Attenuation of Muscle Metaboreflex in Chronic
BRUNO T. ROSEGUINI1, CRISTIANO N. ALVES1, GASPAR R. CHIAPPA1, RICARDO STEIN1,2, MARLI M. KNORST3,4,and JORGE P. RIBEIRO1,2,4
1Exercise Pathophysiology Research Laboratory, 2Cardiology and 3Pulmonary Divisions, Hospital of Clinics of Porto Alegre,Porto Alegre, BRAZIL; and 4Department of Medicine, Faculty of Medicine, Federal University of Rio Grande Sul, PortoAlegre, BRAZIL
ROSEGUINI, B. T., C. N. ALVES, G. R. CHIAPPA, R. STEIN, M. M. KNORST, and J. P. RIBEIRO. Attenuation of Muscle
Metaboreflex in Chronic Obstructive Pulmonary Disease. Med. Sci. Sports Exerc., Vol. 40, No. 1, pp. 1–6, 2008. Purpose: Abnormal
skeletal muscle function is well documented in chronic obstructive pulmonary disease, but there is no information about the activity of
muscle metabosensitive afferents. In this study, we tested the hypothesis that patients with chronic obstructive pulmonary disease would
have abnormal reflex responses to stimulation of metabosensitive afferents in skeletal muscle when compared with healthy, matched
subjects. Methods: In 16 patients with moderate to severe chronic obstructive pulmonary disease and 13 healthy, age-matched control
subjects, we evaluated heart rate, mean blood pressure, calf blood flow, and calf vascular resistance responses to static handgrip exercise
at 30% of maximal voluntary contraction, followed by recovery with or without circulatory occlusion. Muscle metaboreflex control of
calf vascular resistance was estimated by subtracting the area under the curve with circulatory occlusion from the area under the curve
without circulatory occlusion. Results: Mean blood pressure and heart rate responses were not significantly different in patients and
controls during exercise and recovery. In the control group, calf vascular resistance increased significantly during exercise and remained
elevated above baseline during circulatory occlusion, whereas in patients changes from rest were not significantly different in both
trials. Estimated muscle metaboreflex control of calf vascular resistance was significantly reduced in the patients (controls: 31 T 22units, patients: 8 T 31 units, P G 0.05). Conclusion: Patients with chronic obstructive pulmonary disease have a reduced calf vascularresistance response to handgrip exercise and to selective activation of muscle metaboreflex when compared with healthy subjects. Key
Words: BLOOD FLOW, STATIC EXERCISE, METABORECEPTORS, HEMODYNAMIC CONTROL
Itiswellrecognizedthatcardiovascularadjustmentsto In this technique, interruption of perfusion immediately
static exercise are partially mediated by activation of
before the termination of exercise is thought to trap
mechanosensitive and metabosensitive afferents within
metabolites within the formerly active muscle, thus stim-
the active skeletal muscle. Specifically, stimulation of metab-
ulating chemosensitive fibers (12). Although the specific
osensitive afferents by products of muscle contraction evokes
chemical products that activate these metabosensitive
a powerful increase in sympathetic nervous system activity
afferents remain controversial, considerable evidence sup-
and a consequent pressor response known as the muscle
ports the notion that muscle acidosis is strictly linked to
metaboreflex (27). It is postulated that the primary function
sympathetic vasoconstriction and blood pressure (BP)
of this reflex is to correct a mismatch between blood flow
and metabolism in ischemic exercising muscle (27).
In patients with chronic obstructive pulmonary disease
Static handgrip exercise has been shown to elicit a
(COPD), skeletal muscle dysfunction and its contribution to
decrease in calf muscle vascular conductance (31), and
the pathophysiology of exercise intolerance is a matter of
selective activation of muscle metaboreflex in humans can
extensive investigation (3). Several studies have shown that
be achieved by postexercise circulatory occlusion (PECO+).
