Otolaryngology–Head and Neck Surgery (2006) 134, 558-564
ORIGINAL RESEARCH Palatal implants for the treatment of snoring: Long-term results Ståle Nordgård, MD, PhD, Brit Kari Stene, MD, Ketil Wichman Skjøstad, MD, Vegard Bugten, MD, Kjell Wormdal, MD, Nina Vanvik Hansen, Ann Helen Nilsen, and Tove Helen Midtlyng, Trondheim, Norway
diminished in uvulopalatopharyngoplasty (UPPPand la-
OBJECTIVE:
To evaluate the safety and long-term effective-
ser-assisted uvuloplasty by reducing the pharyn-
ness of a new treatment for snoring using permanent palatal
geal tissue volume and increasing palatal stiffness through
postoperative scarring. However, these procedures are pain-
STUDY DESIGN:
Prospective study with 35 patients referred
ful and may cause considerable morbidity and functional
to the clinic for the treatment of snoring. The patients were fol-
lowed for 1 year, and a sleep analysis was performed and repeatedat 360 days. During the procedure, 3 braided polyethylene tereph-
These concerns have resulted in the development of
thalate implants were placed in the palate of each patient.
targeted procedures that produce less surgical trauma for the
RESULTS:
The average duration for nonnarcotic analgesics
patients. The cautery-assisted palatal stiffening operation
was 1.3 days. No adverse events were observed. The mean snoring
has lower morbidity than UPPP and LAUP but
intensity was reduced from 7.1 at baseline to 4.8 at 1 year (P Ͻ
similar postsurgical pain. Radiofrequency (RF) tissue abla-
0.001). Bed partner satisfaction rate was very high at 70.6% after
tion of the soft creates submucosal scarring to re-
1 year. Six patients (17.8%) experienced a total of 9 partial
duce tissue volume and stiffen overly compliant soft tissue.
However, RF often requires multiple treatment sessions
CONCLUSIONS:
The palatal implant system is safe, and the
with single-use instruments, which increases the cost of
effectiveness in treating snoring is comparable to other surgical
care. Injection sclerotherapy of the palate has been intro-
methods. Advantages are virtually no tissue damage and minimal
duced with favorable results, but the drug is not available in
patient discomfort as a result of one standardized, low-costprocedure.
the United States. As with RF, most patients required more
EBM rating: C-4
than 1 treatment for optimal palatal stiffening, and tissue
2006 American Academy of Otolaryngology–Head and Neck
damage can cause mucosal breakdown and The
Surgery Foundation, Inc. All rights reserved.
newly introduced palatal implant has been designedto achieve palatal stiffening without tissue damage and
Because habitual snoring is so common, finding an ef- volume reduction. The intention of the system is to reduce
fective, minimally invasive, and cost-effective treat-
snoring through placement of permanent implants, causing
ment for those failing conservative therapy has received
fibrosis and submucosal scarring in a single procedure. The
considerable attention over the last several years. Snoring is
implant itself is a segment of braided polyethylene tereph-
From the Department of Otolaryngology–Head and Neck Surgery, St
Presented at the Annual Meeting of the Academy of Otolaryngology–
Olav University Hospital, Trondheim, Norway (Drs Nordgård, Stene,
Head and Neck Surgery, New York, NY, September, 19, 2004.
Skjøstad, Bugten, Wormdal, Nilsen, Midtlyng); Sintef Health Research,
Reprint requests: Ståle Nordgård, MD, PhD, Department of Otolaryn-
Trondheim, Norway (Dr Hansen); and the National University of Science
gology, Head and Neck Surgery, St Olav University Hospital, 7006 Trond-
and Technology, Trondheim, Norway (Drs Nordgård, Stene, Skjøstad).
Costs of performing the study were supported by a grant from Restore
E-mail address: stale.nordgard@medisin.ntnu.no.
