Biotechnol. Appl. Biochem. (2001) 33, 85–89 (Printed in Great Britain) Erythrocyte-mediated delivery of dexamethasone in patients with chronic obstructive pulmonary disease Luigia Rossi*, Sonja Serafini*, Luigi Cenerini†, Francesco Picardi†, Leonardo Bigi‡, Ivo Panzani‡ and Mauro Magnani*1
*Istituto di Chimica Biologica ‘ G. Fornaini ’, UniversitaZ degli Studi di Urbino, Via Saffi 2, 61029 Urbino (PU), Italy,
†Ospedale ‘Fraternita di S. Maria della Misericordia’, Via Bonconte da Montefeltro, 61029 Urbino (PU), Italy,and ‡Di.De.Co. S.p.A., Via Statale 12 Nord, 41037 Mirandola (MO), ItalyHuman erythrocytes from ten patients with chronic
should be considered if a reversible component in COPD is
obstructive pulmonary disease (COPD) were loaded
present. In fact, oral steroids appear to be beneficial for
with increasing amounts of dexamethasone 21-phos-
acute exacerbations, giving faster impovement in FEV (i.e.,
phate and were re-infused into the original donors.
forced expiratory volume in 1 s) and fewer relapses [6]. Drug-loaded erythrocytes acted as circulating bio-
However, it is important to note that glucocorticoids
reactors, converting the non-diffusible dexamethasone
have a short half-life (approx. 3 h), which make frequent
21-phosphate diffusible dexamethasone.
administrations and high dosages necessary. Consequently,
Pharmacokinetic analyses on these patients showed
this causes a dangerous peak in plasma concentration, toxic
that a single administration of drug-loaded erythrocytes
side effects and poor patient compliance, especially during
was able to maintain detectable dexamethasone con-
the chronic use of the drug. Moreover, when corticosteroids
centrations in blood for up to seven days. This contin-
are administered by inhalation, only a low percentage of the
uous release of dexamethasone was paralleled by the
drug (7 %) is able to reach the lungs, thus compromising the
suspension of β -agonist and oral corticosteroid treat-
therapy. Therefore alternative strategies that are able to
ments by all of the patients.Thus dexamethasone 21-
reduce the toxicity of the drugs, allow prolonged application
phosphate-loaded erythrocytes are safe carriers for
intervals and use different kinds of administration could be of
corticosteroid analogues and are a useful alternative to
clinical importance for the treatment of COPD. frequent oral or inhaled drugs in elderly patients with
It is known that human erythrocytes, owing to the
noteworthy ability of their membrane to be opened andresealed [7], provide an extraordinary vehicle for thedissemination of drugs in the circulation. Moreover,
Introduction
engineered erythrocytes have been proposed as carriers andbioreactors suitable for use in the treatment of various
Chronic obstructive pulmonary disease (COPD) is a major
diseases [8–13]. Previous experiences in our laboratory [14]
cause of morbidity and mortality in adults [1]. It includes
have demonstrated that the non-diffusible pro-drug dexa-
bronchitis (unspecified and chronic), emphysema, asthma
methasone 21-phosphate can be entrapped in human
and acute exacerbations of chronic bronchitis. In COPD,
erythrocytes where it is slowly dephosphorylated to the
inflammation of the airways is a pathogenic factor, inducing
corresponding diffusible dexamethasone by erythrocyte-
chronic sputum production, parenchyma destruction and a
resident enzymes. Furthermore, a new apparatus called ‘ Red
decrease in lung function as a result of airway obstruction.