patients with COPD have lower percentages of type Imuscle fibers, lower levels of intracellular ATP andphosphocreatine, and reduced activity of oxidative enzymes
Address for correspondence: Jorge P. Ribeiro, M.D., ScD, Associate
(1,16). The latter may occur in the absence of altered
Professor and Chief on Noninvasive Cardiology, Hospital de Clı´nicas de
physical activity patterns, as shown by animal experiments
Porto Alegre, Rua Ramiro Barcelos 2350, 90035-007, Porto Alegre, RS,
(23). During exercise, some studies also have shown that
Brazil; E-mail: jpribeiro@cpovo.net. Submitted for publication July 2007.
these patients develop faster and greater muscular lactic
Accepted for publication August 2007.
acidosis (19,20). At present, however, no evidence existsconcerning the activity of muscle metaboreflex in patients
0195-9131/08/4001-0000/0MEDICINE & SCIENCE IN SPORTS & EXERCISEÒ
with COPD. Accordingly, the purpose of the present study
Copyright Ó 2007 by the American College of Sports Medicine
was to test the hypothesis that patients with COPD have
abnormal reflex responses to stimulation of metabosensitive
Copyright @ 2007 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
afferents in skeletal muscle when compared with healthy-
Muscle metaboreflex. Muscle metaboreflex was
matched subjects. To accomplish this goal, we evaluated
evaluated as described elsewhere (26). In short, after 15
BP, heart rate, and resting limb hemodynamic responses to
min of rest, baseline data for HR, BP, and calf blood flow
static exercise followed by PECO+ in patients with COPD
(CBF) were collected for 3 min. Static handgrip exercise
was then performed with the dominant arm, at an intensityof 30% of maximal voluntary contraction, for 3 min. Duringthe last 15 s of exercise, a pneumatic cuff on the upper arm
was inflated to suprasystolic pressure for 3 min (PECO+).
Subjects. Sixteen patients (11 men) with moderate to
In addition, in a crossover design, subjects performed the
severe COPD (Global Initiative for Chronic Obstructive
same protocol without circulatory occlusion (PECOj).
Lung Disease classes II–IV) (25) participated in the study.
During the protocol, HR was monitored by lead II of the
COPD diagnosis was based on a previous smoking history
electrocardiogram, and BP was measured, using a standard
and pulmonary function testing showing irreversible airflow
auscultatory technique, by the same observer. Mean BP
obstruction (postbronchodilatator FEV1 G 80% and FEV1/
(MBP) was calculated as diastolic + 1/3(systolic j diastolic).
FVC G 70% of predicted). Exclusion criteria were exacer-
CBF was measured by venous occlusion plethysmography
bation or infection in the past 4 wk; severe or unstable
(Hokanson, TL-400, Bellevue, WA) (33). The limb was
cardiac disease revealed by medical history, physical
positioned above heart level and was supported in the thigh
examination, and resting, as well as exercise electrocar-
and ankle to ensure proper venous drainage. A strain gauge
diogram; and locomotor or neurological disease, diabetes
was positioned on the right calf at the point of maximum
mellitus, or uncontrolled hypertension. The control group
circumference. During the entire protocol, a BP cuff on the
consisted of 13 (8 men) healthy, age-matched subjects, who
thigh was alternately inflated to 60 mm Hg and deflated in
also participated in a previously reported study (26). The
7.5-s cycles. Additionally, another cuff was placed on the
research protocol was approved by the institutional ethics
ankle and inflated to suprasystolic levels (240 mm Hg) to
committee, and signed informed consent was obtained from
occlude foot circulation. CBF (mLIminj1I100 mLj1) was
determined manually on the basis of a minimum of four
Protocol. Subjects came to the laboratory for two visits.
separate readings. Reproducibility of CBF measurements in
On day 1, after individuals had spent 20 min of quiet rest in
our laboratory present coefficients of variations of 5.7% and
the supine position, venous blood samples were drawn for
5.9% for short-term (same day) and medium-term (different
plasma norepinephrine determination by high-pressure liquid
chromatography and electrochemical detection. In addi-
Data analysis. Values are reported as means T SD.
tion, arterial blood was drawn from the radial artery for
Subjects_ characteristics and baseline data were compared
blood gas analysis (Rapidlab 865, Chiron Diagnostics, East
by Student_s t-test. Hemodynamic responses to exercise and
Walpole, MA). Later, pulmonary function tests and
to PECO+/PECOj were compared by analysis of variance
symptom-limited cardiopulmonary exercise tests were per-
for repeated measures and Tukey–Kramer_s post hoc for
formed. In the second visit, at least 72 h after the tests,
pairwise comparisons. Correlations were evaluated with the
subjects performed the protocol for the evaluation of mus-
Pearson correlation coefficient. Significance was accepted
cle metaboreflex activity. On both days, patients with
COPD were asked to withdraw from inhaled short-actingA2-agonists and short-acting anticholinergic agents for 8 h,
as well as long-acting A2-agonists and theophylline for 12 h.
