Users and abusers of psychiatry: a critical look at psychiatric practice, second edition
Women’s and men’s role problems and psychiatry
The story of a depressed housewife
This is the story of Elaine Jones, who is typical of very many womenwho break down and are taken into psychiatric hospitals. ELAINE’S STORY
Elaine is 46, married with four children. Her husband is a vandriver for a local firm, where she worked as a cleaner before hermarriage. She is warm, outgoing and intelligent, and cares verydeeply for her family. Generally she seems to cope well with herlife, which since her marriage has consisted mainly of looking afterher husband and children.
However, six months after the birth of her last child fifteen years
ago, she suffered the first of many recurring episodes of depression,which have often been so severe that she has tried to kill herself. Shehas had over twenty admissions to psychiatric hospitals, varying inlength from a few days to several months. Her treatment hasconsisted mainly of medication; she has been prescribed twentydifferent drugs, and has been taking at least one of them ever sinceher first breakdown. She has also had ECT (electro-convulsivetherapy). While in the occupational therapy department, she hasfollowed programmes of cooking and sewing, pottery and art. Noneof this has prevented her from breaking down again, sometimes onlyweeks or months after being discharged.
On Elaine’s twenty-second admission, a new member of the
psychiatric team, hearing that she had had a very unhappy childhood,suggested that she might benefit from a different treatment approach.
This new team member was prepared to offer Elaine psychotherapysessions to try and understand the background to and reasons for herdepression. The consultant, who had had a lot of contact with Elaineover the past ten years, was not keen on this idea. He was inclined tobelieve that Elaine was not so much depressed as seeking an escapefrom chores at home, and pointed out that a few weeks afteradmission she usually appeared looking perfectly cheerful and askingto be discharged. However, he eventually agreed to the new plan.
Elaine, too, had mixed feelings about starting psychotherapy. She
knew very little about it, and in any case she and her family had beentold by her doctors that her depression was due to a recurrentillness. She found the idea of looking too closely at her feelingsrather frightening. Nevertheless, she wanted to try anything thatmight help.
In the first session, Elaine started to reveal the depression behind
the brave face that she felt compelled to put on for the world. Eversince childhood she had been known as the ‘strong one’, and she felttremendously guilty about not being able to be strong for her familyall the time. Although the battle had often been horrific, she hadforced herself to carry on through many bouts of depression withoutcoming into hospital. Sometimes she had vomited because of thestrain of preparing herself for family gatherings; but not wanting tolet people down, she somehow got through them without her socialfaçade cracking. At other times, however, she reached the pointwhere even washing a plate seemed like climbing a mountain, andshe collapsed and retreated to bed in an extremity of exhaustion,guilt and despair.
Elaine also described how hurt she was that others did not
understand how she felt. Her brother slammed down thetelephone one night when for once she rang for help. Tears cameto her eyes as she recalled the incident. But she expressednothing but gratitude to the hospital for taking her in so often. The consultant insisted on discharging her once after a three-month stay when she had not improved at all, and although shehad thought she would not be able to stand it, she had struggledthrough in the end. At the time she had thought him harsh, butlooking back she was grateful for his firmness.
In that initial session, Elaine also revealed for the first time the
incident that precipitated her first breakdown. She had been feeling
very low after the birth of her third child, when some homelessrelatives and their children arrived on the doorstep. She and herhusband had felt obliged to take them in, and most of the burden oflooking after two families in a medium-sized council house had fallenon Elaine’s shoulders. The visiting husband started drinking heavily,and the whole family departed after six months without a word ofthanks. Elaine broke down shortly afterwards.
In twice-weekly meetings over the next four months, Elaine and
her therapist continued to trace the roots of her depression. Atheme that emerged very strongly was the resentment and angerbehind Elaine’s guilt and depression. She had helped to set up asituation in which it was somehow always she who did the givingwhile getting no acknowledgement from anyone else. For example,in the build-up to the present admission, her stepmother hadinvited an extra six relatives for Christmas lunch at Elaine’s house. Since it had always been Elaine’s task to cook the meal, she had feltunable to refuse or ask for extra help. Her Christmas had been anightmare of shopping, cooking and organising. Elaine’s life wasfilled with similar incidents. Her sons expected dinner to be readyas soon as they came in, although sometimes they arrived hourslate and offered no apologies. Her father and stepmother wereoffended if she did not visit them, and yet often they neglected tovisit her when she was in hospital. Even on her weekend leavesfrom hospital she rushed around doing household chores while therest of the family had a lie-in. She described tearfully how it wasalways she who went forward to kiss her children and parents atvisiting time and ask them how they were. ‘Why can’t it be theother way round for once?’ she cried.
The irony was that Elaine’s ‘brave face’ was too effective.
Patients mistook her for a nurse and implied that she didn’tneed to be in hospital, while her sister said openly that shewas just looking for an escape from her responsibilities. Elainefeared that the hospital staff thought the same, though theydenied it to her face. Elaine had set a trap for herself; she feltshe had no right to protest or be dissatisfied. So she struggledon, putting on a façade which others were deceived by, andthen felt angry and hurt about being so badly misunderstood,as well as guilty at not being able to cope. She tried tosuppress these feelings too, and so the vicious circlecontinued.
Elaine and her therapist started looking into her childhood for the
origins of this pattern. The accumulation of hurts, resentments andlosses went back many years. Elaine was nine when her mother died. Shortly afterwards, Elaine’s father remarried and two furtherchildren were born. Elaine and the two boys from the first marriagewere shunned; but although still a child herself, Elaine had to bringup her younger brothers. She was kept back from school to do thehousework and despatched to relatives to help out, while her half-sisters had every attention and comfort. Elaine, known as the ‘strongone’, was expected to cope with all this without acknowledgement,support or affection: and as a young child she had little option but tocomply. It was very painful for Elaine to recall these events from herpast. At one point she cried out in anguish, ‘Why did they do it tome? I needed love too! Why did they have everything and I hadnothing?’ and she wept bitterly. But as the hurts were graduallyreleased, she experienced the sensation of a hard lump in her chestslowly dissolving.
Elaine and her therapist discussed the ways in which she was
continuing her childhood role of serving others, bottling up herfeelings, having to be ‘strong’ and not having anything for herself. Onthe one hand, she seemed to spend her life apologising and fightingfor the right to exist. On the other, a part of her was starting to saymore strongly, as she put it, ‘I’m me, I’m an individual – I’m not justa cook and wife and mother! I’ve got to have some life of my own!’
Slowly, Elaine started to make changes in her life. She resolved
that this time she would not discharge herself from hospital longbefore she was fully recovered, telling the doctors untruthfully thatshe was fine because she felt so guilty at taking up their time andneglecting her home. She allowed herself to let down the brave fronta little, and asked the staff for help and support when she was at herworst. She was firmer with people who questioned her need to be inhospital, whether they were staff, patients or family. Her therapistarranged a different occupational therapy programme that includedsome enjoyable and relaxing activities.
The major changes had to take place within her family. There
were some successes. On weekend leave, instead of cleaning out thekitchen cupboards, she started to go on outings with her husband. She summoned up the courage to tell her brother how much hisactions had hurt her. Although he was not very receptive, she found
an unexpected ally in her sister-in-law. In fact, they discovered thatthey were both fed up with various aspects of Elaine’s parents’behaviour, and decided to visit them less often, even if there werecomplaints and ‘bad atmospheres’.
However, Elaine was still very fragile, and often despaired of the
possibility of changing entrenched patterns of behaviour in her ownhome. Her two daughters, who uncomplainingly took on the role ofcleaning and caring for the men of the family during Elaine’sadmissions, had never given much trouble, but they, like Elaine,found it hard to break the habit of running around after everyoneelse. Her two sons resisted change very fiercely. Elaine asked for herhusband’s support in challenging the long-standing tradition thatthey contributed none of their earnings for food, keep or laundry,and a furious row broke out. For once Elaine held her ground, onlyto be told by her sons that she was ‘hysterical’, ‘crazy’, and needed‘another spell in the loony bin’. Most hurtfully of all, her husbandchanged sides and accused her of stirring up trouble and being toohard on young lads who deserved a bit of fun. Still fragile and unsureof herself, Elaine was driven close to despair by such incidents. Shefelt it was desperately unfair that, while everyone else was allowed toget angry and have their say, she was labelled as ‘crazy’ when shespoke up for once instead of trying to soothe everyone else, and thewhole family ranged themselves against her. Yet she now realisedvery clearly that her only hope of staying out of hospital was to bringabout changes at home. Both options seemed so bleak that shesometimes contemplated running away and leaving the family, butthey were her whole life and she felt she could never do it.
Elaine tried to explain some of this to her husband. He had coped
valiantly with the children during her many admissions and hadrefused to put them into care, and she deeply appreciated how muchhe had had to bear over the years. At the same time the changes inher were beginning to highlight severe diff iculties in theirrelationship. She knew him well enough to sense that he was feelingvery low himself, yet he refused to confide in her, his GP or anyoneelse. Nor would he come up to the hospital for a joint session,saying, ‘The next thing, they’ll put me in there too!’ When they madetime to sit down quietly and talk, he would try to understand whatshe was going through; but in family crises he was as likely to shout ather as to support her. He frequently exploded in violent rages.
Elaine told her therapist, ‘Sometimes I think he should be heretalking to you, instead of me.’