Cell Loader ’ that allows the encapsulation of drugs in human
Since glucocorticoid hormones are potent anti-inflammatory
erythrocytes for clinical use is now available [15]. Thus, based
drugs [2], they could act as efficient therapeutic agents for
on the above mentioned considerations, we evaluated the
the treatment of COPD. In fact, there are data that support
potential use of autologous erythrocytes with encapsulated
the use of systemic corticosteroids in the treatment of acute
dexamethasone 21-phosphate as a slow delivery system
exacerbations of COPD [3,4], although benefits deriving
from long-term use of corticosteroids to manage chronicCOPD have not been demonstrated. Despite the lack ofevidence for this approach, inhaled corticosteroids are
Key words : corticosteroids ; drug delivery ; erythrocytes.
widely used for the treatment of severe COPD, especially in
Abbreviations used : COPD, chronic obstructive pulmonary disease ; FEV ,
the United States [5]. Moreover, the use of corticosteroids
1 To whom correspondence should be sent (e-mail magnani!bib.uniurb.it). Materials and methods
solution, the addition of dexamethasone 21-phosphate andthe resealing of the lysed cells. This process was performed
Materials
using the ‘ Red Cell Loader ’ apparatus previously described
The blood-processing machine (Di.De.Co Compact A) and
[15], and was completed in 2 h at room temperature under
the red cell loader disposables were obtained from
blood-banking conditions. Briefly, blood (50 ml) was col-
Di.De.Co. S.p.A. (Mirandola, Italy). Dexamethasone 21-
lected from COPD patients in syringes containing heparin as
phosphate and the resealing solution, PIGPA.C (1.606 M
anticoagulant and processed following the sequence of the
KCl, 0.194 M NaCl, 33 mM NaH PO , 0.1 M inosine,
operations described for the ‘ Red Cell Loader ’. To obtain
5 mM adenine, 20 mM ATP, 0.1 M glucose, 0.1 M pyruvate
erythrocytes loaded with different amounts of dexa-
and 4 mM MgCl ), were obtained from Mastelli (Imperia,
methasone 21-phosphate, different amounts of a 40 mM
Italy). Other solutions (washing and hypotonic) were as
dexamethasone 21-phosphate (120 mOsM) solution (5–
20 ml) were added to the lysed cells. At the end of theloading procedure, dexamethasone 21-phosphate-loadederythrocytes were transferred to a final disposable bag and
Patients
re-infused into the original donor. Before this step, the
Ten patients with COPD [PO l 51.28±9.4 mmHg (mean±
volume of the erythrocyte suspension was evaluated and a
S.D.) ; normal value in 70-year-old patients is approx.
100 µl aliquot was used for dexamethasone 21-phosphate
75 mmHg ; FEV l 62.25±8.3 % compared with controls
(mean±S.D.)] were enrolled in this clinical study. They weredivided into three groups : group A (patients 1–5), whoreceived a single administration of autologous erythro-
Determination of the amount of dexamethasone 21-
cytes loaded with different amounts of dexamethasone 21-
phosphate administered to COPD patients
phosphate ; group B (patients 6–8), who received two
The amount of dexamethasone 21-phosphate administered
administrations of dexamethasone 21-phosphate-loaded
to COPD patients was determined by HPLC on boiled
erythrocytes at 15 day intervals ; and group C (patients
samples essentially as described in [15], with some modi-
9 and 10), who received a single administration of loaded
fications. Briefly, 100 µl of the final erythrocyte suspension
erythrocytes and were observed in order to evaluate the
was diluted with 0.9 ml of doubly distilled water, boiled for
pharmacokinetics of dexamethasone. In addition, the phar-
5 min and filtered through 0.22 µm-pore-size filters. HPLC
macokinetics were also evaluated in patient 6 after the first
determinations were performed with a 5 µm Res Elut
dexamethasone 21-phosphate-loaded erythrocyte adminis-
C -90A column (25 cmi4.6 mm internal diameter ; Varian,
tration. All patients received β agonists (theophylline and
Harbor City, CA, U.S.A.) protected by a guard column
bromophylline) and oral or inhaled corticosteroids. Ad-
(Pelliguard LC-18, 20 mmi4.6 mm internal diameter, 40 µm
ministration of these drugs was suspended following
particles). The mobile phase consisted of two eluents : buffer
dexamethasone 21-phosphate administration until they
A containing 10 mM KH PO (pH 5) ; and buffer B, which
consisted of buffer A plus 70 % (v\v) acetonitrile (pH 5). The
The following clinical parameters were evaluated :
elution conditions were : 5 min at 100 % buffer A, increasing
symptoms reported by patients (difficulty in breathing,
to 100 % buffer B over 10 min and held for 8 min. The
cough, quality of life, etc.) ; clinically evaluated symptoms
gradient was returned to 100 % buffer A over 3 min and the
(bronchospasm, bronchostenosis, etc.) ; and frequency of
initial conditions were restored in 5 min. The flow rate was
administration of β agonists and corticosteroids. All patients
0.9 ml\min and detection was performed at 239 nm. Ana-
were monitored for 1 month after the last infusion of
lyses were performed at room temperature and quantitative
drug-loaded erythrocytes. The entire experimental pro-
measurements were obtained by the injection of a standard
cedure was approved by the Ethics Committee of the ‘ S.