Pulmonary function and cardiopulmonary exercise
As shown in Table 1, groups had similar age and body T1
tests. Measurements of forced vital capacity and forced
mass index. Patients had severe ventilatory obstruction and
expiratory volume in 1 s were obtained with a computerized
mild reduction in resting PaO2 and SaO2, but normal PaCO2.
spirometer (Eric Jaeger, GmbH, Wu¨erzburg, Germany), as
As expected, exercise tolerance was markedly reduced in
recommended by the American Thoracic Society (2), and
COPD patients. Baseline MBP, CBF, and calf vascular
AQ1 results were expressed as percent predicted (17). A
resistance (CVR) were similar between the two groups.
symptom-limited incremental exercise test was performed
Maximal voluntary contraction (Table 1) and absolute
on an electrically braked cycle ergometer (ER-900,
handgrip force were not significantly different in COPD
Ergoline, Jaeger, Wu¨erzburg, Germany), with minute
patients and controls. Plasma norepinephrine was signifi-
increments of 5–10 W for COPD patients and 10–15 W
cantly higher in COPD patients (414 T 163 pgImLj1) when
for healthy controls. During the test, gas exchange was
compared with controls (203 T 101 pgImLj1; P G 0.05).
measured breath-by-breath by a previously validated system
MBP, HR, CBF, and CVR responses to handgrip exercise,
(Metalyzer 3B, CPX System, Cortex, Leipzig, Germany)
PECO+/PECOj, and recovery are shown in Figure 1. MBP F1
(22). Heart rate (HR) was determined from a 12-lead
and HR increased significantly during exercise and re-
electrocardiogram. Salbutamol (spray, 400 Kg) was inhaled
mained elevated during circulatory occlusion (PECO+) when
20 min before the tests in patients with COPD.
compared with the control trial (PECOj) (Fig. 1). Changes
Official Journal of the American College of Sports Medicine
Copyright @ 2007 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
increase in CVR during handgrip exercise and postexercise
circulatory occlusion when compared with healthy, matched
controls. Overall, these findings provide the first evidence
for an attenuated contribution of the muscle metaboreflex to
the calf hemodynamic control in COPD.
It is well known that during static handgrip exercise,
there is a time-dependent increase in muscle sympathetic
nerve activity to inactive calf muscles that is tightly coupled
with a reduction in CBF and a pronounced increase in CVR
(29,31). This sympathetic, mediated vasoconstriction acts to
redistribute blood flow toward exercising muscles (27). In
our study, CVR increased, on average, by approximately
38% in healthy controls at the end of exercise, whereas in
patients with COPD it increased by only about 20%, thus
demonstrating a blunted CBF response to exercise in COPD
patients (Fig. 1). Thus, although the mechanisms underlying
this response are unclear, they likely involve a reduced
sympathetic outflow response to exercise and/or a blunted
sympathetic, mediated vasoconstriction in COPD patients.
Available evidence suggests that neurohumoral activation
may play a pivotal role in the pathophysiology of COPD
(4). Recently, direct evidence of marked sympathetic
activation thorough microneurography recordings in
patients with COPD when compared with healthy subjects
COPD, chronic obstructive pulmonary disease; BMI, body mass index; FEV1, forcedexpired volume in 1 s; % pred, percentage of predicted; FVC, forced vital capacity;
was reported (13). In agreement with previous findings
CPET, cardiopulmonary exercise test; V˙O2, oxygen uptake; V˙CO2, carbon dioxide
(34), our COPD patients had higher basal levels of
output; RER, respiratory exchange ratio; V˙E, minute ventilation; SBP, systolic bloodpressure; DBP, diastolic blood pressure; MBP, mean blood pressure; CBF, calf blood
norepinephrine than did healthy controls, compatible with
flow; CVR, calf vascular resistance. * Significantly different (P G 0.05) from control.
