Pak J Physiol 2006; 2(2) EFFECT OF SILDENAFIL CITRATE (VIAGRA) ON PENILE VASCULATURE AND CARDIODYNAMICS IN DIABETIC MALES WITH AND WITHOUT NEUROPATHY Syed Tabrez Ali*, Nabeeh I. Rakkah Department of Physiology, Faculty of Medicine and Medical Sciences, Umm-Al-Qura University, Makkah, Saudi Arabia Background: Erectile and cardiovascular dysfunctions in diabetes are important signs resulting probably due to pelvic autonomic neuropathy with damage to the parasympathetic nervierignetes. Direct evidence for a neuropathic etiology comes from studies that show structural changes in autonomic nerve fibers supplying the corpora cavernosa. The present study deals with the diabetic neuopathies prevailing in men and the possible role of sildenafil citrate (Viagra) treatment for these neurogenic cardio-sexual disturbances. Methods: Penile mid shaft circumference and length, penile pulse amplitude, both systolic and diastolic blood pressure s, and heart rate were measured in response to erotic stimulation by film and fantasy and the effect of the treatment of sildenafil citrate (50 mg oral dose) was noted in 50 insulin dependent diabetes mellitus (IDDM) and in 50 non insulin dependent diabetes mellitus (NIDDM) patients with and without an objective evidence of neuropathy, having an age span in between 20 and 65 years and a duration of diabetes distributed over 1-25 years with their age matched non diabetic controls. Results: Sildenafil treatment showed a significant increase (P<0.0005) in penile mid shaft circumference and length, and penile pulse amplitude, where as both systolic and diastolic blood pressure s and heart rate exhibited a significant decrease (P<0.025 and P<0.005 respectively) in both IDDM and NIDDM diabetic neuropathic patients. However this difference was found to be non-significant in both types of diabetic patients without neuropathy and when compared with their respective control subjects . Conclusion: Oral administration of sildenafil citrate is an effective first line therapy for erectile dysfunctions in diabetic impotent men with neuropathic etiology (irrespective of their type of diabetes) with out much altering the cardiodynamic profile. These results further explain how to manage sexual disorders as part of diabetic care, and suggest rules for sildenafil prescription in diabetic neuropathic patients. Key Words: Diabetes; Neuropathy; Erectile/cardiovascular response; Sildenafil citrate. INTRODUCTION
with involvement of the sympathetic fibers that sub
Erectile dysfunction (ED) has been linked
serve the seminal vesicles, vas deferens, and bladder
increasingly to cardiovascular risk factors and
comorbidities. Considering the potential
associated with sexual activity, guidelines were
neurogenic bladder, and delayed bulbocavernous
developed (Princeton I) for assessment and
reflex response latency are indirect evidence for a
management of patients with varying degrees of
neuropathic etiology of the patient's complaints5.
cardiac risk. These guidelines are most recently
Failure of ejaculation secondary to emission
updated (Princeton II) based on new data concerning
disturbances due to sympathetic denervation of the
the link between ED and cardiovascular disease and
vas deferens is another manifestation of autonomic
the availability of additional phosphodiesterase type
neuropathy, usually seen in more advanced stages 6-7.
5 inhibitors vardenafil, tadalafil1. Despite the need for
It is now established that sexual dysfunction is a
careful risk assessment in all cases, sexual activity
common complication of diabetic autonomic
remains safe for the large majority of patients.
neuropathy both in men and in women8-9-10-11. Despite
However, all patients presenting with complaints of
the general agreement of previous investigators that
ED should be carefully assessed for the presence of
the prevalence of impotence in diabetic men
cardiovascular risk factors like obesity, hypertension,
approximates 50 per cent, there is controvers y
hyperlipidemia, diabetes and its associated
surrounding the etiology of this problem.
