition to acute attacks, patients have many
www.namcp.org | Vol. 10, No. 4 | Journal of Managed Care Medicine 35
Exhibit 3: EDSS: Progression to Disability
8.0-8.5 = Confined to bed/chair; self-care with help
5.0-5.5 = Increasing limitation in ability to walk
commonly used.The typical agents include baclofen,
tion can be managed with intermittent self-catheter-
ization; medications such as antispasmodics, tricyclic
(Dantrium®), nerve blocks with various agents, and
antidepressants, DDAVP (an antidiuretic hormone),
botulinum toxin (Botox®). Surgical interventions
and alpha blockers; and, if necessary, indwelling
include baclofen pumps and rhizotomy.
catheters. With bowel dysfunction, constipation and
Various types of pain occur with multiple sclerosis.
fecal incontinence are the most common problems.
Nonpharmacologic management of pain includes
Constipation is treated with fiber, fluids, activity,
appropriate seating support to improve posture, physical
bowel training, laxatives, and dietary modification.
therapy, gait training, assistive devices, muscle strength-
Involuntary loss of bowel control can be treated with
ening, and stretching. When treating pain, many phar-
fiber, anticholinergics, and dietary modification.
macologic agents are used off label. The most com-
Because of brain shrinkage, cognitive issues occur
monly used agents include amitriptyline (Elavil®), nor-
in 45 to 60 percent of patients, but result in signifi-
triptyline (Pamelor®), carbamazepine (Tegretol®),
cant changes in only 15 percent of patients.8,9 Early
gabapentin (Neurontin®), phenytoin (Dilantin®),
treatment to minimize the number of acute attacks
baclofen, tizanidine, and clonazepam (Klonopin®).
will prevent this shrinkage. The most common cog-
More than half of the patients with MS have issues
nitive issues are short-term memory loss or impaired
with their bladder or bowels, which are very dis-
judgment, learning, word finding, or executive func-
abling. Aggressive management of bladder dysfunc-
tioning. Neuropsychological testing is used to iden-
tion is necessary because untreated bladder dysfunc-
tify and monitor cognitive issues related to MS. A
tion can lead to chronic infections. Bladder dysfunc-
brain defect secondary to the disease needs to be dis-
Exhibit 4: Disease-Modifying Therapy Indications & Administration
*May be administered only by specialty trained healthcare professionals trained in the TOUCH program.
Journal of Managed Care Medicine | Vol. 10, No. 4 | www.namcp.org
Tremor and unsteadiness are two MS symptoms
difficult to treat. Various medications can be triedincluding carbamazepine, ondansetron (Zofran®),
clonazepam, primidone, gabapentin, propranolol, tri-
cyclic antidepressants, and levetiracetam (Keppra®).
Optimizing therapy requires regular clinical assess-
ment of patients. Therapies need to be evaluated for
effectiveness and adverse effects. Therapy may need to
- Liver function and bone marrow abnormalities
be changed periodically for several reasons.The medi-
cations currently available are not all effective in every
patient, and are only partially effective in many cases.
Disease progression may not be well controlled in some
- Risk for life-threatening PML necessitates prescription
patients. Additionally, the development of neutralizing
only through special risk management program
antibodies may compromise efficacy of the interferons. Switching or combining therapies is routinely practiced
although well-designed study data are limited.
Optimizing therapy also has to include the patient.
Patients need to be educated about their disease andits therapies.Adherence with the prescribed therapiesneeds to be monitored and maintained.
Exhibit 6: MS Symptoms Correspond to Brain Regions
Appropriate care of the patient with MS involves a
team approach using many different medical profes-
Symptoms vary widely in incidence and severity
sionals.Vocational counselors can be most helpful in
assisting the patient with adjusting their workplace tomanage many of the symptoms such as pain and
fatigue. Physical therapists work with the patient to
manage many of the symptoms. Nutritionists assistpatients with maintaining an appropriate diet.
Keeping these patients active, productive members of
MS is a disease of an overactive immune system
resulting in inflammation and neurodegeneration.