tonic activation of the sympathetic nervous system. In thissetting, it is possible to consider that higher sympathetic
from baseline for both variables were similar between
activity at rest would limit the incremental response to
groups during the entire protocol. CBF did not change
exercise because of a ceiling effect, thus resulting in a
significantly from baseline in the two trials in both groups.
decreased calf vasoconstriction, as seen in the COPD
However, patients with COPD exhibited a distinct response
patients. Importantly, however, we did not observe baseline
pattern when compared with control subjects. When compar-
CVR differences between groups, but only a differential
ing both groups, CBF was significantly reduced in healthy
CVR response to exercise in the COPD group.
controls at the end of exercise and during the entire
The origins of sympathetic activation during exercise are
circulatory occlusion period (Fig. 1). CVR increased signifi-
not firmly established, but they likely involve the reflex
cantly during exercise only in the control group (Fig. 1).
responses to stimulation of metabosensitive afferents within
Likewise, during circulatory occlusion (PECO+), CVR
the skeletal muscle (27). To gain insight into the potential
remained elevated above baseline in the control group,
involvement of these chemical-sensitive afferents on the
whereas in the COPD patients changes from rest were not
hemodynamic adjustments to exercise in patients with
significant in either trial. When comparing the estimated
COPD, we performed selective activation of the muscle
difference in the areas under the curves of CVR between
metaboreflex through PECO+ technique. Of note, we also
the two trials during PECO+/PECOj periods, patients with
observed a reduced calf vasoconstriction during PECO+ in
COPD had lower changes (8 T 31 units) compared with
the COPD patients when compared with healthy controls.
healthy subjects (31 T 22 units; P G 0.05). There was a
Thus, by inference, it is reasonable to suggest that this
significant correlation (r = 0.47, P = 0.01) between V
impaired sympathetic activation in COPD patients was at
and the difference in the area under the curve of CVR.
least partially mediated by an attenuated muscle metabore-flex control of CVR.
Interestingly, despite an evident blunted muscle metabor-
eflex control of CVR, COPD patients had only modest
In the present study, we evaluated the cardiovascular
reductions in the pressor response to PECO+ when com-
adjustments to static handgrip exercise and selective
pared with healthy subjects. The reasons for this apparent
activation of the muscle metaboreflex through PECO+ in
discrepancy are unclear, but several hypotheses can be
patients with moderate to severe COPD. The major new
advanced. Sustained BP elevation during PECO+ is thought
finding is that patients with COPD present an attenuated
to be mediated by sympathetic, induced vasoconstriction in
Medicine & Science in Sports & Exercise
Copyright @ 2007 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
FIGURE 1—Mean blood pressure (MBP), heart rate (HR), calf blood flow (CBF), and calf vascular resistance (CVR) changes from baseline duringstatic handgrip exercise, postexercise circulatory occlusion (PECO+), or control (PECOj) periods, and recovery in healthy subjects (left panels) andin patients with COPD (right panels). * P G 0.05 PECO+ vs PECOj.
nonactive vascular beds (12) and enhancement in myocar-
and colleagues (8) have demonstrated that, in contrast to
dial contractility and cardiac filling (30). Thus, first it is
healthy individuals, in which BP elevation during PECO+
relevant to consider that similar BP responses to circulatory
is mediated by increases in cardiac output, patients with
occlusion do not necessarily mean that the mechanisms
heart failure rely mainly on increases in systemic vascular
underlying these responses are the same. In fact, Crisafulli
resistance to achieve similar BP levels.