of known concentration. The retention times under the
Maria della Misericordia ’ Hospital of Urbino and was
conditions used were 15.2 min for dexamethasone 21-
performed in accordance with the guidelines given in the
phosphate and 17.4 min for dexamethasone. The amount of
Helsinki Declaration with informed written consent.
dexamethasone 21-phosphate (mg) administered was calcu-lated from the concentration of dexamethasone 21-phos-phate encapsulated (µmol\ml of erythrocyte suspension)
Encapsulation of dexamethasone 21-phosphate in
and the volume of the erythrocyte suspension re-infused. erythrocytes Dexamethasone 21-phosphate was selected as a non- diffusible glucocorticoid analogue for encapsulation in Extraction of dexamethasone from plasma samples
erythrocytes of COPD patients. The encapsulation pro-
At different times after the infusion of drug-loaded
cedure involves the lysis of erythrocytes in a hypotonic
erythrocytes (time 0, and 1 and 7 days post-infusion) 10 ml
Erythrocyte-mediated delivery of dexamethasone
of blood was drawn from COPD patients (group C) and collected in heparin. After centrifugation at 2000 g, plasma was separated from blood cells and dexamethasone was extracted using diethyl ether. Briefly, 9 vol. of diethyl ether were added to 1 vol. of plasma and incubated for 1 h at room temperature with gentle mixing. Following centrifugation at 2000 g, the diethyl ether was separated, concentrated with a Speed Vac concentrator (Savant Instruments, Hicksville, NY, U.S.A.) and resuspended in acetonitrile (Sigma–Aldrich, Milan, Italy). The amount of dexamethasone was quantified by HPLC as described above. Recovery was determined by adding a known amount of dexamethasone, and was found to be 64.8±2.5 % (mean±S.D. ; n l 10).
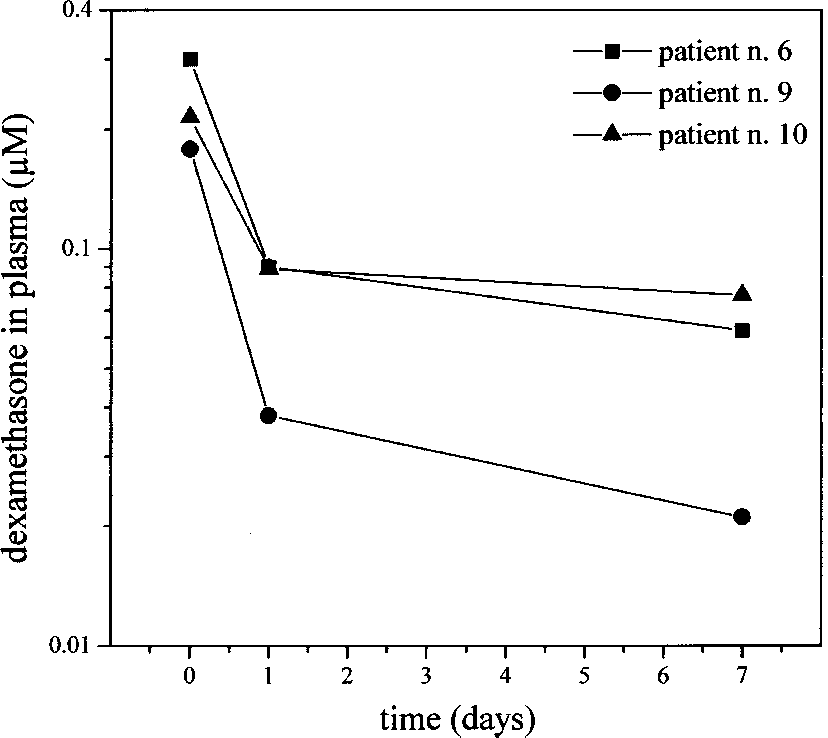
Plasma levels of dexamethasone after administration of dexa-
Dexamethasone 21-phosphate administrations using
methasone 21-phosphate-loaded erythrocytes
the ‘ Red Cell Loader’
Dexamethasone concentrations were determined by HPLC on plasma
Dexamethasone 21-phosphate was encapsulated in auto-
), 9 ($) and 10 (>) at time 0, and 1 and 7 days post-
logous erythrocytes of COPD patients by the procedure
infusion of dexamethasone 21-phosphate-loaded erythrocytes. The amounts of