0194-5998/$32.00 2006 American Academy of Otolaryngology–Head and Neck Surgery Foundation, Inc. All rights reserved. doi:10.1016/j.otohns.2005.09.033
Palatal implants for the treatment of . . .
ing. The intensity of snoring and the degree of pain, speech,
and swallowing problems were recorded on a visual analog
Selection criteria
scale (VAS) from 0 to 10. For snoring intensity, 0 was no
snoring and 10 related to an intensity that causes the partner
to leave the bedroom. The Epworth Sleepiness Score (ESS)
was used to describe the patient’s daytime sleepiness. To
evaluate the satisfaction rate, the patients and their partners
were asked if they would recommend the procedure to a
friend or a family member based on how they felt at the timeof follow-up.
The ambulatory, nocturnal polysomnography was per-
formed with a thin transnasal esophageal catheter with pres-
thalate (PET). PET has a long history of human implanta-
sure transducers combined with pulse oximetry and an ac-
tion, causing a well-characterized fibrotic response with a
timeter (Reggie system; Camtech AS, Sandvika, Oslo,
fibrous capsule formation typically complete by 4 weeks.
Norway). The airflow in the nose, oro- and hypopharynx
Advantages are expected to be low morbidity, simplicity,
was calculated from the differential pressures in these loca-
and low cost. The objective of this study was to evaluate the
tions. Apneas were defined as an airflow of less than 10% of
safety and efficacy through long-term follow-up.
baseline and hypopnea as a greater than 50% reduction inairflow, both needed a duration of 10 seconds and a 3% dropin SaO . The combined apnea-hypopnea index (AHI) was
PATIENTS AND METHODS
registered and the events registered as obstructive, central,or mixed. This system also allows for an analysis of the
Patient Evaluation
distribution level of obstructions in the airway (transpalatal
Thirty-five consecutive patients referred to St Olav Univer-
sity Hospital, Trondheim, Norway, for habitual snoring and
Follow-up office visits were performed at 2 to 3 days, 14
those who met the selection criteria listed inwere
days, 30 days, 90 days, 180 days, and 360 days after treat-
included in this prospective, nonrandomized study. The
ment. These follow-ups consisted of a physical examination
study protocol was reviewed and approved by the Regional
and the completion of questionnaires to evaluate the safety
Research and Ethical Committee, and informed consent was
and efficacy for the procedure. A polysomnography was
A complete medical history and physical ear, nose, and
throat examination was conducted. To evaluate the physical
The Palatal Implant Procedure
dimensions of the upper airway, the following parameters
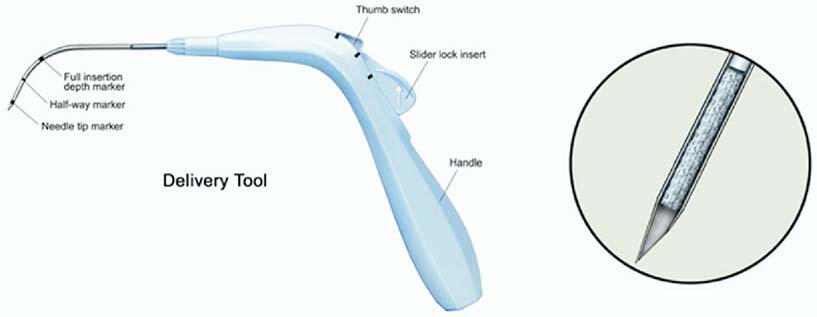
The Palatal Implant System (Pillar System, Restore Medi-
were recorded: the modified Mallampati index (MMP)
cal, St Paul, MN) consists of a delivery system and an
grade I to IV and tonsil size grade 0 to IV according to
implant The delivery system is comprised of a
and the tongue base volume related to the val-
handle and a needle assembly for positioning and placement
lecula grade I-IV (grade I open vallecula, grade II vallecula
of the implant within the soft palate. A thumb slider on the
filled, grade III and IV epiglottis pushed posteriorly or
handle is pulled down to retract the needle tip once the
against the posterior pharyngeal wall) on transnasal fibre-
appropriate depth is reached, while an obturator housed
optic laryngoscopy or related to the visibility of larynx on
within the needle maintains the position of the implant,
indirect laryngoscopy (I: anterior comissure visible, II: pos-
leaving it in place when the delivery device is withdrawn
terior comissure visible, or III: not visible). The patient and
from the tissue. The implant is 18 mm long and 1.5 mm in
the bed partner completed questionnaires to evaluate the
diameter. The implant is designed to be permanent while the
severity, intensity, duration, and social effects of the snor-
The palatal implant system with the delivery handpiece and the implant.