Official Journal of the American College of Sports Medicine
Copyright @ 2007 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
In our study, patients with COPD had similar BP
hypoxia are not sufficient to alter vascular responsiveness to
responses but attenuated CVR responses to PECO+. One
sympathetic agonists (32). On the basis of these findings, it
possible explanation for these findings is that despite blunted
seems unlikely that eventual reduction in vascular adrener-
vasoconstriction in resting skeletal muscle, these patients
gic reactivity may account for the blunted CRV observed
would exhibit augmented sympathetic, mediated vasocon-
striction in viscera, such as the splanchnic area and the
Sympathetic mediated reduction in resting-limb vascular
kidneys. Prior reports in patients with chronic heart failure
conductance is important for appropriate cardiac output
have demonstrated a similar blunted increase in CVR during
redistribution during exercise. Thus, the correlation between
handgrip exercise (18) associated with exaggerated renal
˙ O2peak and the difference in the area under the curve
vasoconstriction (23). Moreover, although controversial, evi-
of CVR suggest that the blunted muscle metaboreflex–
dence from animal studies suggests that nonuniform changes
mediated vasoconstriction in the resting calf would com-
in sympathetic nerve activity to different regions may exist
promise the distribution of blood flow toward exercising
in certain conditions, such as sustained elevations in BP (6) or
limbs. Conceivably, however, other mechanisms involved
nitric oxide synthase inhibition (15). Together, these findings
in sympathoexcitation during exercise, such as the muscle
reinforce the notion that a shift in the mechanisms under-
mechanoreflex and the respiratory muscle metaboreflex,
lying cardiovascular responses to muscle metaboreflex ac-
might also be altered in COPD patients. For example, as
tivation may also exist in patients with COPD.
indicated by Dempsey et al. (9), augmented respiratory
Another potential mechanism involved in the blunted
muscle work in these patients can potentially exacerbate
CVR responses to exercise and circulatory occlusion in
the respiratory muscle metaboreflex and the consequent
COPD patients is an attenuated vascular responsiveness to
‘‘stealing’’ of blood flow from locomotor muscles. In this
sympathetic stimuli. In general, pathophysiological states
scenario, blunted vasoconstriction in inactive areas would
associated with tonic activation of the sympathetic nervous
also compromise diaphragmatic perfusion, accelerating the
system and release of norepinephrine produce an agonist-
occurrence of diaphragm fatigue during exercise. However,
promoted desensitization of >-adrenergic signaling (29), as
the activity of the respiratory muscle metaboreflex remains
seen in chronic heart failure (11). In addition, the available
to be characterized in this population.
evidence clearly demonstrates that chronic hypoxemia, a
The major limitation of the present study is that we did
common condition in COPD, impairs reflex responses to
not measure muscle sympathetic nerve activity (MSNA) or
sympathetic activation. Heistad and colleagues (14) first
blood catecholamine responses in our subjects during the
demonstrated that patients with chronic severe hypoxemia
protocol. It has been suggested that MSNA responses to
had a depressed forearm vasoconstriction response to lower-
PECO+ provide the major assessment for the muscle
body negative pressure. Likewise, animal studies have
metaboreflex in humans (24). Accordingly, MSNA mea-
shown that chronic, systemic hypoxemia reduces vascular
surement could have helped us to explain the mechanisms
responsiveness to vasoconstrictor substances (9) and to
underlying blunted CVR responses to circulatory occlusion
in patients with COPD. Importantly, however, it is well
Importantly, patients in the present study experienced
known that CVR responses to static handgrip and PECO+
only relatively moderate hypoxia at rest (PaO2 = 71.9 mm
Hg), and all were normocapnic (PaCO2 = 40 mm Hg)—
In conclusion, this study demonstrates that patients with
characteristics that largely differ from those reported in
COPD have a reduced calf CVR response to handgrip
previous studies that have demonstrated a detrimental effect
exercise and to selective activation of muscle metaboreflex,
of hypoxemia on vascular responsiveness to sympathetic
despite a preserved pressor response. Further studies should
stimuli (7,10,13). In contrast to patients with severe
be conducted to address the intrinsic causes of this blunted
hypoxemia, COPD patients with moderate hypoxemia may
muscle metaboreflex control of CVR in COPD and the
develop only episodic reductions in arterial oxygenation
potential impact of this on the pathophysiology of exercise
during the day (5). Thus, it seems reasonable to suggest that
intolerance in this clinical condition.
the functional vascular adaptations may differ whencomparing distinct levels and times of exposure to systemic
We are grateful to Graziella Aliti, RN, MSc, and Eneida R. Rabelo,
RN, ScD, for their careful technical expertise and assistance. This
hypoxia. In this regard, there is evidence derived from
work was supported in part by grants from CAPES and CNPq,
animal studies showing that chronic episodic exposures to
Brasilia, Brazil, and FIPE-HCPA, Porto Alegre, Brazil.
