JOURNAL OF CLINICAL MICROBIOLOGY, Feb. 2001, p. 740–742
0095-1137/01/$04.00ϩ0 DOI: 10.1128/JCM.39.2.740–742.2001
Copyright 2001, American Society for Microbiology. All Rights Reserved.
Maxillary Sinusitis Caused by Actinomucor elegans
GRACIELA DAVEL,1* PATRICIA FEATHERSTON,2 ANIBAL FERNA
CRISTINA CANTEROS,1 LAURA RODERO,1 CARLOS SZTERN,3 AND DIEGO PERROTTA1
Departamento Micologı´a, INEI, ANLIS Dr. Carlos G. Malbra´n, Buenos Aires,1 and Hospital San Juande Dios2 and Fundacio´n Jose´ Marı´a Mainetti, Centro Oncolo´gico,3 La Plata, Argentina
Received 11 August 2000/Returned for modification 19 September 2000/Accepted 16 November 2000
We report the first case of maxillary sinusitis caused by Actinomucor elegans in an 11-year-old patient. Histopathological and mycological examinations of surgical maxillary sinuses samples showed coenocytic hyphae characteristic of mucoraceous fungi. The fungi recovered had stolons and rhizoids, nonapophyseal and globose sporangia, and whorled branched sporangiophores and was identified as A. elegans. After surgical cleaning and chemotherapy with amphotericin B administered intravenously and by irrigation, the patient became asymptomatic and the mycological study results were negative.
An 11-year-old female patient, being neither diabetic nor
paranasal sinuses were inoculated on Sabouraud glucose agar
human immunodeficiency virus positive, without evident un-
with 5% (vol/vol) blood and Sabouraud glucose-honey agar
derlying disease, but with slight leukopenia, was brought to a
supplemented with chloramphenicol and 0.5% (wt/vol) yeast
specialist about left-eye epiphora. On physical examination,
extract and incubated at 28 and 37°C.
the patient reported serosanguinous nasal discharge and de-
In both samples, several cottony, white colonies were evident
creased sinus ventilation lasting 2 months. A magnetic reso-
after 48 h of incubation, and microscopic examination showed
nance imaging (MRI) study revealed left pansinusitis, and non-
that they consisted of coenocytic, branched hyphae of variable
specific treatment was initiated. One month after the first
widths (10 to 25 m), characteristic of mucoraceous fungi.
clinical examination, the patient spontaneously expelled sero-
After 7 days, the same colonies developed globose to subglo-
mucous material during a cough. The presence of coenocytic
bose sporangia. The colonies were more exuberant on Sab-
hyphae in a direct examination of this sample, culturing of
mucoraceous fungi, and opacification of the left maxillary sinus
The fungus was sent to Departamento Mycologia, INEI,
observed by MRI dictated the need for surgical cleaning of the
ANLIS “Dr. Carlos G. Malbra´n,” Buenos Aires, Argentina, for
paranasal sinuses. All the surgical specimens were sent to lab-
identification. Subcultures on potato dextrose agar (PDA), Sa-
oratories for mycological and histopathological studies. Direct
bouraud glucose agar, 2% malt extract agar, Czapek’s solution
microscopy of KOH preparations and tissue sections of the left
agar (Cz), and oatmeal agar were incubated at 25 to 28°C in
maxillary sinus showed broad hyphae, typically coenocytic,
darkness. Subcultures were examined at 4, 7, and 14 days.
characteristic of mucoraceous fungi. No evidence of osseous
Cultures on PDA yielded fast-growing, cottony, almost white
tissue invasion or eosinophils was observed.
colonies. After 4 days, the colonies measured 75 mm in diam-
The results of histopathological and mycological examina-
eter and became olive-buff, with an abundant aerial mycelium
tions of the surgical specimens from ethmoid, sphenoid, and
over 1 cm in height and a colorless reverse. Under a dissecting
frontal sinuses were negative for fungi.
microscope, the colonies showed whorled branched sporangio-
The same fungus was isolated from the seromucous material
phores, originating at a short distance below the terminal spo-
and from the maxillary sinus. The fungus was isolated as a
rangia and bearing secondary sporangia subtended by cross
single microorganism from both samples.