Direct evidence for a neuropathic etiology of
neurological dysfunction of diabetic autonomic
diabetic erectile dysfunction comes from studies that
show structural changes in autonomic nerve fibers
blood pressure homeostasis in a number of ways. The
disturbances that occur in diabetes are associated
efferent limb of the baroreceptor reflex is composed
Pak J Physiol 2006; 2(2)
of sympathetic vasoconstrictor fibers to the
MATERIALS AND METHODS
splanchnic, skin, and striated muscle vessels and sympathetic cardiac fibers. Interruption of these
For experimental purposes and for the studies of
fibers interferes with three compensatory
diabetic neuropathy, after getting the permission from
mechanisms: vasoconstriction, i.e., a drop in systolic
the local ethical committee, 50 insulin dependent
blood pressure of 30 mmHg or greater. The lack or
(IDDM) and 50 non insulin dependent (NIDDM)
inadequacy of the expected increase in heart rate
diabetic male patients with and without evidence of
differentiates the orthostatic hypertension of
neuropathy and 50 age matched non diabetic male
autonomic neuropathy from those seen under
controls were selected. Every male aged between 20
hypovolaemic conditions such as dehydration or
to 65 years with duration of the onset of the disease
The presence of diabetic complications were
diastolic supine blood pressure have been described
assessed by a review of the medical record.
in diabetic impotent patients with idiopathic
Neuropathy was present if the records indicated
autonomic dysfunction following food ingestion16-17.
absence of ankle jerk, decreased vibration sense or
However, the pathologic basis |of diabetic autonomic
pin prick sensation in the feet or hands, or there was
neuropathy is still incompletely understood.
history of neuropathic pain, foot ulcer, or symptoms
compatible with autonomic neuropathy (differential
treatment of erectile and cardiovascular dysfunctions
diagnosis) including postural hypotension,
using oral drugs lies in the substance sildenafil citrate
intermittent diarrhea especially nocturnally,
(ViagraTM) seems to be a most promising discovery18.
epigastria fullness, bladder dysfunction, diminished
Sildenafil is a potent and selective inhibitor of the
sweating in the legs, gustatory sweating and
cyclic guanosine monophosphate (cGMP)-specific
hypoglycemic unawareness. The criteria for the
phosphodiesterase type 5 (PDE5), which is
presence of symptomatic autonomic neuropathy were
responsible for the degradation of cGMP in the
two or more severe or three or more mild/moderate
Sildenafil has a peripheral site of action on
Impotence was determined according to the
erections. It potently enhances the relaxant effect of
method described previously21. Men were considered
nitric oxide (NO) on this tissue. When the NO/cGMP
candidates for this study when they had complained
pathway is activated, as occurs with sexual
of erectile dysfunction with diabetic neuropathy for 6
stimulation, inhibition of PDE5 by sildenafil results
or more months. All candidates had normal results on
in increased corpus cavernosum levels of cGMP.
Increased levels of cGMP are involved in smooth
hypothalamic pituitary axis as obtained by their
muscle relaxation, which in turn leads to penile
erection. cGMP is converted back to guanosine
monophosphate (GMP), a cGMP precursor, by the
alone, oral hypoglycemic agent or insulin. Inquiry
action of phosphodiesterase type 5 (PDE5). Sildenafil
was made of other drug therapy, angina pectoris,
prevents the breakdown of cGMP thereby preventing
previous myocardial infarction or cardiac failure,
premature detumescence. Furthermore, treatment
intermittent claudication, thyroid dysfunction,
with sildenafil is well tolerated and is associated with
previous sympathectomy or other abnormality that
minimal adverse events that rarely cause
might predispose to organic impotence such as
discontinuation of the treatment. It relaxes vascular
neurological disease or previous injury.
