Robert V. Kolbusz, M.D. Why are you here today?
(If you are not here for Acne or a Rash, fill out as
many questions as you can from this Questionnaire.)
Please DO NOT MARK ON ANY UNUSED QUESTIONNAIRES
3825 Highland • Suite 5C • Downers Grove, IL 60515 • 630-964-2000 Fax 630-964-2033
Robert V. Kolbusz, M.D. ACNE QUESTIONNAIRE
PATIENT:________________________________ DATE:_____________________
Are you currently treating your acne with over-the-counter products?
________________________ _________________________ _________________________
Have you used any of the following medications?
Dates treated: _____________ _____________ _____________ _____________
WARNING TO FEMALE PATIENTS: Many acne medications CANNOT be used in women during pregnancy and breastfeeding, nor if you are planning pregnancy in the near future. Are you currently: Pregnant
If you are sexually active, do you use birth control? Birth Control Pill
SIGNATURE:___________________________
3825 Highland Avenue • Suite 5C • Downers Grove, IL 60515 • 630-964-2000 Fax 630-964-2033
Robert V. Kolbusz, M.D. RASH QUESTIONNAIRE
PATIENT:________________________________ DATE:____________________ AGE: ________________
DURATION OF RASH: ______YEARS ______MONTHS ______DAYS 1.
IN WHICH LOCATION DID YOUR RASH BEGIN:______________________________________
AND THEN WHERE DID IT SPREAD TO:____________________________________________
ARE YOU CURRENTLY TREATING OR RECEIVED PAST TREATMENT? YES NO
DO YOU OR YOUR FAMILY MEMBER(S) HAVE A HISTORY OF:
CIRCLE M FOR YOURSELF OR LIST FAMILY MEMBER(S)
YES NO ________________________________________________
YES NO ________________________________________________
YES NO ________________________________________________
YES NO ________________________________________________
YES NO ________________________________________________
YES NO ________________________________________________
YES NO ________________________________________________
HOW OFTEN DO YOU BATHE? ___________________________________________________
WHICH BRANDS OF SOAP(S) DO YOU USE? _______________________________________
DO YOU BATHE WITH WARM OR HOT WATER? ____________________________________
DO YOU USE MOISTURIZERS ROUTINELY? YES
WHICH BRANDS? ______________________________________________________________
_____________________________________________________________________________
SIGNATURE: _______________________________
3825 Highland Avenue • Suite 5C • Downers Grove, IL 60515 • 630-964-2000 Fax 630-964-2033
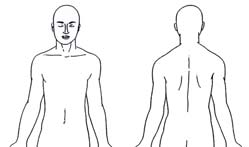
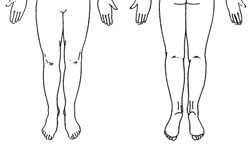
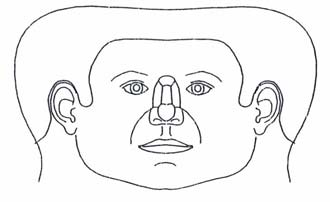
Robert V. Kolbusz, M.D. SKIN LESION QUESTIONNAIRE
PATIENT: _________________________________ DATE: ___________________ PLEASE MARK THE SITE OF YOUR LESION(S).
DURATION OF LESION(S):____________YEARS____________MONTHS____________WEEKS
1. WHAT HAS BROUGHT THE LESION TO YOUR ATTENTION NOW? (CIRCLE)
INTERFERES WITH _____________________ CUTS WITH SHAVING
OTHER_________________________________________
2. HAS THE LESION BEEN PREVIOUSLY TREATED?
YES NO
IF SO, WHEN WAS IT TREATED? DATE: __________________________
3. DO YOU HAVE A FAMILY HISTORY OF SKIN CANCER?: (CHECK ALL THAT APPLY)
IF YES WHICH FAMILY MEMBER? ____________________
SQUAMOUS CELL CARCINOMA DYSPLASTIC NEVUS
4. DO YOU HAVE A PERSONAL HISTORY OF SKIN CANCER? YES NO IF YES, WHICH TYPE?
SQUAMOUS CELL CARCINOMA DYSPLASTIC NEVUS
SIGNATURE: __________________________
3825 Highland Avenue • Suite 5C • Downers Grove, IL 60515 • 630-964-2000 Fax 630-964-2033
Worship in Jerusalem 2006 Conference & Tour RESERVATION APPLICATION Please complete this entire form and return, together with your $500 per person tour deposit to: International Church for All Nations, C/O Apostle Lyrica Smith. Deposits can be paid by check or credit card. Be sure to write your name(s) exactly as on your passport, so that your airline ticket and alldocuments will co
 Robert V. Kolbusz, M.D.
Robert V. Kolbusz, M.D.  Robert V. Kolbusz, M.D.
Robert V. Kolbusz, M.D.  Robert V. Kolbusz, M.D.
Robert V. Kolbusz, M.D. 
 Robert V. Kolbusz, M.D.
Robert V. Kolbusz, M.D.