The use of prolotherapy in the sacroiliac joint
M Cusi, J Saunders, B Hungerford, et al.
2010 44: 100-104 originally published online April 9, 2008
Br J Sports Meddoi: 10.1136/bjsm.2007.042044
Updated information and services can be found at:
References
This article cites 21 articles, 3 of which can be accessed free at:
Email alerting
Receive free email alerts when new articles cite this article. Sign up in the
box at the top right corner of the online article. Original article
The use of prolotherapy in the sacroiliac joint
M Cusi,1 J Saunders,2 B Hungerford,3 T Wisbey-Roth,4 P Lucas,2 S Wilson1
anaesthetic SIJ blocks in a low-back pain popula-
Objective: In this study the effectiveness of prolotherapy
tion. Fifty-four patients completed the study, of
in the treatment of deficient load transfer of the sacroiliac
whom 10 (18.5%) were considered as having pain
Programs, University of NewSouth Wales, Sydney, New
originating from the SIJ.10 Given that the injections
Design: A prospective descriptive study.
were administered into the synovial part of the
Setting: Authors’ private practice.
joint and did not involve the posterior ligaments, it
Participants: 25 patients who consented to treatment
is possible that the SIJ is responsible for chronic
low-back pain in a higher proportion of individuals.
and attended for at least one follow-up visit and
The purpose of this study is to examine whether
Study period: From April 2004 to July 2007.
prolotherapy injections into the dorsal interosseous
Intervention: Three injections of hypertonic dextrose
ligament of the SIJ (fig 1) can assist patients with a
clinical diagnosis of deficient stability of the SIJ
solution into the dorsal interosseous ligament of the
affected SIJ, under CT control, 6 weeks apart.
that fails to respond to specific exercise therapy.
Main outcome measures: Quebec Back Pain Disability
The null hypothesis is, therefore, that prolotherapy
injections, in addition to exercise therapy, do not
Scale, Roland–Morris 24, Roland–Morris 24 Multiform
questionnaires and clinical examination by two authors
improve the clinical examination parameters or
Results: All patients included in this study attended atleast one follow-up visit at 3, 12 or 24 months. The
number of patients at follow-up decreased at 12 and
Patients were recruited from the private practices
24 months. Functional questionnaires demonstrated sig-
of two sport and exercise medicine (SEM) physi-
nificant improvements for those followed-up at 3, 12 and
cians and two physiotherapists. Patients who
24 months (p,0.05). Clinical scores showed significant
fulfilled the entry criteria were invited to partici-
improvement from commencement to 3, 12 and
pate in the prospective study after the treatment
programme was explained in detail. Verbal and
Conclusions: This descriptive study of prolotherapy in
written information was provided before patients
private practice has shown positive clinical outcomes for
were asked to make a separate appointment to give
the 76% of patients who attended the 3-month follow-up
their written consent once they had their questions
visit (76% at 12 months and 32% at 24 months). Similar
answered and had reached a decision. This study
results were found in the questionnaires (Quebec Back
was conducted as a practice quality project and as
Pain Disability Scale, Roland–Morris 24 and Roland–
such did not require ethics approval or trial
Morris 24 Multiform questionnaires) at 3, 12 and
Maintenance of Professional Standards (MOPS)activity of the Australasian College of SportsPhysicians.