Otolaryngology–Head and Neck Surgery, Vol 134, No 4, April 2006
The implantation procedure. Three implants are placed parallel to the midline in the muscular layer of the palate.
The operative procedure has been described earlier in
the muscular layer toward the base of the uvula until the
In brief, the patients were given paracetamol 400
insertion depth marker reached the insertion point. The implant
mg/codeine 40 mg and diclofenac 50 mg orally. Local anes-
was deployed while retracting the cannula, and the proce-
thesia was obtained by topical lidocaine spray and infiltration
dure was repeated twice more in order to place 2 more
of the palate with lidocaine/adrenaline solution. No sedation
implants 5 mm lateral to either side of the midline
was given. Surgery was performed by 3 of the authors (SN,
The patients were given penicillin V orally 660 mg 3 times
KW, and VB). The mucosa of the soft palate was perforated
a day for 7 days as a prophylaxis against infection and
in the midline about 5 mm distal to the trailing edge of the
diclofenac 50 mg 3 times a day as analgesic, if necessary.
hard palate with the insertion of the cannula moving through
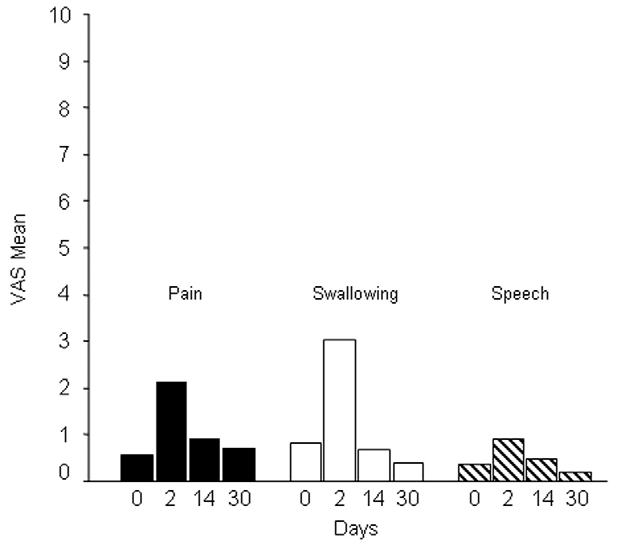
The VAS scores for pain, speech, and swallowing
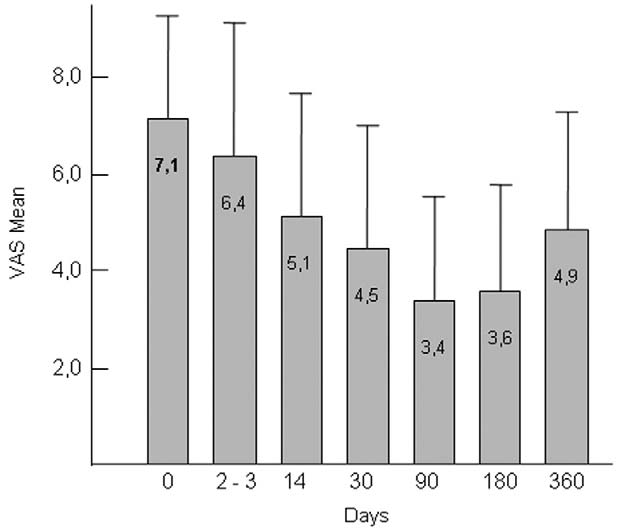
VAS score of snoring intensity before and after
difficulties at baseline (0) and 2, 14 and 30 days postoperatively.