Over the following weeks, Elaine needed a great deal of support,
which she gained both from her therapist and from a small therapygroup of other patients. Slowly, she increased in strength andconfidence. Indeed, she said, ‘If I’d had this sort of help fifteen yearsago, I might not have needed to be on pills all this time.’ But shecouldn’t afford to look back with regrets because she knew thestruggle to bring about changes in her family would continue formany months and need all her courage and determination. After alonger stay than most, she reached the point of being genuinelyready for discharge. She intended this admission to be her last one. Time will tell whether she succeeds.
Elaine’s story is a clear illustration of many of the themes with whichthis book will be concerned. It can be understood and examined onvarious levels. THE PSYCHOTHERAPEUTIC ANGLE
Let us look at Elaine’s episodes of depression from a psychologicalpoint of view. Her psychotherapy gives us a way of understandingher depression as part of her whole person, of all of her past andpresent experiences and relationships, rather than just as an unpleasantrecurring illness.
Clearly, Elaine was severely emotionally (and to some extent
materially) deprived from a very young age. Not only did she missout on the love, care and attention that all children need, she was alsoexpected to provide it for others – her younger brothers and relatives. She was bearing adult responsibilities without getting the emotionalnourishment that she needed for herself. Her parents seem to havejustified this treatment by designating her as the ‘strong one’ who couldcope with anything. Elaine learned to accept this view, whicheffectively stopped her from complaining or questioning the set-up. She too believed that she should be able to cope. In any case, she hadvery little choice in the matter.
Since the capacity to meet other people’s needs depends on having
your own needs met in the first place, someone in Elaine’s position is inconstant danger of becoming emotionally overdrawn, as it were, and
of not having the resources to cope with others’ demands. Moreover,someone like Elaine is particularly likely to get into the situation whereothers are making a lot of demands, since the role of looking afterothers is one they have been trained in from childhood. As Elaine herselfcame to realise through her therapy, she had contributed to setting up arepetition of her childhood circumstances, and still felt she had no rightto protest about it.
Obviously a lifestyle based on such fragile foundations cannot
continue indefinitely. There comes a point where so much more is beinggiven out than taken in that the whole system breaks down. Sometimesthe event that is the ‘last straw’ seems fairly trivial. Since the family,psychiatric staff, and indeed the woman herself have usually subscribedto the myth of her as strong and capable, the sort of person who helpsothers with their problems, they are often at a loss to understand why arelatively minor incident precipitates such a severe reaction. They areunlikely to appreciate that, from a psychological point of view, thebreakdown can be understood as a cry for rest, care and thereplenishment of depleted resources, and as a desperate protest againstan intolerable lifestyle.
The significance of the precipitating event for Elaine’s first breakdown
now becomes clearer. After the birth of her last child, she was fragileand vulnerable. At the same time, she was required to meet the needs ofothers – her baby and her existing family – and to push her own needsinto the background. It was a repetition of her childhood predicament. For many women, made vulnerable by similar backgrounds, childbirthon its own is enough to trigger what is usually described as ‘post-nataldepression’, but often has its roots much further back. For Elaine,however, the problem was compounded by a whole extra set of demandsfrom the relatives who came to stay. There was just too much weighton the wrong side of the fragile balancing act, and Elaine tipped overfrom ‘strong one’ to ‘sick one’.
Real recovery from depression, as opposed to merely managing
and containing it with medication, involved change on a whole-person level. Elaine had to find a way of completing the manyunfinished events from her past that still haunted her. Much of thiswork was done in the therapy sessions, where she was able to releasethe hurt and anger she had been carrying around for so many years. By shouting, weeping and grieving, Elaine was able to work throughand come to an acceptance of her past, and to liberate the energythat had been bound up in keeping all this pain inside. At the sametime, she needed to fill her emptiness with support, understanding
and care from her individual and group sessions. Her feelings hadto be recognised and validated, not labelled and dismissed. Finallyshe could turn to the task of redefining herself and her life.
Elaine’s therapy also showed that her depression had to be understood,
not just as part of a whole person, but as part of a whole system. She wasinvolved in a network of relationships which included her husband,parents, children, brothers and sisters, friends, patients and hospital staff,and many of the interactions between these people were actually helpingto maintain her depression. For most of her fifteen-year career as apsychiatric patient, this system was stable, if uncomfortable: variouspeople continued to hurt and use her; Elaine continued to allow herself tobe hurt and used; and the psychiatrists continued to admit her to hospitalat regular intervals to administer the same treatment as before. Throughher therapy, Elaine was made aware of this pattern and the way in whichshe had, in her own words, ‘made a rod for my own back’. As she startedto change her contribution to the pattern – for example, refusing to doher sons’ laundry – other members of the system found that their roleswere being challenged too. If, in certain instances, she was not willing tobe the servant, they were no longer so clearly the masters. Change wasforced upon them too.
When someone like Elaine starts off this process of change, two things
characteristically occur. First, it becomes less clear who really is the‘patient’. Elaine and her family had long accepted the doctors’ definitionof her as the ‘sick one’ in the family. However, as she began to makesense of her depression and climb out of the passive, suffering ‘sick role’to become more active and assertive, the problems in the rest of the familystarted to come into focus. Her husband, in particular, seemed to be or tobecome quite depressed himself. It began to look as if it had been part ofElaine’s function to ‘carry’ the depression for both partners in therelationship. While she was the ‘sick one’, he could continue the familiarbut limited role of strong, silent head of the family. As she changed anddemanded more understanding and emotional support from him, itbecame apparent that he was completely unable to deal with his own orother people’s feelings other than by blocking them off. Other membersof the family had their difficulties too – the daughters tending to followtheir mother’s lead, and the sons to follow their father. In fact, it could besaid that in some ways Elaine’s depression had served the function ofcamouflaging the problems of the whole family.
The second characteristic occurrence is that there is strong resistance
to change from other members of the system, who find themselvesbeing challenged in very uncomfortable ways. Elaine’s sons didn’t
want to do their own laundry; her husband was scared of acknowledginghis own feelings; her brother was reluctant to admit he had been hurtful. Although they would doubtless all have said they would do anything tocure the ‘illness’ which had brought the whole family such unhappiness,a view of her difficulties which included a critical look at their owncontributions was not so welcome. In fact, their reaction was to try andpush Elaine back into the ‘sick role’ by labelling her new and assertivebehaviour as ‘hysterical’ and ‘crazy’. Thus their own investment inkeeping her sick was revealed.
For Elaine, too, it was tempting to fall back into this familiar role,
to keep quiet and struggle on as before, paying the price of needingfuture hospital admissions. Some people who become psychiatricpatients actually prefer to stay in the sick role, with the compensatingbenefit of avoiding painful conflict. Many others stay in the role thatpsychiatrists and other staff assign to them because they do not getthe help they need to break out of it. Either way, a false solution, akind of unhappy compromise, is reached. No one is especially happybut, on the other hand, everyone can avoid facing certain painfulissues. In such cases, the unresolved problem tends to be passed on, toreappear in future generations. This can be seen in Elaine’s case. Elaine’s daughters had learned to take over her role, stepping in to dothe cooking, shopping and cleaning for the whole family, includingtheir grown-up brothers. Possibly they too had unfulfilled emotionalneeds because of their mother’s depression and absences during theirupbringing. Their compliant behaviour allowed the men of the familyto act selfishly and ignore other people’s rights and feelings. All thechildren were thus set up to repeat the pattern in their own families:the men prepared to exploit, and the women to allow themselves tobe exploited. In this way, the sins of the fathers (and mothers) are visitedupon the sons (and daughters). THE MEDICAL ANGLE
Let us now look at the part played by the hospital and its staff inElaine’s story.
In fifteen years and twenty-two admissions to two different hospitals,
Elaine had come into contact with more than twenty psychiatrists,including three consultants, and a large number of nurses, occupationaltherapists and other staff. Some of the psychiatrists saw her simply as anunfortunate victim of a recurrent illness which caused her to becomedepressed. Most of the others would have agreed, if asked, that childhood
experiences and family relationships play a part in depression; but withlittle or no training in psychotherapy, they did not have the skills to workout how this might apply to Elaine. In this they were no wiser than Elaineherself, who hadn’t realised how her upbringing was still affecting herand blamed herself for everything, and who initially presented a pictureof a happy family where only she was at fault. With a long list of otherpatients to be seen, it was easier for the psychiatrists to fall back onsomething they did know about: medical-style treatment consisting ofdiagnosis, hospitalisation and medication, all of which carried theimplication that Elaine was suffering from some kind of mental illness. In Elaine’s notes, the words ‘depressive neurosis’ or ‘endogenousdepression’ appeared in the space left for diagnosis. Although details ofElaine’s childhood were dutifully recorded by each of the many doctorswho admitted her, no one was able to make sense of it in relation to herbreakdowns; nor were the interactions between Elaine and her extendedfamily investigated or discussed. In other words, Elaine’s depression wastreated, whether deliberately or in default of any alternative, not as partof a whole person and a whole system, but as an isolated phenomenon. Elaine and her family accepted the professional view that frequentadmissions and permanent medication were the best hope of keeping itunder control.
In fifteen years of pill-taking, Elaine had been prescribed the following
She also had ECT (electro-convulsive therapy or electric shocktreatment) during which an electric current is passed through thebrain, simulating an epileptic fit.
Elaine also received treatment on what might be called a behavioural
level, that is, focusing quite simply on the activities, or behaviours, thatshe was unable to carry out. Here the equation seemed to be:
Problem: She says she can’t cope with the household chores. Solution: Make her do the household chores.
Hence she was assigned to cooking and household managementprogrammes in occupational therapy, as well as art, pottery anddiscussion groups.
Clearly, Elaine’s physical treatment was not particularly successful.