1. Allaire J, Maltais F, Doyon JF, et al. Peripheral muscle endurance
Skeletal muscle dysfunction in chronic obstructive pulmo-
and the oxidative profile of the quadriceps in patients with COPD.
nary disease. Am J Resp Crit Care Med. 1999;159(Suppl):
2. American Thoracic Society. Standardization of Spirometry
4. Andreas S, Anker SD, Scalon PD, Somers VK. Neurohumoral
(Update). Am Rev Resp Dis. 1997;136:1285–98.
activation as a link to systemic manifestations of chronic lung
3. American Thoracic Society/European Respiratory Society.
Medicine & Science in Sports & Exercise
Copyright @ 2007 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
5. Casanova C, Hernandez MC, Sanchez A, et al. Twenty-four hour
with chronic respiratory impairment. Am Rev Resp Dis. 1992;146:
ambulatory oximetry monitoring in COPD patients with moderate
hypoxemia. Respir Care 2006;51:1416–23.
20. Maltais F, Simard A, Simard C, Jobin J, Desgane´s P, Leblanc P.
6. Claassen DE, Morgan DA, Hirai T, Kenney MJ. Nonuniform
Oxidative capacity of the skeletal muscle and lactic acid kinetics
sympathetic nerve responses after sustained elevation in arterial
during exercise in normal subjects and in patients with COPD.
pressure. Am J Physiol. 1996;271:R1264–9.
Am J Resp Crit Care Med. 1996;153:288–93.
7. Coney AM, Bishay M, Marshall JM. Influence of endogenous
21. Mattson JP, Poole DC. Pulmonary emphysema decreases hamster
nitric oxide on sympathetic vasoconstriction in normoxia, acute
skeletal muscle oxidative enzyme capacity. J Appl Physiol. 1998;
and chronic systemic hypoxia in the rat. J Physiol. 2004;555:
22. Meyer T, Georg T, Becker C, Kindermann W. Reliability of gas
8. Crisafulli A, Salis E, Tocco F, et al. Impaired central hemody-
exchange measurement from two different spiroergometry sys-
namic control and exaggerated vasoconstriction during muscle
tems. Int J Sports Med. 2001;22:593–7.
metaboreflex activation in heart failure patients. Am J Physiol
23. Middlekauff HR, Nitzsche EU, Hoh CK, Hamilton MA, Hage A,
Heart Circ Physiol. 2007;292:H2988–96.
Moriguchi JD. Exaggerated renal vasoconstriction during exercise
9. Dempsey JA, Sheel AW, Haverkamp HC, Babcock MA, Harms
in heart failure patients. Circulation 2000;101:784–9.
CA. Pulmonary system limitations in health. Can J Appl Physiol.
24. Negra˜o CE, Rondin MU, Tinucci T, et al. Abnormal neuro-
vascular control during exercise is linked to heart failure severity.
10. Doyle MP, Walker BR. Attenuation of systemic vasoreactivity in
chronically hypoxic rats. Am J Physiol. 1991;260:R1114–22.
25. Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the
11. Feng Q, Sun X, Lu X, Edvinsson L, Hedner T. Decreased
diagnosis, management, and prevention of COPD—2006 update.
responsiveness of vascular postjunctional >1-, >2- adrenoceptors
Am J Respir Crit Care Med. 2007;176:532–55.
and neuropeptide Y1 receptors in rats with heart failure. Acta
26. Roseguini BT, Alvez CN, Chiappa GR, Stein R, Ribeiro JP.
Muscle metaboreflex contribution to resting limb haemodynamic
12. Hansen J, Thomas GD, Jacobsen TN, Victor RG. Muscle
control is preserved in older subjects. Clin Physiol Funct Imaging
metaboreflex triggers parallel sympathetic activation in exercising
and resting human skeletal muscle. Am J Physiol. 1994;266:
27. Rowell LB, O_Leary DS. Reflex control of the circulation during
exercise: chemoreflexes and mechanoreflexes. J Appl Physiol.