Palatal implants for the treatment of . . . Table 2 Treatment success according to different criteria
Recurrence is defined as patients no longer fulfilling the criteria for success. Statistical Analysis
The implant procedure was easy to perform under
The statistical analyses of the results were performed with
local anesthesia with minimal discomfort for the patients.
the SPSS statistical program version 12 (SPSS Inc, Chicago,
Four implants were immediately replaced because of
IL). A Wilcoxon signed rank test was used for analysis of
paired data from VAS scores and ESS and a paired t test
placement. Average operation time was 8 minutes (range
when data had a normal distribution (AHI and body mass
3-16 minutes, decreasing with experience). There were
index [BMI]). When analyzing independent samples, a
no perforations of the soft palate. No bleeding, hema-
Mann-Whitney U test was used to compare data from 2
toma, or infection was experienced during the procedure
groups (satisfaction or extrusion related to physical param-
or in the follow-up period. The patients described the
eters and snoring-related symptoms). When these data had a
postoperative discomfort as a mild sore throat similar to
normal distribution, a t test was used. A chi-square test was
a beginning of an upper-airway infection. On average, the
used for analysis of categorical data in 2 groups. P values
patients took their prescribed analgesics 1.3 days after
the procedure (range 0-6 days), and mean total dose was2.1 pills of diclofenac 50 mg (range 0-15 pills). Eight ofthe patients (24%) did not take any analgesics at all. One
patient had a minor edema at the base of the uvula, whichresolved in 5 days. Two patients reported a mild transient
One patient was excluded from the study because of a
metal taste. No adverse swallowing or speech dysfunc-
tonsillectomy in the observation period. After this, the study
tion was noted. The VAS scores for pain, speech, and
group comprised 26 men and 8 women with a mean age of
43.7 years (range 23-67 years). The mean BMI was 26.1
The snoring intensity reported by the patient’s bed part-
(SD 2.3) and did not change significantly after 1 year (BMI
ners throughout the observation period is described in
26.3, SD 2.3). Four patients did not repeat the polysomnog-
The mean VAS value was reduced from 7.1 (SD 2.1)
raphy, leaving 30 pairs of data for comparison of the sleep
at baseline to 4.8 (SD 3.1) at 360 days (P Ͻ 0.001, Wil-
study results. There was no significant change in mean AHI
coxon signed ranks test). This corresponds to a reduction of
(baseline mean 2.2, SD 2.3 and 360 days mean 3.3, SD 3.8).
33.8% with 50% of the patients (17 of 34) having their
None of the patients withdrew from the study, and all
snoring reduced to less than or equal to 5. Eight of these
completed their follow-up visits at 2, 14, 30, 90, 180, and
(24% of the total group) had a final score of less than 3 on
the VAS scale for snoring intensity The ESS
Table 3 The relationship of partner satisfaction to snoring reduction and physical parameters
Otolaryngology–Head and Neck Surgery, Vol 134, No 4, April 2006
changed from 9.3 (SD 4.1) to 5.6 (SD 3.8) at 360 days (P Ͻ
mild foreign-body sensation, leaving a tip of the implant
0.001, Wilcoxon signed ranks test). At the last follow-up,
visible. Because patients reported improvement of snoring
70.6% (24 of 34) of the partners and 79.7% (27 of 34) of the
after temporary worsening related to partial extrusion, we
patients were satisfied with the results. The satisfaction rate is
did not replace any of the removed implants. The correlation
significantly associated with the snoring reduction in the VAS
of treatment results for the partial extrusion and nonextru-
Insufficient reduction of snoring was the reason for
sions groups may indicate an increased fibrosis caused by
not recommending the procedure among the unsatisfied
the partial extrusion process itself. Therefore, it is advisable
partners. Satisfactory snoring reduction was also inversely
to wait with the removal of a partially extruding implant a
correlated with the MMP (P Ͻ 0.05, Mann-Whitney U test)
few days until it penetrates the mucosa. This also facilitates
the removal itself. These observations are valid only for
During the observation period, 6 of the patients (17.6%)
partial extrusions taking place after 1 month because this
experienced a partial extrusion of, in total, 9 implants (8.8%
was the earliest-occurring partial extrusion in this study.