Her doctors might have argued that she would have been even worseoff without medication, which at least kept her going for a time, althoughElaine herself said she was nearly always aware of depression lurkingin the background. But there seems to have been general resignation tothe fact that she would need to come into hospital regularly, and to besupported with medication – supervised in fortnightly or monthlyoutpatient appointments – in between. Since 1991 patients have hadthe right, except in some limited circumstances, to read their medicalnotes. However, since no one may quote from them without thepermission of the health authority, some fictional examples based ontypical real-life extracts will serve to illustrate how the ‘medical model’approach works in practice.
In cases such as Elaine’s, the accumulation of notes and letters tends
to follow a predictable sequence. There will be a pile of memos frompsychiatrist to GP monitoring progress and making minor adjustmentsto medication following the fifteen-minute appointment, along thelines of:
Dear Michael, re: Mrs Elaine Jones, I saw this patient of yourstoday in my outpatient clinic. Her depression is improved and sheis doing rather well on Dothiepin 150 mgs nocte. I have suggestedshe reduces the Tranxene to 15 mgs daily. I will see her again in twoweeks’ time.
After some months or years of ringing the changes in this way, with nosubstantial alteration in the patient’s condition, a slight note ofdesperation may creep in, although the remedy is still to prescribe moreof the same treatment rather than to revise the treatment approach itself. One might then see:
Dear Michael, I saw Mrs Elaine Jones who is still complaining ofsevere depression, with associated early morning wakening, lethargy,and loss of appetite. Although I appreciate she has not done verywell on tricyclics, I thought it might be worth starting her on Tofranil,
possibly combined with ECT and/or admission at a later date if hercondition seems to warrant it.
Or there may be a bald statement about recent stresses, without anysuggestion that it might be useful or relevant to discuss the meaningand implications of these with the patient: ‘Her son has recently lefthome to start a college course, and her elderly mother is ill. I will beseeing her again on . . . ’ At this stage, there may be some grasping ofstraws, at the possibility that another physical cause will be found sothat she can be put right, perhaps: ‘She seems to be worse pre-menstrually,and I wonder if it would be worth referring her to Dr Smith for possiblehormonal therapy.’ Even a psychological hypothesis may be put forward,usually to be dismissed: ‘One suspects that her marriage plays somepart in her depression, but I am doubtful about the likelihood of changein that area.’ A male psychiatrist’s identification with the husband whoalso has to deal with this awkward woman may be revealed by suchphrases as: ‘Mr Jones has put up with his wife’s outbursts with remarkablygood humour over the years.’
Finally, a note of persecution creeps in. The patient has obstinately
refused to get better, and someone who started off five years ago as ‘thispleasant lady’ may end up as ‘this difficult woman’ or worse.
If we look at the effect of the medical model approach on Elaine’s
depression, we can see that one result of ignoring the whole-person,whole-system approach is to deny that her feelings and reactions haveany validity. It is not that she has reason to be depressed, or exhausted,or tearful – these are merely ‘symptoms’ of her ‘illness’. This effectivelytraps her in her situation. She does not strive for change, because importantprofessionals who know about these matters have defined her problemin such a way that she is prevented from realising that change is necessary. Her part is to comply obediently with the treatment that they prescribe. Indeed, the underlying message of giving pills to a patient is: ‘Let mediagnose and treat this problem for you. Follow my instructions andyou will be better.’ This may be very appropriate for earache or ’flu,but for someone like Elaine it is not only not helpful, it is actuallyharmful. The final irony is that she even thanks the hospital for theirtreatment, and feels especially grateful to the consultant who dischargedher, protesting, despairing, and unhelped, back to the very situationthat was contributing to her problems in the first place.
As we have seen, the illness model also reinforces the family’s natural
tendency to exempt themselves from playing any part in Elaine’sdepression. Their need to see the entire problem as located in Elaineand her ‘illness’ is legitimised.
To summarise, Elaine’s treatment not only failed to address the wider
issues at stake, but actually ensured that they would not be addressed. It not only failed to help Elaine, it actually perpetuated her difficulties. Indeed, one could go further and say that the medical model approachnot only perpetuates, but actually creates the difficulties it purports tosolve because, as we have seen, Elaine’s children are set up to carry theproblem down the generations.
Elaine’s story is all too common among people having psychiatric
treatment. This is not to say that Elaine would have suffered the samefate everywhere. The standards of psychiatric practice vary, and thereare some excellent wards, community centres and teams which offer avery good service to those in need. Nevertheless, the fact that thecombined efforts of more than twenty psychiatrists and many other staffover fifteen years failed even to start to help Elaine make sense of herdepression indicates that she was not just the victim of an unfortunateoversight. Nor is such treatment found only in the more backwardasylums; most of Elaine’s admissions were to a modern psychiatric unitin a district general hospital. She had in fact received fairly standardpsychiatric care as practised in the majority of hospitals in this country. If this is so, how and why does it happen?
Part of the answer lies in the training that doctors, nurses and other
psychiatric staff receive. Contrary to popular belief, most of theseprofessionals are not primarily trained to understand people and theirproblems. Doctors are mainly trained to diagnose and prescribe, nursesto manage wards, occupational therapists to run activity and discussiongroups, and so on. If they do have additional skills in counselling orpsychotherapy, these will probably have been gained on courses takenvoluntarily after training or picked up on the job.
Another factor is that even the best efforts are compromised by
working within the psychiatric system. Some of Elaine’s nurses spenthours talking with her and some of her doctors would doubtless havelearned to understand her much better had they not been obliged to moveon every six months to fulfil their training requirements, or had theyhad more time and supervision. However, the overall policy towards apatient tends to sabotage whatever more constructive work may becarried out, unofficially, by staff lower down the hierarchy. By the timesomeone gets to be a ‘known depressive’, usually about their second orthird admission, the chances of them getting treatment different frombefore become fairly remote – partly because success would challengethe correctness of the original decisions. As we saw, Elaine’s consultantwas reluctant for her to have psychotherapy, even though his efforts
had not met with notable success. So, while individual members of staffmay be trying their best to understand the patient as a person in a difficultposition, their efforts will be undermined by the overall message thatshe or he is ‘ill’.
Finally, the ‘illness’ model enables the psychiatric staff themselves,
like Elaine’s family, to avoid facing and sharing the enormous amountof pain that Elaine and others like her are carrying around inside them. They can distance themselves from their own hurts, fears and frustrationswhich might otherwise be stirred up. They do not have to confront thedifficult questions that Elaine’s anguish might raise about their ownattitudes, families, beliefs, roles, and the society in which these thingstake place. THE ‘SEX ROLE’ ANGLE
Let us look at Elaine’s depression from yet another perspective, thatof sex role expectations.
Elaine, like most people who are diagnosed as suffering from
depression, is a woman.1 One way of viewing her problems, and thoseof many of her fellow-patients, is that she was caught in thecontradictions of the traditional female role.
Part of Elaine’s dilemma was that she was expected to give without
receiving enough in return, leading to a build-up of need and resentment. Believing that she ought to be able to cope with this, she blamed all herfailures on herself, without questioning the role that had been thrustupon her. This was not just Elaine’s particular misfortune, althoughshe had had an especially rigorous training in it. Despite changing rolesin recent years, women in general, especially older women and thosefrom workingclass backgrounds, are expected to spend their lives givingto others – their husbands, children and extended families. They areoften defined not as individuals, but in relation to others – wife, mother. Even outside the family, the jobs that involve most in terms of giving,and return least in salary and status, are still held mainly by women –nurses, cleaners, primary school teachers, secretaries, childminders. When Elaine cried out, ‘I’m not just a wife and mother, I’m me! I’m anindividual! I’ve got to have some life of my own!’ she was speaking notjust for herself, but for her whole sex. The women who break down andcome into psychiatric hospitals tend to be those who have adopted thetraditional woman’s role most completely.2
Behind every woman trapped in her sex role, there is a man trapped
in his. The partner who presents to the psychiatric hospital is often the
woman, since women in trouble characteristically become unable toact but are overwhelmed by their feelings. Men, on the other hand, whoare generally less in touch with their feelings, but are freer to act in theworld, are more likely to deal with distress by such means as drinking,violence and delinquency, and ultimately to end up in prisons ratherthan psychiatric hospitals. They may also manifest distress in physicalillnesses. While Elaine followed the woman’s pattern, her husband wasprone to violent outbursts. As Elaine progressed, his inability to dealwith his feelings in any other way became very apparent. His maleconditioning did not equip him to deal with years of strain or to meethis wife on an emotional level. He was trapped too.
Again, the hospital served to reinforce rather than to challenge these
complementary roles. As far as Elaine’s husband was concerned, noattempt was made to allow for his feelings over fifteen difficult years,to encourage him to express them or to see his wife’s desperation asanything more than the symptom of an illness. His part in the treatmentwas limited to meeting the doctors from time to time to discuss whatwas going to be done to his wife next.
As for Elaine, the hospital’s message was quite clear. She was
supposed to be able to cope with all her domestic duties withoutprotesting. Indeed, successful treatment was defined in terms of her beingable to return home and uncomplainingly continue the same activities. Obediently following this regime on the advice of experts, Elaine feltshe had no one but herself to blame when she did not get better, and yetmore guilt was added to her despair. In this too she was following thepattern of the rest of her sex, who characteristically blame themselves,their inadequacy, their weakness, their stupidity, their weight and theirappearance, rather than question the obligation to meet these standardsin the first place.