Prolotherapy treatment has been advocated for a
Entry criteria included a diagnosis of persistent
variety of soft tissue conditions, including non-
suboptimal stability of the SIJ following a 3-month
specific low-back pain, chronic musculoskeletal
specific exercise programme. This diagnosis had to
pain and hypermobility of joints.1 2 The goal of
be made independently by a SEM physician (MC
this therapy is to produce dense fibrous tissue to
and JS) and a physiotherapist (BH and TWR)
strengthen the attachment of ligaments, tendons,
joint capsules and other fascial structures at their
Clinical history included localised and/or radiat-
fibro-osseous junctions.3 Prolotherapy has been
ing low back or buttock pain in the vicinity of the
defined as ‘‘the rehabilitation of an incompetent
posterior superior iliac spine, worse on loading
structure (as a ligament or tendon) by the induced
positions such as standing, sitting, walking or
proliferation of new cells’’.4 This procedure was
negotiating stairs. Symptoms had to be present for
initially used for treatment of spinal pain in the
a minimum of 6 months before the initial assess-
1930s. Its use continues despite the controversy
ment. Exclusion criteria were acute radiculopathy,
that has surrounded it. A frequent indication is
infection, pregnancy, inflammatory conditions of
spinal or low-back pain. The injection techniques,
substances used, volumes injected and the site or
The clinical tests used were the SIJ glide test
(anteroposterior and vertical arm, with and without
The sacroiliac joint (SIJ) is a source of pain in the
self-bracing),11 posterior pelvic pain provocation test
lower back and buttocks in up to 15% of the
(PPPP),12 active straight leg raise (ASLR)13–15 with and
population,7 and there is evidence that dysfunction
without self–bracing, and external manual compres-
of this joint could, similar to a herniated lumbar
sion and stork support (Gillett) test.16 A score of 1
disk, produce pain along the same distribution as
was given for each positive finding. Clinical tests
the sciatic nerve.8 9 Schwarzer et al10 administered
were, therefore, not graded. Maximum score was 9. Br J Sports Med 2010;44:100–104. doi:10.1136/bjsm.2007.042044 Original article
localised using the CT slice laser and axis/distance functionfrom the scanner and marked on the skin with a pen. The skinwas prepared with antiseptic Betadine and alcohol. The skinwas then anaesthetised with 3 ml of 1% Xylocaine.
The prolotherapy solution was prepared by drawing into a 5-
ml syringe 1.8 ml of 50% glucose solution, 2.3 ml of bupivicaine1% and 0.8 ml of Isovue (iopamidol) 300 contrast (approxi-mately), and 0.8 ml was injected into the ligament.
After allowing time for the local anaesthetic to work, a 22-g
spinal needle was inserted with the appropriate angle and depthto the interosseous ligament, as close to its ilial attachment aspossible. Once the needle was in place, 0.8 ml of theprolotherapy solution was injected as the needle was movedup and down in the ligament (fig 2). Care was taken to ensurethat only the ligament was injected but not the auricularsynovial portion of the joint.
After the procedure, patients were asked to keep pain records
for 14 days. They were also given specific warnings aboutpossible complications such as bruising and the rare possibilityof infection. No adverse effects were reported.
RESULTSTwenty-five patients were treated between 2004 and 2007, witha 26-month average follow-up after injection (range 6–39 months). There were 5 male and 20 female patients(table 1). Their average age was 40.4 years (range 26–67 years). One male patient was lost to follow-up after 12 months whenhe moved to another country; two others have had no formal
(A) Posterior and (B) axial views of the SIJ. Auricular part of
follow-up assessments but remained asymptomatic when
the joint (arrow). The superficial posterior ligaments are not depicted.
contacted by phone. Two patients withdrew from follow-upat 2 years because of unrelated medical causes. Their scores had
Twenty-five patients entered in the study after the exercise
also improved considerably. One male patient received a fourth
programme had shown no benefit. They underwent three
injection in the sacrotuberous ligament, which successfully
injections of prolotherapy solution 6 weeks apart. They were
treated what were considered to be residual instability
assessed within 24 h before each injection by both SEM
physician and physiotherapist, and 1 week after each injection.
The main outcome measures were the negative findings in
They continued to carry out the exercise programme under
the clinical examination (patients had improved clinically)
physiotherapist supervision. They filled in pain maps, the
carried out independently by two of the authors (one SEM
Quebec Back Pain Disability Scale, Roland–Morris 2417 and
physician and one physiotherapist), the Quebec Back Pain
Roland–Morris 24 Multiscale Disability questionnaires at the
Disability Scale, and Roland–Morris 24 and Roland–Morris 24
point of entry and periodically over the following 2 years. They
Multiform questionnaires. Statistical analysis was carried out
were weaned from non-steroidal anti-inflammatory medication
with SPSS software version 5 (SPSS, Chicago, Illinois).
before the first injection and for the duration of the treatment.