of 102 implants). Three of the patients experienced 2 partial
The partial extrusions took place with no regular consis-
extrusions. Partial extrusions were only seen with the lateral
tency or pattern from 1 to 12 months postoperatively. Only
implants, 6 on the right and 3 on the left side. The most
one of the patients with a partial extrusion had a partner
common site for partial extrusion was the cranial end of the
dissatisfied with the result and that partial extrusion oc-
palate, corresponding to the insertion site, where 6 extru-
curred at 7½ months. There were no parameters that could
sions took place. The remaining 3 implants were partially
predict a partial extrusion, except for the first-observed
exposed at the caudal end of the palate. One implant was
partial extrusion (1 month) in which the implant was placed
removed under local anesthesia, and the others were easily
too superficial during the procedure and was visible under
retracted with a forceps without any anesthesia. None of the
the mucosa. However, the fact that all partial extrusions
partially extruded implants were replaced.
were lateral indicates that a partial extrusion is more likely
There was no significant difference in snoring intensity
when the tissue thickness is low. Therefore and despite the
reduction or partner/patient recommendation between the
patients’ wishes, we have not advised any placement of
extrusion and the nonextrusion group No re-
additional implants further laterally in patients that may
corded physical parameters could be correlated to the oc-
benefit from an additional “tune-up” palatal surgery. In-
stead, partial uvula resection or RF treatment of the otherparts of the palate may be an option. From our data, there isno evidence that there is an increase in obstructive eventswith the use of palatal implants. Only one of the patients
DISCUSSION
changed from an AHI of less than 10 to an AHI of greaterthan 10 (4.8-18.4). This patient had only hypopnea and went
The use of these implants introduces a new philosophy of
from a preoperatively 50% high to a mainly low (84%)
stiffening the palate to reduce snoring. Unlike UPPP,LAUP, RF, CAPSO, and injection snoreplasty where scar-
location of the obstructive events. The Camtech Reggie
ring takes place after tissue resection or ablation, this pro-
system is a powerful tool for discriminating between high
cedure causes virtually no tissue damage and the implants
and low obstructions. However, when the AHI is less than
serve as a template for fibrous ingrowths. This is reflected in
5, the site of obstruction varies considerably from night to
the very low patient morbidity observed in this study. No
The sleep study findings were not emphasized here
mucosal breakdown, palatal swelling, discomfort, or fistu-
because of the fact that 15 of 34 patients (42%) showed no
obstructive events at all and the rest of this population also
noted with the palatal implant system. In this study, pain
had low figures (median AHI 1.0). When evaluating patients
was not registered on a day-to-day basis, but the objective
with more obstructive events and sleep apnea, however,
data related to analgesic use places it at least similar to the
these figures will be helpful and can override the physical
most favorable results from However, the single pro-
parameters. Traditionally, evaluation of site of obstruction
cedure results in less total trauma for the patient. RF also is
is based on clinical evaluation and radiography and even-
a heterogeneous and nonstandardized procedure. Because
tually endoscopic evaluation under anesthesia. However,
the implants procedure is standardized, the learning curve
these methods are highly subjective and are not based on the
will be short and mastering a technique will also reduce the
number of complications. Interestingly, swallowing discom-
No consensus has been reached regarding the evalua-
fort was significantly less at the 14-day control period than
tion of treatment results, and VAS scales frequently dif-
preoperatively. This may be attributed to less dryness of the
fer. Therefore, the comparison of the results between
different studies is difficult. Yet-suggested criteria for
Hypothetically, the most serious complication related to