Hospital staff, like Elaine’s family, often resist healthy assertiveness
in a person who is taking steps towards real recovery. Someone whosits miserably but quietly in a corner, taking their medication regularly,is easier to deal with than someone who is prepared to disagree, protestand complain. Staff may show their resistance in the same way as Elaine’sfamily did – by pushing her back into the ‘sick role’. Patients are likelyto acquire labels like ‘aggressive’ and ‘paranoid’ if their behaviourbecomes too challenging.
What might be called the ‘depressed housewife’ syndrome, with
variations, makes up the everyday bread-and-butter work of psychiatry. The unlucky ones will be getting exactly the same treatment as Elaine.
If traditional psychiatry fails these women so badly, as I believe it
does, then it does little better with other categories of patient – people
who have acquired the labels of schizophrenia, obsessional-compulsivedisorder, manic-depression, anorexia, and so on. A recent survey foundthat 40 per cent of psychiatric in-patients had previously been admittedwithin the same year; 13 per cent had had another admission withinthe previous six weeks.3 For a substantial proportion, this will be thestart of a pattern lasting twenty or thirty years. Such a situation wouldbe unacceptable in any other branch of medicine. Yet a psychiatricadmission costs £50,000 per person per year, and overall treatment costsof psychiatric disorders run at an estimated £4.2 billion a year.4 Whyare such enormous sums expended on methods that are not onlyineffective, but damaging? I have indicated some of the reasons whythis state of affairs continues. A fuller answer takes us on to the rest ofthe book. The Rescue Game
There are many misconceptions about people who receive a psychiatricdiagnosis. Surveys show that although people believe that they deservesympathy and the best possible treatment, a significant and apparentlygrowing minority also believe that they are potentially violent anddangerous, and may pose a risk to others in the community.1 Aninternational study found that ‘schizophrenia’ was ranked fourth offorty diseases in terms of stigma, after rabies, alcoholism and drugaddiction.2 This damaging and inaccurate picture is reinforced by themedia, where even quality newspapers frequently run headlines suchas ‘Schizophrenic raped three’ and ‘Schizophrenic killer givenprobation’,3 which would rightly be condemned as racist ifthey containedthe phrase ‘black man’ instead. In fact, black people, and particularlyblack men, may be doubly demonised: articles on homicides bypsychiatric patients are often illustrated by pictures of black men,although four out of five perpetrators of these crimes are white.4 Suchreports are never balanced by less dramatic, but much morerepresentative, announcements such as ‘Psychiatric patient settlespeacefully into the community’.
The Glasgow Media Group analysed media items dealing with mental
health issues and found that the theme of violence to others accounted for66 per cent of all coverage in the sample month. Sympathetic stories, incontrast, made up only 18 per cent of the items. In exploring the impactof these messages, they found that two-thirds of their audience samplebelieved that mental illness was associated with violence, and most gavethe media as the source of this belief. Worryingly, such beliefs sometimesprevailed even when contradicted by personal experience of thosediagnosed as mentally ill. The researchers concluded that ‘the media canplay a significant role . . . in fuelling beliefs which contribute to thestigmatisation of mental illness’.5
Campaigning groups such as the Schizophrenia Media Agency6 have
been formed to counteract this kind of press coverage. But what is the realrisk of being murdered in a ‘frenzied attack’ by a ‘mad axeman’ releasedfrom the local asylum? There were 699 homicides in 1995, of which 32, or4.6 per cent, were carried out by mentally disturbed suspects.7 The risk peryear of being murdered (by anyone) is one in 100,000.8 Given that only avery small percentage of murders are carried out by those with a psychiatricdiagnosis, the risk of being killed by someone with a mental health problemhas been estimated at only one in 2,000,000 (compared, for example, to arisk of one in 25,000 of dying in an accident at home9 ). Nearly all thesehomicides are of family members;10 although horrific for all those involved,this is not consistent with the picture of widespread random attacks on totalstrangers. Contrary to alarmist reports, there is no evidence of an increasein such incidents since the introduction of community care, despite the factthat the rate of homicides in general has risen; in fact there has been a smalldecline.11 While tragic events do occasionally happen, and are rightlyinvestigated so that lessons can be learned from them, there is no justificationfor stigmatising a whole group of people, or for condemning the policy ofcommunity care on these grounds.
Far less attention is paid to two important ways in which a diagnosis
of mental illness clearly does have links with violence. One is the riskof suicide, which has been estimated to be up to sixteen times the rate inthe general population.12 The other is that the very people most oftenseen as perpetrators of violence are in fact more likely to be victims –previously in their lives, they are disproportionately likely to havesuffered physical and sexual abuse.13 And in their present daily lives,nearly half can expect to be publicly harassed, attacked or abused (forexample, having local gangs spit at them and call them ‘nutter’, orfinding dog faeces pushed through their letterboxes) simply because theyhave a diagnosis of mental illness.14
The vast majority of people using psychiatric services, then, are
ordinary men and women who are temporarily overwhelmed by acomplex mixture of emotional and social problems. On making contactwith the psychiatric services, they are given a diagnosis in accordancewith standard medical practice. The main division is into psychotics(people who are out of touch with reality, or in a layperson’s terms ‘mad’)versus neurotics. Under the first heading come diagnoses such asschizophrenia, manic depression and paranoia. Under the secondheading would come agoraphobia, obsessive-compulsive disorder, mostcases of depression and anxiety, and many others. In order to get a clearerpicture of what actually goes on in psychiatry, I propose to look at groups
of patients, not according to their diagnosis, but according to how theyuse the services and how the services characteristically respond:
1. There is a group of people who are asking for help with problems
that are really relationship and family issues. Elaine Jones is anobvious example.
2. There are people who ask for help with problems which, while
still involving those around them, are not primarily to do withcurrent partners or family relationships. An example might besomeone who has been bereaved, or who is a victim of rape orsexual abuse, or who has had an accumulation of stressful lifeevents.
3. There are other people who, usually for lack of alternative options
or more appropriate forms of help, opt for the career of psychiatricpatient as the only escape from painful situations in their lives.
4. There are those who use the hospital or out-patient services mainly
to meet social or economic needs, perhaps because they are lonelyand isolated or have no suitable place to live. Hospitals may alsobe used for what is often called ‘time out’, or respite. For example,an exhausted mother might come in for a break, or a disturbedadolescent might be admitted for a week mainly to relieve hisparents. However, pressure on beds means that such admissionsare far less frequent than they used to be.
5. There is a group of people who are suffering from conditions of
definite physical origin, such as senile dementia, Huntingdon’sChorea and severe head injury.
6. Finally, there are more extreme examples of the first category,
where family relationships are so intense and entangled that oneperson in the system breaks down very severely.
Obviously these divisions are very rough, and many people will cutacross several of them. There are typical diagnoses for some of thecategories – ‘schizophrenia’ is often the choice for the sixth group – butby using these categories rather than medical diagnoses as a guide, Ihope to show what the psychiatric services actually do in response topeople’s overt or covert requests. The people who fall into categories3–6 will be discussed in subsequent chapters. Meanwhile, we shall lookat the first group. PEOPLE WHO ARE ASKING FOR HELP WITH PROBLEMS THAT ARE REALLY RELATIONSHIP OR FAMILY ISSUES
The ‘depressed housewife’ is the classic example of this type. Shemay be middle or working class, and may be treated as an in- or out-patient, producing many variations on the same theme. Let us lookbriefly at another depressed housewife fifteen years after her firstbreakdown. Susan’s story
Susan Smith is 58, a frail, timid, anxious-looking woman. She hasbeen in and out of hospital for many years. Her admissions haveusually been precipitated by complaints from her husband, Bill,that she is not keeping up with the household chores. He makes anout-patient appointment for her and brings her along, complainingforcefully about this and various other ‘symptoms’, such as herirrational fear that he is about to have an affair. She looks nervousand tearful, agrees she is depressed, and is admitted andmedicated.
After many years of this treatment, a discussion in the team
meeting led to a different attempt to help. In accordance with currentpractice, the team had been trying to avoid admission by assigningSusan a community psychiatric nurse to visit her and offer her supportat home. This had not worked. At the most recent out-patientappointment, Bill angrily insisted that his wife needed to be kept inhospital for the rest of her life. However, the nurses commented thatas soon as she arrived on the ward, Susan brightened up, settled inextremely happily, and showed no signs of depression. The clearindication was that the problems lay in the marital situation ratherthan simply in an ‘illness’ suffered by Susan. A member of the teamagreed to see the couple, not, this time, to pass a medical judgementon the wife, but to find out more about the marital relationship.
There were two sessions, both dominated by Bill. This large, well-
built man loudly accused his thin, timorous wife of underfeeding him,of neglecting the housework and of having an irrational fear of hisbeing unfaithful. He talked down to the therapist and demanded toknow what she was going to do to improve the situation. Thetherapist, feeling rather overpowered, tried to point out that changewould have to come from them both, and that Susan might have herpoint of view too. But Susan, who sat in tremulous silence throughout
these outbursts, could not take advantage of this invitation to voice heropinions. She seemed to have been completely cowed by years ofsubmission and the therapist found out that she was fighting Susan’sbattle for her rather than helping her fight it for herself. Meanwhile Billfrustrated all attempts to get him to listen to his wife by interruptingand loudly insisting that he had always tried every possible way tohelp. The therapist was only able to claim the limited success ofblocking his demand that Susan should once again be admitted tohospital. The opportunity to work on the relationship problemsseemed to have passed many years ago.