described in [15] using the specifically designed apparatus
dexamethasone 21-phosphate administered were : 2.00 mg (patient 9) ;2.84 mg (patient 10) ; and 4.39 mg (patient 6, first infusion).
named ‘ Red Cell Loader ’. At the end of the procedure,65±9 ml of erythrocyte suspension at 13±2 haematocrit wasobtained with a cell recovery of 44±6 %. Given the fact thatsome of the erythrocytes are inevitably lost during the
administrations of drug-loaded erythrocytes at 15 day
washing steps and in the dead volume of the circuits, this cell
intervals. These patients received on average 4.90 mg of
recovery can be considered good. The amounts of dexa-
dexamethasone 21-phosphate, a value (in two sequential
methasone 21-phosphate administered to COPD patients
administrations of dexamethasone) close to the highest
are shown in Table 1. The patients enrolled in this study
concentration administered to group A. Patients 9 and 10
were divided into three groups (A, B and C). The first group
(group C) received a single drug administration (2.00 and
(A) received one administration of dexamethasone 21-
2.84 mg of dexamethasone 21-phosphate respectively) and
phosphate with doses ranging from 0.78–8.78 mg. Since no
together with patient 6 (first infusion, 4.39 mg of dexa-
toxic side effects were observed at any of the concentrations
methasone 21-phosphate) were monitored for the deter-
investigated and, moreover, clinical improvements were
mination of dexamethasone in the circulation. The results
obtained, the second group (B) underwent two sequential
obtained (Figure 1), show that dexamethasone was still
Dexamethasone 21-phosphate administered to COPD patients and the number of days passed without taking corticosteroids and β agonists
The amount of dexamethasone 21-phosphate administered to patients was determined by HPLC on boiled samples as described in the Materials and methodssection. admin., administration.
Number of days without β agonists
a This patient did not take any oral corticosteroid or β agonist for the entire period of observation after the first infusion.
present in the circulation 1 week post-infusion of dexa-
chronically treated with steroids for at least 10 years. Thus
methasone 21-phosphate-loaded erythrocytes.
the only possible monitoring was of the reported clinicalsymptoms and medical examinations.