success include endpoints such as VAS Ͻ3,VAS Ͻ5,
the implant method would probably be an extrusion fol-
VAS reduction ϾVAS reduction Ͼor differ-
lowed by aspiration and pneumonia. In all 9 partial extru-
ent statements of patient/partner satisfactionIn this
sions, however, the process was gradual and proceeded by a
study, 4 of the partners reported an initial VAS score Ͻ4,
Palatal implants for the treatment of . . . Table 4 Implant extrusions related to physical parameters and treatment results
the lowest 1.8 with the use of earplugs. In these patients,
After a median of 1.8 (range 1-3) treatments, 75% of 27
the 3 that reported satisfaction with the results, a defini-
patients receiving injection sclerotherapy in the palate re-
tion of VAS Ͻ5 or VAS Ͻ3 as success, would be mean-
ported a greater-than 50% reduction of pretreatment snoring
ingless and a reduction of 4 units would be impossible
For LAUP, success figures for treating snoring is
because the baseline scores were low. We have therefore
reported in the range of 57% to but in the latter
focused on partner satisfaction when evaluating the re-
study 10% and 8% had concomitant surgery on tonsils or
sults and searching for factors that can predict a favorable
turbinates. Relapse rates in the same populations were re-
outcome. Interestingly, partner satisfaction was signifi-
cantly associated with endpoint VAS score and VAS
The gradual reduction of snoring for up to 3 months
score reduction (P ϭ 0.002 and P ϭ 0.007, Mann-Whit-
postoperatively corresponds well with the time observed
ney test). It is not surprising that favorable results are
for PET-induced fibrosis to take place. Together with the
related to low MMP, which is an indicator of tongue size
observation that results are the same after a partial ex-
and hence a possible contributor to subpalatal snoring.
trusion, this indicates that the induced fibrosis is more
When selecting only patients with an MMP class of I or
important than the presence of the implants themselves.
II, the partner satisfaction with the result increases from
All operations aimed at treating snoring by stiffening thepalate seem to tell a quite similar history of a significant
70% to 84% (16/19 cases) in this study population. This
initial reduction in snoring and a partial relapse over
shows the importance of proper patient selection for this
time, either by palatal stretching or by increased contri-
targeted procedure, and the lack of selection for MMI in
bution from other parts of the upper airway, possibly also
this study should be kept in mind when comparing the
combined with some wearing off of an initial placebo
results with other studies. Reports on long-term results
effect. The variations reported in the different studies are
for the different treatment modalities are relatively few,
probably caused by different patient selection and by the
but all include a proportion of relapse to snoring symp-
degree of palatal fibrosis achieved by adjusting the de-
toms over time. Regarding RF treatment, Ferguson et a
gree of trauma in the palatal tissues. When the treatment
showed that 61% had VAS reduction of 50% after 16
results are quite similar, the choice of method therefore
months but with 1.9 treatments per patient. The VAS
will be more focused on discomfort, morbidity, safety,
reduction per treatment session in the multilesion group
and cost. It also seems logical to try to conserve the
was 2.1, which is comparable to our results. The study
delicate tissues of the palate like muscle, nerve ends, and
was, however, limited to patients with MMP Ͻ3. Bäck et
salivary glands without tissue destruction. In all these
showed VAS scores of 9, 4 and 6 at baseline, 3 and
respects, palatal implants compete favorably.
12 months after 2 treatment sessions. The total VAS
Limitations of this study are a relatively small series, the
reduction of 33% was very close to the results in our
lack of a control group, and the limited objective data for
study. Said and reported a 52% improvement
snoring assessment. Further studies should include a ran-
(11% reported deterioration after 2 months) on the VAS
domized, controlled study with placebo (no implant) and the
and a patient satisfaction rate of 67%. The data collection
use of different rigidity of the implants.