Here again we see how medicalising a relationship problem heavilyreinforced the unhealthy aspects of the marriage – the husband’s bullyingdominance, which was the counterpart to his wife’s cowering submission. If the problem had been seen in a whole-person, whole-system wayright back when it started, it might have been possible to do someconstructive work with the couple. Alternatively, if the hospital hadrefused to get involved at all, the resulting crisis might have forcedchange to occur. But by taking an unhappy middle line, defusing eachperiodic crisis by admitting Susan without actually taking any steps todeal with the underlying problems, the hospital played a crucial rolein helping to maintain this destructive relationship exactly as it was. Itwas the necessary third player in this unhappy game.
Again, the values of the traditional woman’s role were accepted without
question. The husband’s complaints were accepted at face value, althoughit emerged in the sessions that one reason for Susan’s so-called irrationalfear of his being unfaithful was his continual threat to be exactly that ifshe did not pull herself together. Indeed, the therapist strongly suspectedthat he was already having affairs, and that his demands for his wife’shospitalisation coincided with times when it would be convenient to haveher out of the way. However, by the time a more community-based,psychotherapeutic approach was available, the situation was tooentrenched for change.
Not very long ago, Susan might have become one of the long-stay
patients whose world is bounded by the grounds of a large Victorianasylum, where years of case notes slowly accumulate in the files. In today’sworld, community teams who inherit such cases are likely to be involvedin a long, demoralising struggle with the legacy of the earlier medicalapproach. And because community teams still incorporate many elementsof the medical model – for example, the use of diagnoses and medication– the overriding messages are still likely to be the ‘illness’ ones that are
keeping the situation so stuck. From a nursing point of view, this can beextemely frustrating, as one researcher observed:
In contrast to the ward, where the nurses had collective responsibilityfor dealing with a group of patients within a ward environmentdominated by the ethos of organic psychiatry . . . the communitynurses were heavily committed to the idea of establishing a personalrelationship with their patients and helping to resolve their problemsthrough individual psychological counselling . . . [However], thesocial role of the mental health system in modern society ensuredthat the contradictions and stresses which often led the ward nursesto withdraw from patient contact were recreated within thecommunity setting . . . The community nurses’ failure to perceivethe underlying continuities within the structure of the mental healthsystem could cause them to respond to changes in their work withinitial enthusiasm followed by growing disillusionment.15
THE RESCUE GAME
There are two predominant models or ways of viewing mental distressin psychiatry, one official and one unofficial. The first is the medicalmodel, and second might be called the ‘pull-yourself-together’ approach. They combine very destructively to take away responsibility from theidentified patient, and then to blame them for their helplessness. Wesaw with Elaine and Susan how the medical view initially encouragedthem and their relatives to see them as helpless victims of an illnessunconnected to the rest of their lives, which meant that the psychiatricservices had to step in and take responsibility for them. Logically,when this fails to help, as it inevitably does, the conclusion should beeither that the illness is more severe or complex than had at first appeared,or that something else is going on. In general hospitals, patients do notget blamed for suffering from incurable illnesses or being misdiagnosed. In psychiatric hospitals, however, the suspicion that psychological and/or social problems are involved tends to manifest itself in a gradualswitch from pitying to blaming the patient. The same process canhappen outside the hospital as well, with clients who are seen by thecommunity mental health team. They turn from ‘mad’ to ‘bad’ andcome to acquire one of the many diagnostic labels reserved for peoplewhom the staff do not know how to help: hysterical, attention-seeking,manipulative, immature, inadequate, aggressive, histrionic. At thispoint, the person may be abruptly discharged. They are then in a
much worse state than before: they have been encouraged to hand overcontrol and responsibility to the psychiatric services and to look tothem for a solution, and have then been blamed for the service’s failureto provide one. What they are left with is the original problem plusconfusion, a sense of failure, possible dependence on medication, anda psychiatric label.
The process can be illustrated by a concept from the school of therapy
called Transactional Analysis. Transactional Analysis analyses manyof the interactions between people as games with predictable outcomes,in which set roles are adopted by the participants. One common exampleis the Rescue Game, in which the two players take turns to adopt thethree main roles of Rescuer, Persecutor and Victim (see Figure 2.1 ).
‘Rescuing’ occurs when one person needs help and another person
tries to help them. The Rescuer, however, fundamentally believes thatpeople cannot really be helped, and cannot help themselves either. Thecorresponding position of the Victim (or patient) is: ‘I’m helpless andhopeless – try and help me.’ The Rescuer responds to this challenge bystepping in and taking over the responsibility for the Victim. Rescuingdoes not work and the Rescuer soon begins to feel angry with the Victimfor being so helpless and hopeless and switches to Persecuting orpunishing (‘This manipulative patient . . . ’). Or the Rescuer may endup being Persecuted by the Victim, who gets angry at being treated asless than equal, and may get his or her own back by making awkwarddemands, taking up staff time, and so on. Or, like Elaine, the patientmay Rescue the staff by pretending to be better. (Rescuing was, of course,
Figure 2.1 The drama triangleSource: Adapted from S.B. Karpman, ‘Script drama analysis’, Transactional AnalysisBulletin 7 (26) (1968), 39–43
a lifelong pattern for Elaine.) The theory says that each player willoccupy every position in the game at some time.
What the three positions have in common is that none of them can be
a basis for relating to others as equals. You are either all-powerful orhelpless. Some careers – nursing, medicine, the helping professions ingeneral – are particularly suited to those who wish to play a lifelong gameof Rescue. The medical profession, with its emphasis on power, statusand specialised knowledge, provides an excellent basis for Rescuing ifthat is what a person wants to do.
In her research on stress in mental health nursing, Jocelyn Handy
describes very clearly how nurses can get caught up in the contradictionsof the system and, lacking a wider analysis of the situation, end up blamingthe patients:
The patient . . . was an ex-school teacher in her early thirties who hadbeen diagnosed as manic-depressive and was being treated within anorganic model involving the long-term administration of lithium salts. The patient definitely exhibited quite severe mood swings . . . Whilstthese symptoms may have had an organic basis, the nurse’s commentsindicate that the patient’s behaviour also seemed to be influenced by anumber of social factors which were not being dealt with because herproblem was officially conceptualised in biological terms. In thisinstance, the main precipitant of a severe mood swing seemed to be aserious row with her boyfriend which had involved him threatening toleave her. The patient’s hospitalisation had always reconciled the coupleand provided them with a needed respite in which to re-negotiate theirrelationship. However . . . the long-term effect of this was that thehospital had become involved in their relationship as a third partywhich simultaneously bound the couple together and made theirrelationship more unstable by ensuring that both partners couldrelinquish responsibility for their acts and blame the patient’s illnessfor the problems in their relationship . . . The nurse’s description of thispatient indicates that she experienced some confusion and frustrationabout this case. While she was obviously aware of the effect of thepatient’s personal relationship on her behaviour, she did not seem toconsider the effects of the more general mental health context beyondclaiming that the patient always ‘played the sick role’ to manipulatean admission. This statement then seemed to strike the nurse as tooextreme and she immediately qualified it by affirming in another partof her diary that the patient had ‘genuine mood swings’ which werestabilised through lithium. The nurse’s attempts to explain the patient’s
behaviour thus oscillated rapidly between an individually-orientedpsychological model in which the patient took full responsibility forher actions and a medical model in which the patient had noresponsibility . . . She later commented to me, rather bitterly, that thepatient ‘was never satisfied until she’s proved she’s ill by making yougive her an injection’ . . . The nurse’s descriptions of her interactionswith other patients illustrated the same problems and indicated thatthe paradoxes of the mental health system coloured most of herrelationships with them.16
In psychiatry, the switch from Rescuer to Persecutor, from ‘this patient ismad’ to ‘this patient is bad’ is seen all the time. Some people presentthemselves as Victims at first assessment. Some are pushed into the Victimrole by the process of medicalising their problems and gradually becomemore helpless and dependent on the psychiatric system, which in turngradually becomes more Persecutory as harsher remedies are tried out.
This is not to say that Rescuing is always inappropriate. In emergencies
– after an overdose, perhaps, or in the relatively rare instances wheresomeone’s mental state puts their own or other people’s safety at risk – itmay be necessary for someone else to take total responsibility for a shortwhile. But in the long term any successful attempt to help people to changeneeds to be based on a treatment contract drawn up by both parties asequal and responsible agents. This flies in the face of all the usualassumptions about the capabilities of those who are called mentally ill. There will be further discussion of this issue later (pp. 59–61). Meanwhile,we can illustrate many of the themes we have been discussing by lookingat how the psychiatric system characteristically intervenes in particularsituations. PEOPLE WHO ASK FOR HELP WITH PROBLEMS WHICH, WHILE STILL INVOLVING THOSE AROUND THEM, ARE NOT PRIMARILY TO DO WITH CURRENT RELATIONSHIP OR FAMILY ISSUES
Linda Hart’s moving and compelling account of nine months in apsychiatric hospital, originally written as a diary, won the MINDbook of the year award in 1995.17 I quote extracts from it below.
Linda’s early life was extremely difficult. Her biological father was
married to her mother’s mother, who looked after her while her motherwent out to work. Linda was the youngest of six children and broughtup in poverty. Her father was violent and a heavy drinker, but he didshow Linda special affection, which made her siblings angry and envious.
She received little attention or warmth from anyone else. When she wasthree, Linda found her father dead in the lavatory.