walls (Fig. 1). The sporangiophores arose opposite from the
In addition to the surgical cleaning, the patient was treated
branched rhizoids. Branched stolons were also present. The
with amphotericin B administered intravenously (1 mg/kg of
microscopic examination showed that all of the sporangia were
body weight/day) and by irrigation of the maxillary antrum (5
spherical, 16 to 72 m in diameter, and slightly colored (cream
to buff), had many spores, and were slightly spinous, with
The patient was monitored bimonthly by MRI for 6 months
elongate-oval (4 to 6 by 30 to 34 m) columellae but without
after surgery. Although persistence of the opacity in the left
apophyses. The branched sporangiophores were slightly cream
maxillary sinus was observed, monthly clinical studies to date
to buff, septate, smooth walled, and 4 to 18 m in diameter.
have shown an asymptomatic patient with negative mycological
Stolons and rhizoids were septate, smooth walled, and color-
Mycological findings. The spontaneously expelled seromu-
In old cultures, chlamydospores were present. The sporan-
cous material and a portion of each tissue biopsy from the
giospores were globose and smooth walled and showed high
size variability in different culture media. We randomly mea-
sured the diameters of 52 sporangiospores from a 14-day PDA
* Corresponding author. Mailing address: Departamento Micologı´a,
culture; the values ranged between 4 and 12 m, the arithmetic
Instituto Nacional de Enfermedades Infecciosas, ANLIS Dr. Carlos G.
mean and standard deviation was 7.33 Ϯ 0.16 m, and the
Malbra´n, Av. Velez Sarsfield 563 (1281), Buenos Aires, Argentina.
Phone: 54-11-4302-5066. Fax: 54-11-4302-5066. E-mail: gdavel@anlis
Subcultures on the other culture media, incubated at 25 to
FIG. 1. Slide cultures (4 days old) on PDA at 25 to 28°C in darkness. The specimen was stained with cotton blue. (A) Whorled branched
sporangiophore, originating at a short distance below the terminal sporangium and bearing secondary sporangia subtended by cross walls.
Magnification, ϫ120. (B) Stolons and rhizoids, repeatedly branched. Magnification, ϫ60. Phase-contrast microscopy was used.
28°C in darkness, grew very fast and luxuriantly, as on PDA,
any evident underlying disease. Most of the cases are caused by
except that Cz that did not support good growth. On PDA, the
species of Rhizopus, Absidia, Rhizomucor, and Mucor. Infec-
fungus grew at 37°C but not at 40°C. Based on these morpho-
tions due to other genera of the Mucoraceae are less frequent
logical characteristics, we identified the isolate as Actinomucor
(3, 5). We report the first case of maxillary sinusitis due to
elegans (1, 2). This identification was confirmed by E. Piontelli,
A. elegans in a young female patient without evident underly-
Facultad de Medicina, Universidad de Valparaiso, Valparaiso,
ing disease but with slight leukopenia. To our knowledge, this
Chile, and J. D. David, CABI Bioscience, Egham, United
fungus has never been isolated from a human source.
Kingdom. This isolate has been preserved in IMI and Univer-
Actinomucor, one of several genera of the family Muco-
sidad de Valparaiso herbaria under the designations IMI383277
raceae, was originally described by Schostakowish in 1898
(1). This genus differs from the other mucoraceous fungal
The in vitro susceptibility of the isolate to amphotericin B
genera, except for Rhizomucor, Rhizopus, and Absidia, in hav-
and fluconazole was evaluated by use of the National Commit-
ing branched stolons that give rise to rhizoids and sporangio-
tee for Clinical Laboratory Standards reference method for
phores. Actinomucor is further separated from Rhizopus and
antifungal susceptibility testing of conidium-forming filamen-
Absidia, two other stoloniferous genera, because of differences
tous fungi (4). The MICs obtained were 2 g/ml for ampho-
in the formation of collumellae and sporangiophores and the
tericin B and 1 g/ml for itraconazole.
limited growth of the stolons. Although Actinomucor resem-
Mucoraceous fungi are the most common group of fungi of
bles Rhizomucor, it differs from that genus by having hyaline to
the Zygomycetes and are an ever-expanding group of organisms
faintly colored sporangia and by temperature requirements for
capable of causing human diseases. The main categories of
growth. At present, the genus Actinomucor includes two spe-
infections caused by mucoraceous fungi are sinusitis and rhi-
cies: A. taiwanensis, which is used in the manufacture of sufu,
nocerebral, pulmonary, cutaneous or subcutaneous, gastroin-
a traditional oriental food made from soybean milk, and A.