The first group of patients was treated with increasing
Clinical evidence
amounts of dexamethasone 21-phosphate to evaluate the
The patients enrolled in the clinical trial were all suffering
safety and efficacy of the procedure. Since no problems
from severe COPD. All ten patients chronically used short-
developed following erythrocyte infusion and overall clinical
and\or long-acting β agonists and systemic, oral or inhaled
benefits were obtained, a second group of patients received
corticosteroids. Following the administration of dexa-
two infusions of loaded erythrocytes at 2-week intervals. In
methasone 21-phosphate-loaded erythrocytes, all patients
this case, patients reported good health, which was borne
suspended these therapies and were requested to record
out above all by the fact that they never used steroids at least
the time at which they felt the need to take these drugs.
up to 1 month post-erythrocyte infusion. The clinical benefits
Patient 2 resumed inhaled corticosteroids 4 days post-
observed were supported by the results of preliminary
infusion. The other patients did not resume taking the drug
pharmacokinetic studies of a third group of patients, which
for at least 10 days post-infusion. It is worth noting that
revealed the presence of dexamethasone in the circulation
patients 6–8, who received two administrations of drug-
up to 7 days post-infusion. Longer periods of time were not
loaded erythrocytes at 15 day intervals, still did not need
evaluated, but, given the results obtained (see Figure 1), we
corticosteroids 1 month after the last infusion. During the
can assume that low amounts of dexamethasone continue to
same period, all patients were also monitored for the use of
be present in the circulation for a longer time. Furthermore,
β agonists. All patients avoided the use of β agonists for
it is noteworthy that the best clinical benefits were obtained
different periods of time (Table 1) and reported a decrease
by administering, twice in a month, an amount of dexa-
in coughing, breathing difficulties and brochospasms. Fur-
methasone (3.7 mg on the average) that is much lower
thermore, for all patients the physicians reported a reduction
(approx. 25–50 times) than that usually administered in
or absence of bronchostenosis and a reduction of dyspnoea.
therapeutic protocols (4 mg\2–3 times a day per patient). Morover, in all patients (except patient 2) there was areduction in breathing difficulty, bronchospasm, broncho-
Discussion
stenosis and dyspnoea, together with a remarkable reductionin the need to take β -agonists and corticosteroids.
In the present paper we report the first clinical study in
We are confident that this procedure will be useful for
which patients were treated with autologous erythrocytes
the administration of drugs for which a slow and prolonged
modified to act as bioreactors for the slow delivery of
release in the circulation is needed. Further studies of drug
corticosteroids in the circulation. In this study, patients
delivery in vivo in human patients are in progress.
with COPD were treated with autologous erythrocytesloaded with the non-diffusible prodrug dexamethasone 21-phosphate. Once re-infused into patients, dexamethasone21-phosphate is slowly dephosphorylated by erythrocyte-
Acknowledgments
resident enzymes (K l 11.1±0.6 mM ; V l 7.4±0.2 nmol\
h per mg of haemoglobin [14]) to dexamethasone, a
We thank the patients and physicians of the ‘ S. Maria della
corticosteroid able to reduce airway inflammation in
Misericordia ’ Hospital of Urbino (Italy) for their invaluable
collaboration. This work was partially supported by the
Ten patients with COPD were enrolled in our clinical
National Research Council. Target Project on Biotech-
study. After the infusion of autologous dexamethasone
nology. The ‘ Red Cell Loader ’ was provided by Di.De.Co.
21-phosphate-loaded erythrocytes, they were monitored
essentially to evaluate clinical symptoms and the number ofdays that passed without taking their usual drugs (β -agonists
and steroids). In fact, the parameter that most significantly
References
provides evidence for lung function (FEV ) could not be
determined, since all of the patients were unable to perform
Higgins, M. W. and Thorn, T. (1990) in Clinical Epidemiology of
the test correctly due to an advanced age and bad-general-
Chronic Obstructive Pulmonary Disease (Hensley, M. J. and
health status. We also considered other determinations to
Saundres, N. A., eds.), pp. 23–43, Marcel Dekker, New York
monitor possible side effects of corticosteroids, such as
Haynes, R. C. (1990) in The Pharmacological Basis of
assesment of ocular pressure and a computerized study of
Therapeutics (Gilman, A. G., Rall, T. W., Nies, A. S. and Taylor,
bone density, not significant, since all patients had been
P., eds.), pp. 1431–1457, Pergamon Press, New York
Erythrocyte-mediated delivery of dexamethasone
Albert, R. K., Martin, T. R. and Lewis, S. W. (1980) Ann. Intern.