As an adult, married with two sons, Linda became, in her words:
‘some kind of Wonderwoman’, working full-time, running andrenovating a large house, and taking an active part in her localcommunity. Perhaps inevitably, she broke down and was diagnosedas ‘schizophrenic’ although she believed that she was actually sufferingfrom severe depression. After many years of admissions, her marriageended. She was working part-time for Social Services in a mentalhealth project when familiar feelings began to recur:
Gradually, high spirits and extravagant behaviour tipped over theline. I started getting up at 4 a.m. and couldn’t relax during theevenings . . . That Wednesday evening . . . things began to turn. Iwas sitting in the kitchen and smelled the maggots in the rottingflesh in my stomach. I could hear my father’s voice abusing me,saying I was nothing but a heap of shit and I deserved to die.
I didn’t want to go into hospital but Graham [the consultant] saidhe was going to call for an ambulance and if I didn’t go voluntarilythen he would get my G.P. and I would be sectioned [that is, admittedagainst her will] . . . Walking the short distance from my gate to theambulance made me feel very humiliated and I dared not lookaround to see if I was being watched by anyone.
On the ward, Linda battled with overwhelming feelings of despairand anguish. Some of the staff were very caring; others were less so:
Last night was very difficult. I could see holograms on the chairsand floor. I spoke to Peter the nurse who tried to help me in mydistress. I told him I felt very unsafe. It’s as if I have a black stoneinside me which continues to cause me despair and torture and hasnot really shifted an inch.
In her distress, relationships with the staff assumed enormousimportance, and stirred up very powerful feelings:
Yesterday . . . I became extremely distraught. It centred aroundthe way Laura was treating me. She didn’t actually do anythingbut her manner was very distant, curt and abrupt. At lunchtime Ibecame overwhelmed by the feeling that everyone on the ward,staff and patients, thoroughly hated me . . . My father jumped on
the bandwagon and told me everyone hated the sight of me andthey were all fed up because I wasn’t better. I feel very much inneed of love and care but find it difficult to accept because I alsofeel unworthy. I have a degree of charm which people fall for butwhat they don’t know is that I’m full of shit and maggots andputrid flesh. Someone take care of me, I’m very young . . .
Although she needed the ward, many aspects of institutional life werehard to bear:
Here on the ward the room for smoking in is really grotty. It’syellow from nicotine; the chairs all collapse under us; the TVchanges channels by itself and has to be hit on frequent occasions;the carpet and coffee table are dirty and there’s an extractor fanwhich makes a terrible droning noise . . . Things are always runningout, like Flora and marmalade, butter, jam and toilet paper andtea bags and sugar and tissues.
The petty restrictions added to her feeling of powerlessness as apsychiatric patient:
They employ catering staff to stand by the bowls of cereal tomake sure you don’t take two Weetabix . . . I asked [a nurse] if Icould have my medication early so I could go to bed. He tried toargue that I had to wait till ten because it’s better not to do it indribs and drabs. I said it has taken longer for him to argue than itwould have been to hand out the pills. Then I got really angry andsaid it was humiliating for me at the age of 47 years to have to begto go for a walk and to ask if I can go to bed.
She was also on very large doses of medication, which producedsevere side-effects:
If I sit in a car seat or in an armchair my back muscles go into spasmand I arch my back. This is very uncomfortable and means I can’trelax in an easy chair and sitting in a car for long periods is mostuncomfortable. Then my stomach is very distended. It sticks rightout and starts from under my breasts and goes right down so that Ilook eight months pregnant. I’m lactating [another effect of thedrugs], so my breasts are enlarged. I have electrical sensations inmy limbs, which make me jerk and twitch. My nasal passages areblocked so I breathe through my mouth, which gawps and makesme look like an idiot. My head feels fuzzy and I’m distanced frompeople and find sustained conversation a strain. My toes spread
and in sandals this looks weird. I’m constipated, tired and veryunhappy with my lot. [Her consultant decided to increase hermedication yet again.] Afterwards I slumped into a deep depression. I saw Laura and couldn’t make much sense of what she was sayingbecause I was emotionally overladen. I felt a terrible fear about themedication but when I saw her later I realised that the fear was aprojection. I felt unsafe myself and converted that into being afraidof the staff and to thinking they were trying to kill me with drugs.
In deep despair at her inability to escape her father’s voice, Linda madea very serious suicide attempt and was found only just in time. Afterwardsvarious nurses came to see her:
Christine came to special me [that is, to keep her under closeobservation]. She looked hostile. She said I was selfish, had betrayedher and when I cried she said she had no compassion whatsoever forme . . . Chris, the ward manager, kept away for several days andwhen he did come in he looked serious and said he had felt angrywith me. Laura was also serious and said she felt very upset. I waskept in isolation in the room, only using the loo and the shower ensuite. The nurses had each other in their teams, I had nothing. Onlymy nightie. Jack, who had more to lose than anyone, did not accuseme. He was forgiving and kind and gentle . . . I felt beaten, hated,abused . . . I did try to argue that because I was on a Section 3 [that is,detained on hospital against her will], legally I was not responsiblefor my actions. They told me over and over again that I couldn’t gohome and leave the ward because I wasn’t considered responsible;but when it came to the hanging, suddenly I was considered responsible. . . I was taking instructions from my father. I had no resources left inmy battle against him.
Linda was temporarily transferred to a locked ward, supposedly asafer environment for her. Here, there was little attempt to provideanything more than physical security. Linda felt rejected, terrified andpunished:
I started wandering around the ward crying and terribly distressed. The nurse, Bridget, said I had to sit down and talk. I thought tomyself I would never talk to a single soul again. How could I trustanyone? Eventually they made me take extra medication, but thatdidn’t have any effect. Then Margaret came and held my hand. That was what I needed.
Very gradually, over a period of months, Linda started to emerge fromher despair. She started to make sense of some of her experiences:
The emotions I’ve experienced [over some incidents on the ward],which are to do with doing something wrong and not being forgiven,have a deeper origin, I think . . . On reflection, I think it has to dowith rejection, because when you are rejected by significant peopleyou do feel you have done something wrong, or at least, you areunlovable and to blame. I can remember two occasions of significantrejection. One was my father dying and two was when Gordon [herex-husband] told me he was leaving me to set up home with Ann. Ithink the first occasion was very traumatic and I’ve never reallyfaced it. To find my father dead; to never get him back again; thefinality; the panic and fear; to feel responsible for it; to feel guiltyand to blame; and he never forgave me for finding him dead on thetoilet with his dentures falling on the floor . . . I have never mournedhis death, which is why he’s still alive. I need to lay him to rest, butcan I let him go? Isn’t a tormentor better than a void? I wish therewas somebody here to hold my hand.
Linda was eventually discharged and was successful in arguing forcommunity-based help; she would be supported at home, and wouldhave weekly visits from Laura, her nurse from the ward, for counsellingsessions to explore the meaning of her ‘symptoms’ and experiences, andin particular the unresolved relationship with her dead father. Althoughthere is a long way to go, she feels she is finally getting the kind of helpshe needs.
Linda’s story is a further illustration of the themes we have beendiscussing so far. Although it might seem intuitively obvious thatLinda had good reasons for breaking down, the medical approach onwhich her treatment was based saw her distress as an illness, whichturns her experiences of feeling maggots in her stomach, hearing herfather’s voice and so on into symptoms. On this model, discussingthe meaning of these experiences is as irrelevant as analysing thespeech of someone who is delirious. Indeed, the traditional teachinghas been that to do so is actually harmful to the patient; Linda’sconsultant advised her at one point not to look too deeply into herself. The main aim of her treatment, then, is to suppress rather thanunderstand her ‘symptoms’.
The commonest way to try and eliminate symptoms is by prescribing
drugs. In more extreme cases, more extreme steps are taken. On a previousadmission, Linda had been given ECT (electro-convulsive therapy);contrary to popular belief, ECT is still used throughout Britain on about11,000 people a year. The flaw in all these interventions is the assumptionthat removing or relieving the ‘symptom’ is the same as solving theproblem. Since this is not the case, repeated rounds of medication and/or ECT are usually necessary. Moreover, because real healing has nottaken place, people may be unable to break their dependence on whateveris keeping them going – drugs, hospital admissions or ECT – and maybecome increasingly reliant on props that are steadily undermining theirpower to direct and control their own lives.
The Rescue Game is clearly at work in Linda’s account. She was
initially Rescued, or taken into hospital under the threat of compulsoryadmission, a decision that may well have been necessary at the time. However, the staff were very reluctant to allow her to step out of the patient/Victim role and play an equal part in decisions about her care. This, andthe numerous petty restrictions of life on the ward, reinforced her sense offear and powerlessness. Ironically, as Linda herself tried to point out, itwas at her time of greatest need and despair that she was finally seen as‘responsible’ and in fact blameworthy, as the staff Persecuted her for beingdesperate enough to try to kill herself. Such reactions are not unusual;one authority on suicide noted that in the build-up towards such acts:‘ward staff became critical of [the patients’] behaviour, which wasconstrued as provocative, unreasonable, or over-dependent . . . Suchalienation appears to have been malignant, in the sense that it gatheredmomentum inexorably and was associated with a fatal outcome.’18
Cruel and damaging as such responses are, they too have to be seen
in context. In a setting based upon a medical rather than apsychotherapeutic model, little allowance is made for the feelings ofthe staff, who are left to struggle largely unsupported with the sometimesoverwhelming impact of others’ distress. And, as we discussed earlierin the chapter, staff too tend to be caught in the paradoxes of the mentalhealth system: ‘the dynamics of the psychiatric system are not those of“oppressors and oppressed” but of an institution manifestly failing tomeet the human needs of both those it exists to help and those who labourwithin it’.19 Damaging and Persecutory responses are the inevitableresult.