was done retrospectively, and only patients with MMPI/IA were included. Li et had better results, with anend score of 3.8, but the patients had several treatments(n ϭ 3.6, SD 1.2). Forty-one percent reported relapse
CONCLUSION
during mean follow-up of 14 months. On the other hand,Trotter et used only a single session, with 22%
The palatal implant system is safe, and the procedure is
improving greater than 50% after 17 months and 44%
associated with a very low patient morbidity and virtually
recommending the procedure. In a 1-year follow-up after
no tissue damage. The effectiveness in treating snoring is
CAPSO, 77% of patients reported that snoring was no
comparable to other surgical methods, but the patient selec-
longer a problem compared with 92% at 4 to 6 weeks
tion is important and can affect the outcome. Up to 30% of
Otolaryngology–Head and Neck Surgery, Vol 134, No 4, April 2006
patients are unsatisfied at 1 year, but this figure can be
9. Friedman M, Tanyeri H, La Rosa M, et al. Clinical predictors of
reduced significantly by selecting only patients with MMI
obstructive sleep apnea. Laryngoscope 1999;109:1901–7.
10. Emery BE, Flexon PB. Radiofrequency volumetric tissue reduction of
3. Partial extrusion of 1 or 2 implants, the most frequently
the soft palate: a new treatment for snoring. Laryngoscope 2000;110:
observed adverse reaction, does not affect the overall treat-
ment results. The advantages when compared with other
11. Troell RJ, Powell NB, Riley RW, et al. Comparison of postoperative
methods are simplicity, low cost, and minimal patient dis-
pain between laser-assisted uvulopalatoplasty, uvulopalatopharyngo-
comfort from only a single procedure in which the majority
plasty, and radiofrequency volumetric tissue reduction of the palate. Otolaryngol Head Neck Surg 2000;122:402–9.
of bed partners remained satisfied long term.
12. Rollheim J, Tvinnereim M, Sitek J, et al. A 2-night study based on
recordings of airway pressures and flow. Eur Arch Otorhinolaryngol2110;258:259 – 64.
13. Blumen MB, Dahan S, Wagner I, et al. Radiofrequency versus LAUP
REFERENCES
for the treatment of snoring. Otolaryngol Head Neck Surg 2002;126:67–73.
14. Ferguson M, Smith TL, Zanation AM, et al. Radiofrequency tissue
1. Fujita S, Conway W, Zorick F, et al. Surgical correction of anatomic
volume reduction: multilesion vs. single-lesion treatments for snoring.
abnormalities in obstructive sleep apnea syndrome: uvulopalatopha-
Arch Otolaryngol Head Neck Surg 2001;127:1113– 8.
ryngoplasty. Otolaryngol Head Neck Surg 1981;89:923–34.
15. Trotter MI, D’Souza AR, Morgan DW. Medium-term outcome of
2. Kamami YV. Laser CO for snoring: preliminary results. Acta Oto-
palatal surgery for snoring using the Somnus unit. Laryngol Otol
rhinolaryngol Belg 1990;44:451– 6.
3. Finkelstein Y, Stein G, Ophir D, et al. Laser-assisted uvulopalatoplasty
16. Said B, Strome M. Long-term results of radiofrequency volumetric
for the management of obstructive sleep apnea. Myths and facts. Arch
tissue reduction of the palate for snoring. Ann Otol Rhinol Laryngol
Otolaryngol Head Neck Surg 2002;128:429 –34.
4. Croft CB, Golding-Wood DG. Uses and complications of uvulopala-
17. Berger G, Finkelstein Y, Stein G, et al. Laser-assisted uvulo-
topharyngoplasty. J Laryngol Otol 1990;104:871–5.
palatoplasty for snoring: medium- to long-term subjective and
5. Mair EA, Day RH. The cautery assisted palatal stiffening operation.
objective analysis. Arch Otolaryngol Head Neck Surg 2001;127:
Otolaryngol Head Neck Surg 2000;122:547–55.
6. Powell NB, Riley RW, Troell RJ, et al. Radiofrequency volumetric
18. Sharp HR, Mitchell DB. Long-term results of laser-assisted uvulopala-
tissue reduction of the palate in subjects with sleep-disordered breath-
toplasty for snoring. J Laryngol Otol 2001;115:897–900.
19. Bäck L, Palomaki M, Piilonen A, et al. Sleep-disordered breathing:
7. Brietzke SE, Mair EA. Injection snoreplasty: extended follow-up and
radiofrequency thermal ablation is a promising new treatment possi-
new objective data. Otolaryngol Head Neck Surg 2003;128:605–15.
bility. Laryngoscope 2001;111:464 –71.