13. Heindl S, Lehnert M, Crie´e CP, Hasenfuss G, Andreas S. Marked
sympathetic activation in patients with chronic respiratory failure.
28. Seals DR. Sympathetic neural discharge and vascular resistance
Am J Resp Crit Care Med. 2001;164:597–601.
during exercise in humans. J Appl Physiol. 1989;66:2472–8.
14. Heistad DD, Abboud FM, Mark AL, Schmid PG. Impaired reflex
29. Seals DR, Dinenno FA. Collateral damage: cardiovascular
vasoconstriction in chronically hypoxemic patients. J Clin Invest.
consequences of chronic sympathetic activation with human
aging. Am J Physiol. 2004;287:H1895–905.
15. Hirai T, Musch T, Morgan D, et al. Differential sympathetic nerve
30. Sheriff DD, Augstyniak RA, O_Leary DS. Muscle chemoreflex-
responses to nitric oxide synthase inhibition in anesthetized rats.
induced increases in right atrial pressure. Am J Physiol. 1998;275:
16. Jakobsson PL, Jordfeldt L, Brunden A. Skeketal muscle metab-
31. Sinoway L, Prophet S, Gorman I, et al. Muscle acidosis during
olities and fiber types in patients with advanced chronic
static exercise is associated with calf vasoconstriction. J Appl
obstructive pulmonary disease (COPD), with and without chronic
respiratory failure. Eur Respir J. 1990;3:192–6.
32. Tahawi Z, Orolinova N, Joshua IG, Bader M, Fletcher EC.
17. Knudson RJ, Slatin RC, Lebowitz MD, Burrows B. The maximal
Altered vascular reactivity in arterioles of chronic intermittent
expiratory flow-volume curve. Normal standards, variability, and
hypoxic rats. J Appl Physiol. 2001;90:2007–13.
effects of age. Am Rev Respir Dis. 1976;113:587–600.
33. Thijssen DH, Bleeker MWK, Smits P, Hopman MTE. Reprodu-
18. Kon H, Nakamura M, Arakawa N, Hiramori K. Muscle
cibility of blood flow and pos-reactive hyperemia as measured by
metaboreflex is blunted with reduced vascular resistance response
venous occlusion plethismography. Clin Sci. 2005;108:151–7.
of nonexercised limb in patients with chronic heart failure. J Card
34. Van Helvoort H, Van De Pol M, Heijdra Y, Dekhuijzen PN.
Systemic inflammatory response to exhaustive exercise in patients
19. Kutsuzawa T, Shioya S, Kurita D, Haida M, Ohta Y, Yamabayashi
with chronic obstructive pulmonary disease. Respir Med. 2005;
H. 31P-NMR study of skeletal muscle metabolism in patients
Official Journal of the American College of Sports Medicine
Copyright @ 2007 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
AQ1 0 Some references were not cited alphabetically and have been renumbered; please
check carefully to ensure that all references and citations are correct as edited.