Nine clinical testing manoeuvres were performed independently
Written informed consent was obtained in every case. All
by two examiners, and a consensus score was given. Each
injections were done under CT control, by the same radiologist
positive test was given a score of 1. Maximum clinical score was
(PL), on a Siemens Somoton plus 4 CT scanner, according to the
9. If a particular testing manoeuvre was not done, it was scored
0. Scores were analysed with the Student t test for matched
The patient was positioned in the CT scanner with head first,
pairs. Clinical scores on entry into the programme averaged 7.2
in prone position. Pillows were placed under chest and ankles,
(range 4–9, SD 1.5) at the point of decision to proceed to
the head resting on forearms and the face clear of the pillow.
injections. The mean clinical scores showed a significant
Gentle respiration was allowed. Axial slices 5 mm apart were
decrease of 4.5 points at 3 months, 5.0 points at 12 months
obtained over the sacral area, and the appropriate level was
(p,0.001) and 6.5 points at 2 years from the commencement
selected for injection. The entry point on the patient was
score before treatment (see table 1).
Clinical scores at 3, 12 and 24 months using t test for matched pairs
Br J Sports Med 2010;44:100–104. doi:10.1136/bjsm.2007.042044 Original article
Quebec Back Pain Disability Scale Scores at commencement, 3, 12 and 24 months using t test for
Interestingly, there was improvement before the course of
injections was finished. Some changes were noted after the first
Prolotherapy has been advocated in the treatment of low-back
injection and more marked improvement after the second
pain for many years. However, its published results have not
injection. The PPPP test was the first one to become normal and
been consistent. A large, well-conducted randomised controlled
ASLR was the last. However, when the ASLR test was
trial concluded that prolotherapy was no better than the
combined with self-bracing and/or external compression of
injection of normal saline.20 A Cochrane Collaboration report
the anterior superior iliac spines by the examiner, it was normal
concluded that, ‘‘There was no evidence that prolotherapy
in 80% of cases by the time the third injection was given. The
injections alone were more effective than control injections
SIJ glide test results improved earlier. The stork test was
alone, but in the presence of co-interventions, prolotherapy
negative in two-thirds of the patients at the time of the third
injections were more effective than control injections, more so
when both injections and co-interventions were controlledconcurrently’’.21
Most studies that involve the use of prolotherapy in the
treatment of spinal pain do not consider a specific clinical
diagnosis for patient selection. Patient selection is based mainly
The mean total score for the Quebec Back Pain Disability Scale
on pain symptoms in the low back region, and the injections are
at commencement was 58.1 (SD 19.4). The 3-month post-
given in the painful sites. Injected volumes depend on the
treatment scores were significantly improved by 20.7 points
number of sites injected. This could explain the inconsistency of
(95% confidence interval (CI) 11.3 to 30.1, p,001). At
results,20 as there is no evidence that the proliferation of soft
12 months post-treatment, the improvement was 18.2 points
tissue is analgesic per se. However, if injury to specific
(95% CI 7.8 to 28.6, p,0.002), and at 24 months, 33.3 points
structures, such as ligaments or fascia, can be related to a
(95% CI 13.7 to 52.9, p,0.006). The improvement in Quebec
specific clinical presentation and subsequent loss of function
Back Pain Disability Scale scores remained significant at
associated with pain, a case could be made for the use of
12 months and 2 years (see table 2).
prolotherapy. It is important, however, that appropriatetreatment protocols conducted by clinicians experienced in the
Roland–Morris Back Pain Questionnaire (RMQ)
effective rehabilitation of pelvic disorders be trialled before
The mean total score for the RMQ at commencement was 13.3
(SD 5.0). The 3-month post-treatment scores were significantly
Understanding the role of the SIJ has improved in recent
improved by 6.1 points (95% CI 3.0 to 9.2, p = 0.001).19 25 28 At
years. The muscular contribution to the dynamic stability of the
pelvis has been verified in vivo.22 In the presence of pain, there is
points (95% CI 0.0 to 5.0, p,0.047) and at 24 months, 4.4
evidence of altered muscle-recruiting patterns and altered load
points (95% CI 0.8 to 15.7, p,0.035). The improvement in
transfer.23 Symptoms and muscle-recruiting patterns can
RMQ scores remained significant at 12 months and 2 years (see
improve with appropriate exercise therapy.24 25 Clinical tests
exist to examine the load transfer function of the SIJ.13–15 Incases where deficient stability of the SIJ has been established,
Roland–Morris 24 Multiform Questionnaire
clinical experience suggests that specific exercise programmes
The mean total score for the Roland–Morris 24 Multiform
designed to increase lumbopelvic stability may not be sufficient
Questionnaire at commencement was 151.4 (SD 55.0). The 3-
to decrease pain and improve function.