testinal, and disseminated zygomycoses (3, 5). elegans, the type species of the genus Actinomucor, which is
The incidence of fungal sinusitis, particularly in immuno-
found in soil and other natural substrata from different coun-
competent patients, appears to be increasing. Paranasal sinus
tries but which has never been isolated from a human source
mucormycosis usually has been reported for patients with di-
abetes mellitus but also has been detected in patients without
These two species are very similar, but the major difference
between them is the sporangiospore size; A. elegans has smaller
Fungal sinusitis has been broadly divided into four catego-
sporangiospores (6 to 8 m) than A. taiwanensis (7 to 15 m,
ries: the acute fulminant form, the indolent form, the myce-
even up to 20 m). Although our isolate had some spores
toma form, and the allergic form (3). In this case, as the patient
larger than those described for A. elegans, the mean and the
was immunocompetent, with chronic noninvasive colonization
mode for the spore sizes are included in the spore size range of
of a maxillary sinus by a fungus and without an eosinophilic
this species. Jong and Yuan (2) described other different char-
reaction, this clinical presentation was diagnosed as the indo-
acteristics, such as maximum growth temperatures and the
ability to grow on Cz. According to these authors, A. elegans
Within the expanding group of susceptible hosts, new fungal
shows better growth on Cz than does A. taiwanensis; on the
opportunists are increasing in number; therefore, diagnosis
other hand, the maximum growth temperature for A. taiwan-
and management of the infections that they cause can be dif-
ensis is 37°C, while A. elegans does not grow at this tempera-
ficult and will require a greater understanding of mycological
ture. Under these criteria, our isolate may be identified as A.
details. As an aid to the laboratory identification of this fungus,
taiwanensis because it grows at 37°C and develops less on Cz
the most relevant characteristics are as follows. The genus
than on PDA. However, Benjamin and Hesseltine (1), who
Actinomucor resembles Rhizomucor in having rhizoids, stolons,
have studied a larger number of strains, observed that several
and spherical sporangia with columellae but without apophy-
isolates of A. elegans showed smaller amounts of growth on Cz
ses. Actinomucor has projections of whorls of short branches
than on PDA and that the maximum temperature of growth
below the terminal sporangia of the sporangiophores, which
was approximately 32°C; however, their results were not con-
are absent in Rhizomucor; a lighter pigmentation of sporangio-
clusive. It is evident that more strains are needed to evaluate
spores; and a lack of growth at 40°C.
these characteristics in order to compare these two species.
Based on spore size, which seems to be a major taxonomic
criterion, our isolate was identified as A. elegans. We consid-
We thank E. Piontelli and J. D. David for the confirmation of fungal
ered that this isolate, with intermediate characteristics, could
identification and M. Soria for helpful comments.
be a more mesophilic ecotype of A. elegans with some patho-
genic properties. Molecular data are required to determine if
REFERENCES
these two species represent distinct taxons or could be recog-
1. Benjamin, C. R., and C. W. Hesseltine. 1957. The genus Actinomucor. Myco-
nized at an appropriate infraspecific rank.
logia 49:240–249.
Standardization of in vitro susceptibility testing for filamen-
2. Jong, S. C., and G. F. Yuan. 1985. Actinomucor taiwanensis sp. nov., for
manufacture of fermented soybean food. Mycotaxon 23:261–264.
tous fungi has recently been proposed by the National Com-
3. Lawson, W., and A. Blitzer. 1993. Fungal infections of the nose and paranasal
mittee for Clinical Laboratory Standards (4); therefore, data
sinuses. Part I, p. 1007–1035. In W. Lawson and A. Blitzer (ed.), The otolar-
about the susceptibility or resistance of mucoraceous fungi are
yngologic clinics of North America—1993. W. B. Saunders Co., Philadelphia,
still lacking. In this case, as this was the first clinical isolation of
4. National Committee for Clinical Laboratory Standards. 1998. Reference
the fungus, it was important to determine the MICs of current
method for broth dilution antifungal susceptibility testing of conidium-form-
antifungal drugs. Although we cannot determine the meaning
ing filamentous fungi. Proposed standard. Document M38-P. National Com-
of the amphotericin B and itraconazole MICs found for our
mittee for Clinical Laboratory Standards, Wayne, Pa.