Copyright @ 2007 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Perl version 5.12.2 documentation - perlgpl perlgpl - the GNU General Public License, version 1 SYNOPSIS You can refer to this document in Pod via "L<perlgpl>" Or you can see this document by entering "perldoc perlgpl" DESCRIPTION Perl is free software; you can redistribute it and/or modify it under the terms of either: a) the GNU General Public License as publi
While some medications are considered safe to take during pregnancy, the effects of other medications on your unborn baby are unknown. Therefore, it is very important to pay special attention to the medications you take while you are pregnant, especially during the first trimester, a crucial time of development for you baby. If you were taking prescription medications before you b
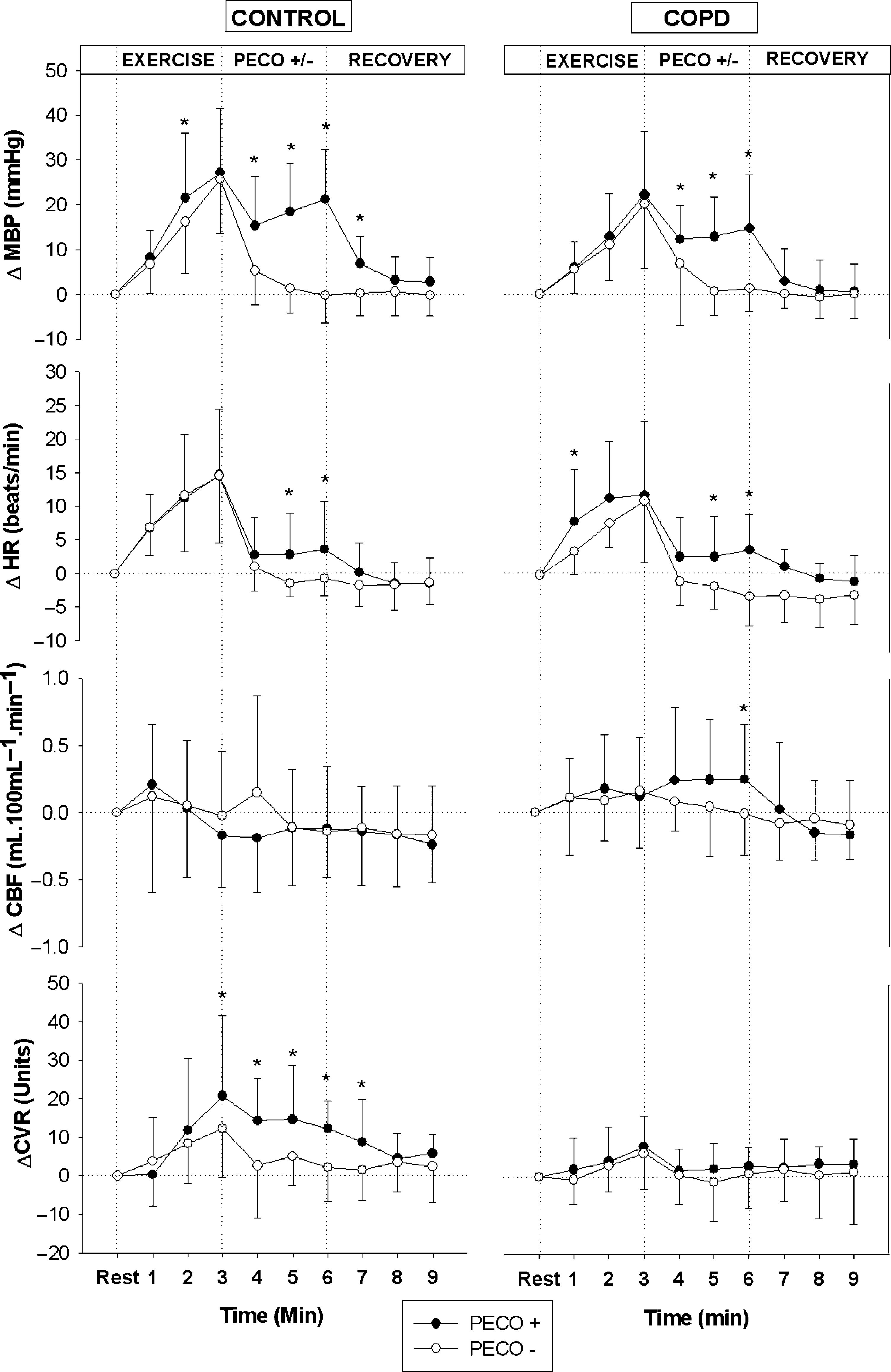 FIGURE 1—Mean blood pressure (MBP), heart rate (HR), calf blood flow (CBF), and calf vascular resistance (CVR) changes from baseline duringstatic handgrip exercise, postexercise circulatory occlusion (PECO+), or control (PECOj) periods, and recovery in healthy subjects (left panels) andin patients with COPD (right panels). * P G 0.05 PECO+ vs PECOj.
FIGURE 1—Mean blood pressure (MBP), heart rate (HR), calf blood flow (CBF), and calf vascular resistance (CVR) changes from baseline duringstatic handgrip exercise, postexercise circulatory occlusion (PECO+), or control (PECOj) periods, and recovery in healthy subjects (left panels) andin patients with COPD (right panels). * P G 0.05 PECO+ vs PECOj.