Another inevitable consequence is that in ignoring the meaning of
people’s experiences, and failing to see them as part of a whole personand a whole system, the psychiatric services end up recreating the
conflicts that lie behind their breakdowns. Coldness from the staff, whowere caught up in their own reactions to Linda’s distress, reinforced allher feelings of unworthiness and made her father’s voice more abusive. Banished to a locked ward after her suicide attempt, Linda felt as lonely,rejected and punished as she had as a child. All aspects of someone’sbehaviour on the ward, or of their relationship to a community worker,can give vital clues to their difficulties, and can, if understood correctly,provide a unique opportunity for learning and growth. With insufficienttraining and support in psychotherapeutic approaches, staff all too oftenignore or encourage compliant and passive behaviour, and Persecuteanger or dissent.
What was also overlooked was the meaning that physical treatments
had for Linda. Not only were the side-effects extremely unpleasant,adding considerably to her distress, but the fear of being persuaded orcompelled to take larger and larger doses increased her distrust and fedinto her beliefs about her father. Of course, medication can be veryunpleasant in general medicine – chemotherapy for cancer, for example– and this isn’t necessarily a reason not to prescribe it. Applying thesame model in psychiatry, Linda’s doctors presumably believed thatthe imposition of extremely powerful chemical compounds was justifiedby the urgent need to treat her underlying ‘illness’. However, the analogyis false; Linda was looking for help, not with a physical state, but amental one, and medication at these levels was actually making hermental state worse.
A psychotherapeutic understanding of Linda’s difficulties would
perhaps see the ‘maggots’ in her stomach as a vivid metaphor for herself-hatred, and her father’s voice as expressing her guilt and confusionabout his death. With the help of a counsellor, Linda has built on theseinsights. She believes that his loss, and the circumstances of his death,were simply too much for a three-year-old to bear. She also suspectsthat, abusive as he was, a bad father was better than no father at all inher hostile family, and that at some level she has been unable to let himgo. Although she still hears his voice, she now feels more in control andless of a victim of these terrifying experiences.20
Unfortunately, although community-based teams can often offer
talking treatments alongside other interventions, there tends to be littletime or support for such work in hospital. This has been even more truein recent years, when the closure of beds has meant that only the mostdisturbed are admitted to hospital and there is constant pressure todischarge them as quickly as possible. In the words of a recent report,people who are admitted to psychiatric wards enter a ‘care vacuum’
where, instead of an individualised appproach, they are offered ‘thesame service, facilities and environment, regardless of theircircumstances or needs, with only minor differences in therapeuticinterventions’. In summary, ‘hospital care is a non-therapeuticintervention’ which may actually increase distress in the long term.21Even if psychotherapy is offered, it may actually be necessary to undothe effects of medical treatment before the original problem can betackled; for example, Elaine and her family’s view of her depression,and the way the family relationships were organised around these beliefs.
We can summarise the principles of two major models of
understanding mental distress, the medical and the psychotherapeutic,as follows:
Psychotherapeutic
Staff feelings marginalised/ Staff feelings acknowledged
and supported, as central tothe work.
Of course, in any enlightened medical setting there will be attempts tosupport the staff, form good relationships with the patients and see peoplein their wider context. However, this will be in addition to the realtreatment – the operation, the medication regime and so on – and isperfectly appropriate for most physical illnesses. In a psychotherapeuticsetting, where emotional distress is the focus, the relationships are thetreatment. The healing comes not from medication (although it mayhelp someone to cope), but from other human beings. Linda’s storyillustrates the point. In her greatest distress, she wanted to be offered,not pills, but a hand to hold. She was searching, not for the correctdiagnosis, but for a way to understand her experiences. She is workingtowards healing, not with the aid of drugs – in fact, she is weaning herselfoff them – but with the help of a trusting relationship within which shecan come to terms with her past.
Most contemporary psychiatrists would see themselves as using an
‘eclectic’ approach – that is, they draw from a number of differentmodels, including psychotherapeutic ones, as appropriate to thesituation. However, the above summary, and the stories we have heardso far, make it clear that medical and psychotherapeutic models arefundamentally incompatible. They start from opposing assumptions,give contradictory messages to patients and staff, and have differentaims. It would be more accurate to describe the so-called eclectic modelas unintegrated, in terms of its poorly thought-out philosophy andinconsistent application. An American psychiatrist describes hisobservations during training:
I listened carefully to staff psychiatrists who made discontinuousswitches back and forth between the two dominant paradigms[models] in discussion of a single case, within the same spokenparagraph, and I realised that psychiatry does not have a coherent,unified model or doctrine. In one instance, a psychiatrist wasdiscussing a young man with schizophrenia from a biomedical . . . point of view. Suddenly, he lurched into a discussion of projectionas the underlying mechanism for some of the man’s symptoms;then after a couple of sentences, he as suddenly returned to hisbiomedical mode and vocabulary.22
This kind of confusion can be observed on a daily basis in psychiatry. For example, a young man is referred to the psychiatric team after thedeath of his father, and counselling is recommended to help him throughhis grief. However, as soon as he becomes tearful and low – a necessarypart of coming to terms with his loss, from a psychotherapeutic view –he is prescribed anti-depressants, which suppress his feelings again. Community mental health teams have moved away from the hospitalsite, but since the medical way of thinking still runs in parallel withpsychotherapeutic models, the same kind of muddle still follows. Clientswho have suffered major traumas may be assessed as having a‘depressive illness’ rather than an understandable emotional response,and be offered medication in parallel with counselling. Survivors ofsexual abuse may find that therapy is only offered at the cost of acquiringa psychiatric label.
In my experience, the switch from psychotherapeutic to medical
language has very little to do with the patient and his/her problems. Ittends to occur when mental health professionals, and psychiatrists inparticular, reach the limits of their own ability to see someone’s distressin psychological terms and to bear the feelings that this stirs up. Since
most professionals only have a very basic training in counselling, ifany at all (see Chapter 7), these limits are reached fairly rapidly. Medicaland/or Persecutory interventions are the rule for patients who are moredistressed than the staff can bear, as Linda discovered. As one womanput it, ‘I feel that, essentially, when a doctor prescribes a pill for me, it’sto put him out of my misery.’23
The split in the treatment approaches can come to reflect the split in
the patient: ‘Can I bear to get in touch with my feelings, or shall I tryand push them away?’ Unless this split in the treatment is resolved, thereis no chance of resolving it within the patient. He or she will simplybecome trapped in the mixed messages from the staff, who arethemselves trapped in the mixed messages of the system they work in.
We have now seen numerous examples of the ways in which the main
model of mental distress, on which psychiatry as a branch of medicine isbased, that is the medical/illness model, undermines and opposes thepsychotherapeutic one, often with disastrous results for patients and staff. However, the split is not just between different models of intervention. There is also a fundamental split between the way service users generallysee their problems and the way their difficulties are seen by psychiatrists. When asked what made them break down, service users typically givethis kind of response:
I was depressed and upset following the death of my mother. We hada difficult relationship and I never felt wanted by her. While she wasalive I felt she never loved me. After her death there was no chance toput that right. Also earlier abuse by a family member affected meand the relationship I had with my husband as a result.
Long periods of unemployment. Society in general saying that therewas plenty of work to be had, so those out of work were seen asbeing lazy. Employers told you that you were no good by notemploying you.
The direct issue was the loss of my baby. The indirect one wasproblems with my neighbours and my job.24
If I look back on what caused the depression and what caused me totry and take my life, it was quite normal, average things . . . adivorce, I had two children, I was three months pregnant when I left. . . holding three jobs down, mundane jobs, trying to keep it goingreally. I was worn out, absolutely worn out.25
In other words, despite the adoption of some medical terminology (‘I’mdiagnosed as manic-depressive’, ‘I was very psychotic at the time’26 ),
service users tend to attribute their breakdowns not to illness, but to avariety of psychological and social reasons. The shorthand for this is apsychosocial understanding of mental distress; that is, a model whichsees psychiatric breakdown as resulting from a mixture of psychologicalfactors (mainly past and present relationship difficulties, and sometimesa spiritual crisis of values and beliefs), often accompanied by socialand financial problems.
An eclectic psychiatric view would certainly see such factors as being
relevant too; perhaps they were triggers for an underlying illness in ratherthe same way that stressful life events may lower your immunity tocancer. This is sometimes known as a vulnerability-stress model ofmental illness, and is subscribed to by many psychiatrists. However, asurvey of 516 service users emphasises the difference in viewpoint: ‘Itwas not these factors which led to their problem; these were the problem. . . . Respondents saw their difficulties as meaningful in the context oftheir life experiences in regard to past disappointments, currentdilemmas and future concerns.’27 Their difficulties were complex andindividual, and could not be reduced to simple diagnostic categoriessuch as ‘manic-depression’ or ‘anxiety neurosis’.
As many readers will be aware, dissatisfaction with what the
psychiatric services offer has led to the rise of an increasingly activeand vocal service user movement in recent years. Their protests makesense if there is such a mismatch between how service users andprofessionals view mental distress and the ways it should be dealt with. The above survey put it like this:
Being treated in a medicalised way, as if they had physical illnesses,formed the basis of negative evaluations and complaints on thepart of most users in every aspect of their management. This rangedfrom a dislike of the aloof and cool attitude of psychiatrists duringinterviews whilst in-patients, to the rejection of physical treatmentsas a response to personal distress. In summary, the professionaldiscourse and the lay discourse about personal distress areincompatible . . . In this light it is not surprising that our respondentsfelt misunderstood and aggrieved so often.28
It is consistent with these findings that service users described warm,caring attitudes and being treated with respect as the most appreciatedaspects of their treatment. Counselling or psychotherapy was describedas helpful or very helpful by almost three-quarters of those who hadbeen offered it. On the other hand, a narrow focus on medication anddiagnosis was disliked: ‘They have a set diagnosis which they work to
and treat [you] with ECT and drugs. They do not search out the reasonsfor your illness with you, so the illness just repeats again and again.’29Perhaps we should not be surprised that this survey found psychiatristsrated as the least helpful profession by one in five people, and the mosthelpful by only one in eight.