5. Ribes, J. A., C. L. Vanover-Sams, and D. J. Baker. 2000. Zygomycetes in
isolate, future clinical isolations may yield more useful results.
human disease. Clin. Microbiol. Rev. 13:236–301.
Liste der Veröffentlichungen vom 01.01.2006 bis 31.12.2006 Abteilung Pädiatrische Hämatologie/Onkologie Zentrum für Kinderheilkunde Universitätsklinikum Bonn Glasmacher A, Hahn C, Fleischhack G, Marklein G, Walger P. Penicillin-basierte Strategien der Antibiotika-Therapie. Chemother J 2005; 14: 198-206 Schildgen O, Wilkesmann A, Simon A. Wheezing in patients with human metapn
P&G South Africa 2004 HIV/AIDS Report 1 A. Introduction B. Governance Indicator 1. Indicator 2. Overall Strategy for Managing HIV/AIDS Risk Indicator 3. Indicator 4. Indicator 5. Indicator 6. Current and Projected HIV/AIDS Prevalence and Incidence Rates Indicator 7. Current HIV/AIDS-Associated Costs and Losses Indicator 8. Future HIV/AIDS-Associated Costs
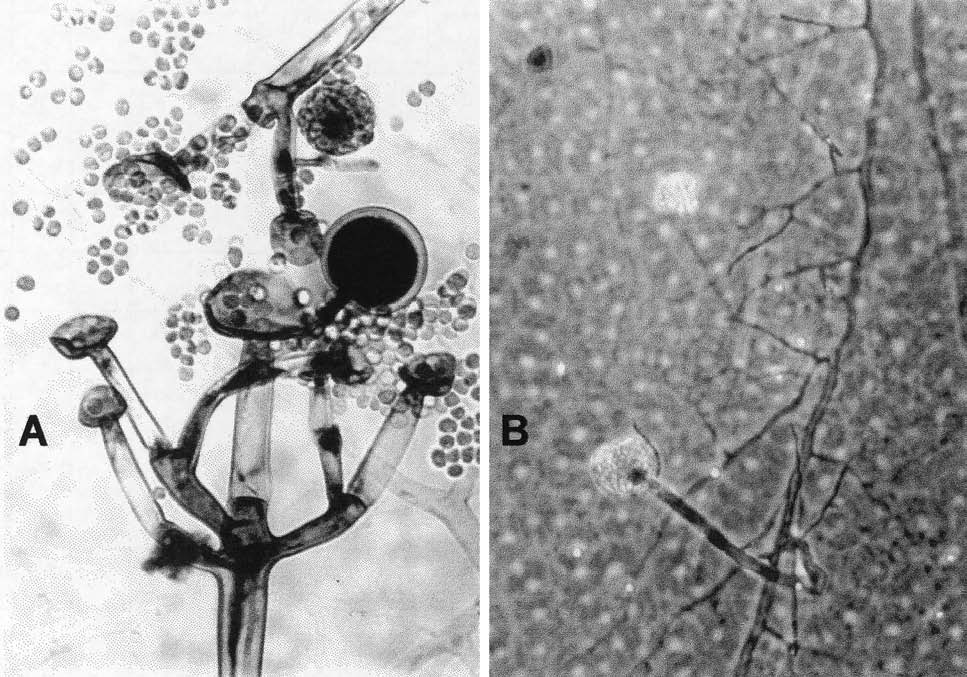 FIG. 1. Slide cultures (4 days old) on PDA at 25 to 28°C in darkness. The specimen was stained with cotton blue. (A) Whorled branched
sporangiophore, originating at a short distance below the terminal sporangium and bearing secondary sporangia subtended by cross walls.
FIG. 1. Slide cultures (4 days old) on PDA at 25 to 28°C in darkness. The specimen was stained with cotton blue. (A) Whorled branched
sporangiophore, originating at a short distance below the terminal sporangium and bearing secondary sporangia subtended by cross walls.