Rossi, L., Bianchi, M. and Magnani, M. (1992) Biotechnol. Appl.
Murata, G. H., Gorby, M. S., Chick, T. W. and Halperin, A. K.
Magnani, M., Fazi, A., Mangani, F., Rossi, L. and Mancini, U.
(1993) Biotechnol. Appl. Biochem. 18, 217–226
American Thoracic Society. Standards for the diagnosis and
Magnani, M., Giovine, M., Fraternale, A., Damonte, G., Rossi, L.,
care of patients with chronic obstructive pulmonary disease
Scarfı', S., Benatti, U. and De Flora, A. (1995) Drug Delivery 2,
(COPD) (1995) Am. J. Resp. Crit. Care Med. 152, S77–S120
Dompeling, E., van Schayck, C. P., van Grunsven, P. M., van
Rossi, L., Brandi, G., Schiavano, G. F., Scarfı', S., Millo, E.,
Ilerwaarden, C. L., Akkermans, R., Molema, J., Folgering, H. and
Damonte, G., Benatti, U., De Flora, A. and Magnani, M. (1999)
van Weel, C. (1993) Ann. Intern. Med. 118, 770–778
AIDS Res. Hum. Retroviruses 15, 345–353
Hoffman, J. F. (1992) in The Use of Resealed Erythrocytes as
D’Ascenzo, M., Antonelli, A., Chiarantini, L., Mancini, U. and
Carriers and Bioreactors (Magnani, M. and De Loach, J. R., eds.),
Magnani, M. (1997) in Erythrocytes as Drug Carriers in
Medicine (Sprandel, U. and Way, J. L., eds.), pp. 81–88,
Ropars, C., Teisseire, B., Avenard, M., Chassaigne, M., Hurel, C.,
Girot, R. and Nicolau, C. (1984) Ann. N.Y. Acad. Sci. 445,
Magnani, M., Rossi, L., D’Ascenzo, M., Panzani, I., Bigi, L. and
Zanella, A. (1998) Biotechnol. Appl. Biochem. 28, 1–6
De Flora, A., Zocchi, E., Guida, L., Polvani, C. and Benatti, U.
(1988) Proc. Natl. Acad. Sci. U.S.A. 85, 3145–3149
Received 15 November 2000 ; accepted 4 December 2000
from Justin Cronin’s The Twelve Bernard Kittridge, known to the world as ‘Last Stand in Denver,’ knew it was time to leave the day the power went out. He wondered what had taken so long. You couldn’t keep a municipal electrical grid running without people to man it, and as far as Kittridge could tell from the 26th floor, not a single soul was left alive in the city of Denver. Which w
Red/Far-Red Light Meter PRODUCT MANUAL Thank you for purchasing a Field ScoutTM Red / Far Red Me- ter. This manual describes its features and operation. Using the Meter 1. Press the ON/OFF button to turn the meter on or off. When first turned on, the display will show the current battery level. 2. Press the READ button to take a light reading. The meter will measure the inciden



 Biotechnol. Appl. Biochem. (2001) 33, 85–89 (Printed in Great Britain)
Biotechnol. Appl. Biochem. (2001) 33, 85–89 (Printed in Great Britain)
 Materials and methods
Materials and methods

 Erythrocyte-mediated delivery of dexamethasone
Erythrocyte-mediated delivery of dexamethasone

 present in the circulation 1 week post-infusion of dexa-
chronically treated with steroids for at least 10 years. Thus
methasone 21-phosphate-loaded erythrocytes.
present in the circulation 1 week post-infusion of dexa-
chronically treated with steroids for at least 10 years. Thus
methasone 21-phosphate-loaded erythrocytes.

 Erythrocyte-mediated delivery of dexamethasone
Erythrocyte-mediated delivery of dexamethasone