Other surveys of user views have produced similar results; for example,
women who self-harm report that what they want above all is to be ableto talk to someone who is sympathetic and supportive about theiremotional and practical difficulties. What they are more likely to getfrom the psychiatric services is ‘no help other than a hurried prescriptionfor drugs’ and dismissive or blaming attitudes; 96 per cent of them aredissatisfied with their hospital treatment.30 Of those service users whospoke to the Mental Health Foundation, 401 said their main need whendistressed was for ‘someone to talk to’, to be listened to and respected, tohelp them express and understand their feelings. This did not necessarilymean formal counselling sessions, although again these were rated verypositively by those who had been offered them: ‘Because I feel my mentalillness had its roots in emotional damage . . . examining these things wasmore profitable than merely using drugs to contain it.’ Althoughmedication could also be helpful, people were clear about its limitations:‘A recurring theme is the failure of these treatments to take account of thewhole person.’ As one respondent put it, ‘Medical treatments can beapplied in an impersonal way, as though you are an object that needs re-moulding rather than a person with feelings and human needs.’31 And adetailed investigation into the lives of discharged psychiatric patientsuncovered the same themes in those trying to survive in the community. One person put it particularly clearly:
A doctor treats a patient and he looks at it, he’s patient-orientatedand my contention is that I get mentally ill because of socialproblems . . . Although they tackle me and give me these injectionsand so on, it will continue to happen because of the social problemsinvolved . . . If you like, I am the symptom of something outside, thecause is outside, whereas they would see the cause as me and if theysolved me, solved my problem, then everybody else is all right. And so it’s an eternal conflict!
What participants looked for from psychiatrists was an approachthat took account of their needs and concerns as persons, an approachin which . . . the prescription of anti-psychotic drugs was an adjunct
to a psychosocial understanding of their predicaments rather thana substitute for such understanding . . . And it was here that theirconflicts with the medical profession arose.32
If the above picture is accurate, and there is indeed an irreconcilabledifference between what service users want and what the psychiatricsystem provides, between the psychosocial understandings and needsof those in distress and the medical assumptions and treatments of theprofessionals, then two results can be predicted:
1. recovery within the psychiatric system will be rare;2. those who do recover will do so despite rather than because of
their psychiatric treatment, and mainly with help from non-medicalsettings outside the psychiatric system.
There is evidence for both these predictions.
Anyone who has worked in psychiatry knows how unusual it is for
people to recover completely and be discharged for ever. Onepsychiatrist who asked colleagues in a busy psychiatric unit to identifyrecovered patients for a research project collected only thirteen namesin nine months, and even these people were still suffering fromconsiderable problems.33 Every ward has its complement of regularattenders who may have had up to twenty or thirty admissions over theyears. The staff move on; the patients, on the whole, do not. Some ofthis can be attributed to the ‘poor prognoses’ of the ‘illnesses’ concerned,although there is intriguing evidence that ‘schizophrenia’, for example,has a much better outcome in non-Western, non-medical settings (seeChapter 10). The alarmingly high re-admission rate, as discussed inChapter 1, confirms this depressing picture.
There has been remarkably little official interest in how service users
do explain their recovery, if it occurs (although service users themselveshave written on the subject34 ), but some patterns can be discerned. Thepeople in the Mental Health Foundation survey had found alternative andcomplementary therapies very helpful, as well as a variety of copingstrategies (exercise, keeping busy, having a regular routine, getting supportfrom friends, and so on). Many of them found support from religious andspiritual beliefs. Others described how their lives were turned around by,for example, a stay in a therapeutic community. These are hospitals runentirely along the psychotherapeutic principles already described; a fewof them exist in the NHS, usually under permanent threat of having theirfunds withdrawn:
It was the most helpful psychiatric ward I was ever in. What made itso helpful was the ethos that we were all there to help each other. Wehad to agree to a written contract before we went in. We could leaveat any time. No one took any drugs. The contract said some unusualthings, for example, ‘Free expression and exchange of views is desiredso that we can learn about these reactions between people.’ Also,‘The staff do not have all the answers, and they have their problemstoo. The patient is just as likely as the staff members to find a solutionto one of the problems under discussion’ . . . I was in this residentialplace for over three months, and came home transformed. It was likebeing brought up again. It was a lesson in love from fellow group andstaff members. I carry the things I learned with me still.35
As we have already noted, not everyone wants or needs formalcounselling or psychotherapy, and the woman quoted above, like manyothers in the surveys we have discussed, also found invaluable supportfrom other service users and self-help groups:
A friend’s boyfriend had joined a self-help network . . . A few monthslater I hit a further low-spot of despair and went along to a meeting. I was greeted as an equal . . . No one was an expert; they’d allstarted where I was. Meetings were led in turn, all tasks were subjectto election and time-limited, so all members quickly felt ownershipof the group . . . I cannot describe the difference between a self-helpgroup based on mutual respect, and the mental health system whereone set of people are the healers and get status and money for it, andanother are the ‘mentally ill’, at the bottom of the hierarchy withless than equal citizenship, stigmatised, no power, barely enoughmoney, seldom respected work, and sometimes no housing.36
I have the support of the tranquilliser project . . . and I work forthem and we all help and encourage each other, support each otherand it’s brilliant. And you have to build back your self-esteem, yourself-worth, it doesn’t just happen . . . and I’m doing it now and it’sfantastic.
I had so much inspiration from other people who were further on
[at a support group], and I really just got involved and startedhelping out there and becoming a bit more empowered . . . I justknew that’s what I wanted to do, try and help other people in theway that that helped me.37
The survey of 516 serv.5ice users noted that they tended to speak farmore positively about voluntary sector provision (drop-in centres, clubsand groups and so on) than about the official services, because of theless formal and more equal relationships, the support from others insimilar situations, and the chance to make an active contribution to theservice.
The overall themes are by now very clear. A substantial proportion of
users of the psychiatric services find them not only unhelpful, but actuallydamaging. The good work that does go on is undermined by the basicprinciples on which the service is run, which derive from the medicalmodel of mental distress. Service users on the whole see their difficultiesin terms that are not just different from, but incompatible with, theseassumptions; this can be referred to as a psychosocial understanding ofdistress. Those who recover often do so despite, rather than because of,their psychiatric treatment, and with non-medical help from outside thepsychiatric system.
All of this raises important questions such as: Why does psychiatry
continue to operate in this way, if it is so unhelpful? Is there any evidencein support of these models and approaches? How can the situation bechanged? However, before discussing these issues, we need to look atsome further consequences of traditional psychiatric practice.
5 Women’s and men’s role problems and psychiatry
6 The professionals and their training
8 Physical treatments and the role of the drug industry
Published in the Winter 2012 CURE Childhood Cancer Newsletter Endocrine Problems after Childhood Cancer Treatment Brooke Cherven, RN, MPH, CPON and Lil ian Meacham, MD Survival rates for childhood cancer have grown greatly over the last few decades thanks to many advances in pediatric cancer treatment. Today the majority of children diagnosed with cancer will become long-term survivors. Su
Update on Daubert: What Has It Done to Affect the Right to Jury Trial? Since 1993, when the Supreme Court issued its decision in Daubert v. Merrell Dow Pharmaceuticals, Inc. 1 federal courts have been grappling with how to properly apply the Court’s gatekeeping mandate. Now that many states have adopted Daubert as well, the affect of the Court’s decision has expanded to virtually ev
 Women’s and men’s role problems and psychiatry
The story of a depressed
Women’s and men’s role problems and psychiatry
The story of a depressed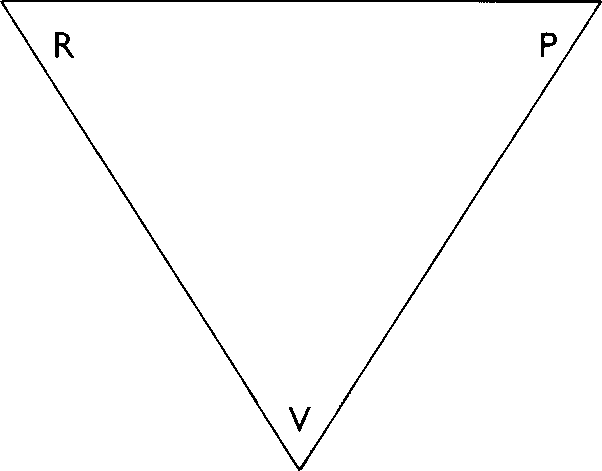 much worse state than before: they have been encouraged to hand overcontrol and responsibility to the psychiatric services and to look tothem for a solution, and have then been blamed for the service’s failureto provide one. What they are left with is the original problem plusconfusion, a sense of failure, possible dependence on medication, anda psychiatric label.
much worse state than before: they have been encouraged to hand overcontrol and responsibility to the psychiatric services and to look tothem for a solution, and have then been blamed for the service’s failureto provide one. What they are left with is the original problem plusconfusion, a sense of failure, possible dependence on medication, anda psychiatric label.