month post-treatment scores were significantly improved by
It has been suggested that when specific exercise programmes
61.5 points (95% CI 30.0 to 93.0, p = 0.001). At 12 months
fail, deficient ligament strength of the posterior elements of the
post-treatment, the improvement was 37.9 points (95% CI 8.2
SIJ does not provide a sufficiently stable base to permit an
to 67.7, p,0.016) and at 2 years, 90.0 points (95% CI 27.1 to
effective muscle recruiting strategy.26 A mechanism that
152.9, p = 0.012). The improvement in Roland–Morris 24
increases the passive functional stiffness of the joint would
Multiform Questionnaire scores remained significant at
contribute to effective muscle recruitment to improve dynamic
12 months and 2 years (see table 4).
stability of the pelvis. In these cases, the increased ligamentous
Roland–Morris Questionnaire Scores at commencement, 3, 12 and 24 months using t test for
Br J Sports Med 2010;44:100–104. doi:10.1136/bjsm.2007.042044 Original article
Roland–Morris Multiform Questionnaire Scores at commencement, 3, 12 and 24 months using
stiffness would have the effect of providing a more stable
Ongley et al.28 Yelland et al20 also found no significant difference
anchor for specific strengthening programmes to produce the
between prolotherapy and normal saline injections for non-
desired outcome. Experimental work in rats27 indicates that
specific low-back pain; however, diagnosis, indications, injec-
prolotherapy is effective in building up collagen fibres and, thus,
tion sites and frequency of injections varied significantly to the
The clinical tests chosen were those used normally by the
Patients in our study were only included when a diagnosis of
authors in their clinical daily work. Most of them have been
failure of load transfer through the SIJ was made. The
referenced in the literature11 13–15 23 and are specific for the SIJ.
theoretical intended effect of the injections was to increase
The results of the main tests (PPPP, active SLR and stork tests)
the stiffness of the dorsal interosseous ligament (fig 2). The
showed similar progression from altered to normal. In parti-
clinical results appear to confirm the hypothesis. The mechan-
cular, the ASLR became normal earlier, before the end of the
ism of action of prolotherapy is not sufficiently understood and
injection period, when patients actively braced their abdomen
requires further study: an inflammatory response could be
or external lateral compression of the pelvis was applied by the
triggered by a mechanical insult (volume of fluid injected), by
examiner. Two-thirds of the patients had normal results for the
an osmotic effect or by neural pathways (needle in position).
clinical tests by the time they had the third injection, and thepatient feedback was that pain levels had decreased and
function increased. This is reflected in the questionnaires scores,
The strength of this study is that there were no incentives or
which were only done 3 months after the third injection was
secondary gains for patients attending follow-up. Patients were
either privately funded or funding was approved by the relevant
This is a novel study of prolotherapy in patients with spinal-
insurance company in work-related cases (n = 5).
related pain where the indication for treatment was loss of
The weakness of the study is that patients acted as their own
function from a specific clinical diagnosis, not pain alone. The
controls and there was no non-intervention control group.
solution injected (hypertonic dextrose) was easily obtainable
There was an insufficient cohort of control patients who fitted
and is a common solution used for prolotherapy injections. The
the criteria of entry but did not undergo the three injections and
time between injections (6 weeks) was based on the assumption
were, therefore, not entered for statistical analysis.