8. Nordgård S, Wormdal K, Bugten V, et al. Palatal implants: a new
20. Li KK, Powell NB, Riley RW, et al. Radiofrequency volumetric
method for the treatment of snoring. Acta Otolaryngol 2004;124:
reduction of the palate: an extended follow-up study. Otolaryngol
“Sobre los modos de amar” Pbro. Dr. Julián Arturo López Amozurrutia Tribunal Eclesiástico de la Arquidiócesis de México 27 de julio de 2009 – 9 de septiembre de 2009 Introducción Se me ha solicitado en esta sede presentar algunas ideas sobre lo que la razón humana ha logrado acuñar en torno al tema de los modos de amar, que pueda ser de ayuda para los jueces ecl
Dr. med. Hans-Dieter Hüwer œ Spessartstraße 27 A rbeitsbereich L ernen V erhalten A ufmerksamkeit Einnässen (Enuresis) Stadien der Blasenkontrolle 1. Phase unbewußte Blasenentleerung ohne zentrale Steuerung: afferente Deh- nungsreize über Reflexbögen im Hirnstamm bewirken die Blasenentleerung; Säug- linge bis zu 20 mal pro Tag im ersten Lebenshalbjahr; die
 Palatal implants for the treatment of . . .
Palatal implants for the treatment of . . .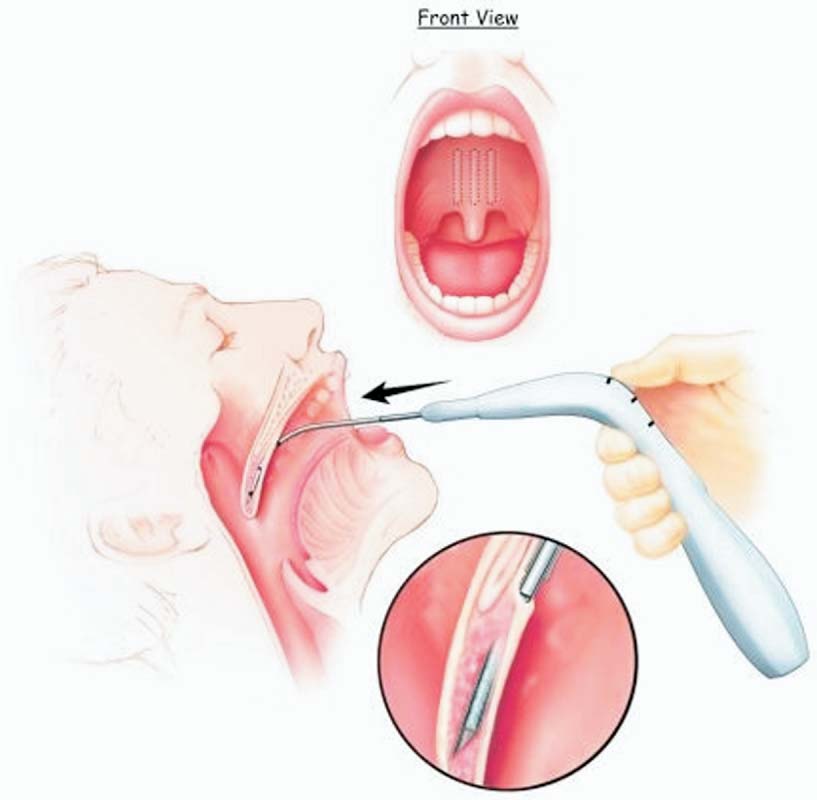
 Otolaryngology–Head and Neck Surgery, Vol 134, No 4, April 2006
The implantation procedure. Three implants are placed parallel to the midline in the muscular layer of the palate.
Otolaryngology–Head and Neck Surgery, Vol 134, No 4, April 2006
The implantation procedure. Three implants are placed parallel to the midline in the muscular layer of the palate.