Early treatment of this disease may delay progression. Optimizing nonpharmacologic and pharmacologic
tinguished from depression. Treatment may include
therapy requires frequent assessment and a team
occupational therapy and cognitive retraining.
approach. JMCM
Medications, approved for use in Alzheimer’s disease,occasionally are used but have minimal efficacy.
Howard Zwibel, MD, is a neurologist and medical director at the
Depression is common in patients with MS. Like
HealthSouth Doctor’s Hospital Comprehensive Multiple Sclerosis Centerin Coral Gables, Fla.
many of the other symptoms of MS, depressioncontributes to a reduced quality of life. The same
antidepressants are used in these patients as in
1. Paty DW, Ebers GC, eds. Multiple Sclerosis. Vol. 50 Contemporary NeurologySeries. Philadelphia; FA Davis, 1998.
2. National Multiple Sclerosis Society. Disease Management Consensus Statement.
Sexual dysfunction is an issue that physicians
Accessed August 2, 2007. Available at www.nationalmssociety.org. 3. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded dis-
often avoid discussing with the patient. Sexual dys-
ability status scale (EDSS). Neurology. 1983;33:1444-1452.
function must be addressed because it can disrupt
4. Kappos L,Traboulsee A, Constantinescu C, et al. Long-term subcutaneous inter-feron beta-1a therapy in patients with relapsing-remitting MS. Neurology.
family life and quality of life. Management strate-
gies include medications for impotence (vardenafil
5. Ebers GC. Disease evolution in multiple sclerosis. J Neurol. 2006;253(Suppl 6):vi3-vi8. 6. Fisher E, Rudick RA, Simon JH, et al. Eight-year follow-up study of brain atro-
[Levitra®], tadalafil [Cialis®], sildenafil [Viagra®]),
phy in patients with MS. Neurology. 2002;59:1412-1420.
management of other symptoms or medical condi-
7. Ford CC, Johnson KP, Lisak RP, et al. A prospective open-label study of glati-ramer acetate: over a decade of continuous use in multiple sclerosis patients. Mult
tions that may be contributing, adjustment of med-
ications that may be contributing, mechanical assis-
8. Prosiegel M, Michael C. Neuropsychology and multiple sclerosis: diagnostic andrehabilitative approaches. J Neurol Sci. 1993;115:S51-S54.
tive devices, and emotional support.
9. Rao SM. Neuropsychology of multiple sclerosis. Curr Opin Neurol. 1995;8:216-220.
www.namcp.org | Vol. 10, No. 4 | Journal of Managed Care Medicine 37
30th Charles A. Coltman San Antonio Breast Cancer Symposium (SABCS) December 13-16, 2007, SanAntonio, Texas, USA Ion Chiricuta Cancer Center Cluj-Napoca, Dept. of Breast Tumors The 30th Charles A. Coltman San Antonio Breast Cancer Symposium (SABCS) took place on December 13-16, 2007, in San Antonio, Texas. Important clinical and research data presented during this prestigious meeting
Kendall A, Dowsett M, Folkerd E, Smith I. Caution: Vaginal estradiol appears to be contraindicated in postmenopausal women on adjuvant aromatase inhibitors. Ann Oncol 2006 17(4):584-7. PMID: 16443612 Laumann EO, Nicolosi A, Glasser DB, Paik A, Gingell C, Moreira E, Wang T; GSSAB Investigators' Group. Sexual problems among women and men aged 40-80 y: prevalence and correlates identified in the Glob
 For a CME/CEU version of this article please go to http://www.namcp.org/cmeonline.htm, and then click the activity title.
For a CME/CEU version of this article please go to http://www.namcp.org/cmeonline.htm, and then click the activity title.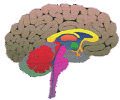 Tremor and unsteadiness are two MS symptoms
difficult to treat. Various medications can be triedincluding carbamazepine, ondansetron (Zofran®),
clonazepam, primidone, gabapentin, propranolol, tri-
cyclic antidepressants, and levetiracetam (Keppra®).
Tremor and unsteadiness are two MS symptoms
difficult to treat. Various medications can be triedincluding carbamazepine, ondansetron (Zofran®),
clonazepam, primidone, gabapentin, propranolol, tri-
cyclic antidepressants, and levetiracetam (Keppra®).