that the inflammatory reaction and formation of collagen takesup to 7 or 8 weeks, and it is not necessary for the injections to
follow each other closely. Three injections were considered
This descriptive study of the use of prolotherapy in combination
sufficient to ensure a reasonable length of time for collagen
with a specific exercise programme in private practice has
shown improvement in clinical outcome scores for all the
Ongley et al28 carried out a study of prolotherapy on patients
patients who attended follow-up visits: 76% of patients
with chronic low-back pain. There are major differences
(n = 19) had been followed-up at 3 months, 76% (n = 19)
between Ongley’s randomised control trial and our study. The
at 12 months and 32% (n = 8) at 2 years. Three other patients
diagnosis was different, individuals had a variety of different
were verbally contacted at 12 months and reported good clinical
combined treatments in both groups, and the location andfrequency of injections were also vastly different. It is, therefore,difficult to compare the results of this study with those of
Prolotherapy acts by creating an inflammatory response. It hasbeen used for a long time in the treatment of axial pain. Thediagnosis is generally non-specific low-back pain, and theinjection technique, substances, volumes and sites injected varyfrom author to author, and the results, so far, have beeninconclusive.
This is the first study that uses coherent injection techniques toinfiltrate specifically the ligamentous structures of the SIJ. Theindication for prolotherapy is not pain but a specific clinicaldiagnosis following strict criteria. The site of injection is also very
Prolotherapy solution and needle in situ. Solution injected
precise and a very small volume is injected.
only in the deep interosseous ligament. Br J Sports Med 2010;44:100–104. doi:10.1136/bjsm.2007.042044 Original article
outcomes but were not assessed and, therefore, not included in
Schwarzer AC, Aprill CN, Bogduk N. The sacroiliac joint in chronic low back pain. Spine 1995;20:31–7.
the statistical analysis. Similar results were found in the
Lee D. The pelvic girdle. 3rd ed. London: Churchill Livingstone, 2004.
functional questionnaires used in the study at 3 and 12 months
Ostgaard HC, Zetherstrom G, Roos-Hansson E. The posterior pelvic pain provocation
and 2 years. This study also showed that it is possible to make a
test in pregnant women. Eur Spine J 1994;3:258–60.
clinical diagnosis of SIJ-deficient load transfer of ligamentous
Mens JM, Vleeming A, Snijders CJ, et al. The active straight leg raising test andmobility of the pelvic joints. Eur Spine J 1999;8:468–73.
origin. Treatment with CT-guided prolotherapy injections in
Mens JMA, Vleeming A, Snijders CJ, et al. Active straight-leg-raise test: a clinical
the dorsal interosseous ligament of the affected SIJ—in
approach to the load transfer function of the pelvic girdle. In: Vleeming A, Mooney V,
combination with specific core stability training—can success-
Dorman T, eds. Movement, stability and low back pain: the essential role of the pelvis. Edinburgh: Churchill Livingstone, 1997:425–31.
fully correct the deficiency, reduce pain and improve function.
Mens JMA, Vleeming A, Snijders CJ, et al. Reliability and validity of
The results of this intervention trial warrant further research
the active straight leg raise test in posterior pelvic pain since pregnancy. Spine
Hungerford B, Gilleard W, Moran M, et al. Evaluation of the ability of physicaltherapists to palpate intrapelvic motion with the stork test on the support side. Phys
Acknowledgements: The authors thank Daniel Wasson, senior CT technician, of the
RNSH Private Medical Imaging Department for his assistance with all injections.
Roland M, Fairbank J. The Roland–Morris Disability Questionnaire and the Oswestry
Disability Questionnaire. Spine 2000;25:3115–24.
McCallum M. Protocol for prolotherapy into the DIOL of the SIJ. Personal
Ethics approval: This study was conducted as a practice quality project and as such
did not require ethics approval or trial registration.
Stratford PW, Binkley JM, Riddle DL, et al. Sensitivity to change of the Roland–
Morris Back Pain Questionnaire: part 1. Phys Ther 1998;78:1186–96.
Yelland MJ, Glasziou PP, Bogduk N, et al. Prolotherapy injections, saline injections,and exercises for chronic low-back pain: a randomized trial. Spine 2004;29:9–16.
Yelland MJ, Yelland MJ, Del Mar C, et al. Prolotherapy injections for chronic low-
Hackett GA. Ligament and tendon relaxation treated by prolotherapy. Springfield, IL:
Van Wingerden JP, Vleeming A, Buyruk HM, et al. Stabilization of the sacro-iliac
Klein RG, Eck B. Prolotherapy: an alternative approach to managing low back pain.
joint in vivo: verification of muscular contribution to force closure of the pelvis. Eur
J Musculoskeletal Med 1997;14:45–9.
Liu YK, et al. An in situ study of the influence of a sclerosing solution in rabbit medial
Hungerford B, Gilleard W, Hodges P. Evidence of altered lumbopelvic muscle
collateral ligaments and its junction strength. Connect Tissue Res 1983;11:95–102.
recruitment in the presence of sacroiliac joint pain. Spine 2003;28:1593–600.
Gove P. Third new international dictionary. Unabridged. Springfield, MA: Merriam-
O’Sullivan PB. Lumbar segmental ‘instability’ clinical presentation and specific
stabilizing exercises. Man Ther 2000;5:2–12.
Dagenais S, Haldeman S, Wooley J. Intraligamentous injection of sclerosing
Stuge B, Veierod MB, Laerum E, et al. The efficacy of a treatment program focusing
solutions (prolotherapy) for spinal pain: a critical review of the literature. Spine J
on stabilising exercises for pelvic girdle pain after pregnancy: two-year follow-up of a
randomized clinical trial. Spine 2004;29:E197–203.
Banks A. A rationale for prolotherapy. J Orthop Med 1991;13:54–9.
Poul-Goudzwaard AL, Hoek van Dijke G, Mulder P, et al. Insufficient lumbopelvic
Dreyfuss P, Dreyer SJ, Cole A, et al. Sacroiliac joint pain. J Am Acad Orthop Surg
stability: a clinical, anatomical, and biomechanical approach to ‘‘a specific’’ low back
Fortin JD, Aprill CN, Ponthieux B, et al. Sacroiliac joint: pain referral maps upon
Liu YK, Tipton CM, Matthes RD, et al. An in situ study of the influence of a sclerosing
applying a new injection/arthrography technique. Part II: clinical evaluation. Spine
solution in rabbit medial collateral ligaments and its junction strength. Connective
Fortin JD, Vilensky JA, Merkel GJ. Can the sacro-iliac joint cause sciatica? Pain
Ongley MJ, Klein RG, Dorman TA, et al. A new approach to the treatment of chronic
Br J Sports Med 2010;44:100–104. doi:10.1136/bjsm.2007.042044
ALLERGY & ASTHMA CLINICS OF GEORGIA, P.C. _______________________________________________ PATIENT HANDOUT for ECZEMA (also known as ATOPIC DERMATITIS) What is eczema? Eczema is a chronic condition with acute flares and periods of remission. It is often the first manifestation of a group of allergic disorders that includes asthma, allergic rhinitis, and food allergy . The
Envois internationaux bpack World Liste des zones et des délais indicatifs (en jours) pour les vil es principales Délais1 Poids Max. Particularités Afghanistan Afrique du Sud Café, graines, thé, tabac, plantes, textiles, pièces de bateau, … Algérie Alcool, parfums, échantillons médicaux, plantes, … Allemagne Antiquités, cosmétiques, fourrures, jeux de
 The use of prolotherapy in the sacroiliac joint
The use of prolotherapy in the sacroiliac joint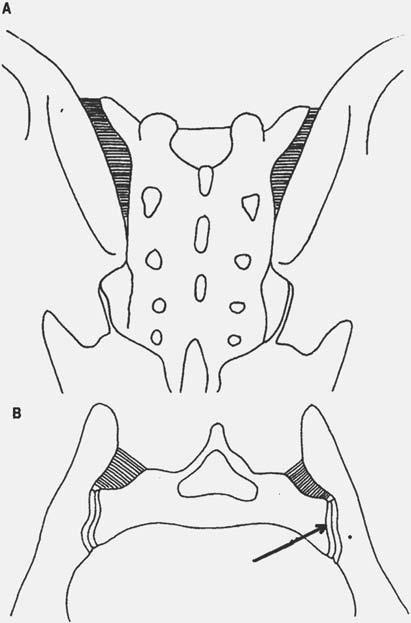 Original article
Original article Original article
Original article