smooth muscle, resulting in modest reductions in
To assess the efficacy and safety of oral
blood pressure that are insufficient to stimulate a
sildenafil citrate (Viagra TM-Pfizer) in the treatment of
reflex increase in heart rate. Sildenafil does not affect
erectile dysfunctions in both IDDM and NIDDM
the force of cardiac contraction, and cardiac
diabetic men with and without neuropathy and in age
performance is unaffected. Sildenafil is mildly
matched non diabetic controls, subjects home and
vasodilating in the coronary circulation and does not
clinical practice centers in the local vicinities, were
increase the risk of ventricular arrhythmia. Among
randomized to receive sildenafil citrate (50 mg), but
men with erectile dysfunction treated with sildenafil,
not more than once daily, for 12 months. Self-
the adverse event profile is similar overall to that in
reported ability to achieve and maintain an erection
men with comorbid cardiovascular disease (CVD), it
for sexual intercourse according to the International
is similar between those with and without CAD, and
Index of Erectile Function and adverse events were
it is similar between those who take and those who
recorded according to the method described
do not take antihypertensive drugs (regardless of the
Pak J Physiol 2006; 2(2)
Erectile and cardiovascular responses were
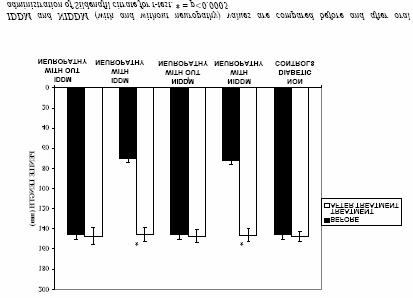
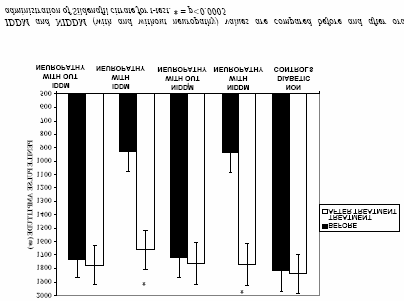
Exactly in a similar manner, values of penile
assessed using simultaneous monitoring of penile
length and penile pulse amplitude showed a
mid shaft circumference & length, penile pulse
significant increase (p<0.0005) in both types of
amplitude, systemic arterial systolic & diastolic blood
sildenafil treated diabetic neuropathic patients when
pressures & heart rate during laboratory based erotic
compared with the values obtained from untreated
stimulation with film and fantasy before and after the
patients (Figures 2 & 3). However this difference was
sildenafil treatment in all the subjects according to
found to be non-significant in both types of diabetic
patients without neuropathy before and after oral
The degree of erection to erotic film &
administration of sildenafil and when compared with
fantasy distinguished between neuropathic & non-
neuropathic etiologies. The initial approach was tentative so that it was easy for the individuals to decline without embarrassment. If there was apparent willingness, a more definite request was made. All the parameters were statistically analyzed using Student t-test. In all the instances probability (p<0.05) was regarded as statistically significant.
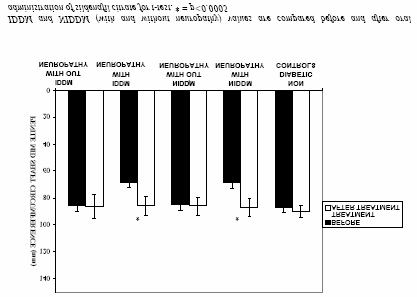
The data for the measurement of penile mid shaft circumference in response to film and fantasy before and after the administration of 50 mg of oral dose of sildenafil citrate in 50 IDDM and 50 NIDDM diabetics (with and without neuropathy) and in 50 age matched non diabetic control subjects is shown in Figure- 1.
Figure-2: Changes in penile length (mm) before and after oral administration of sildenafil citrate (50 mg dose) in response to erotic film and fantasy in insulin dependent (IDDM) and non-insulin dependent (NIDDM) diabetic males (with and without neuropathy) and in age matched non diabetic control subjects. Values are means ± S.D. Figure-1: Changes in penile mid shaft circumference (mm) before and after oral administration of sildenafil citrate (50 mg dose) in response to erotic film and fantasy in insulin dependent (IDDM) and non insulin dependent (NIDDM) diabetic males (with and without neuropathy) and in age matched non diabetic control subjects. Values are means ± S.D. Figure-3: Changes in penile pulse amplitude (µv) before
A consistent increase in the values of penile
and after oral administration of sildenafil citrate (50 mg
circumference in both IDDM and NIDDM diabetic
dose) in response to erotic film and fantasy in insulin
patients with neuropathy was observed with a
dependent (IDDM) and non-insulin dependent
significant statistical difference (P<0.0005) after the
(NIDDM) diabetic males (with and without neuropathy)
sildenafil treatment, the increase being about 26%
and in age matched non diabetic control subjects. Values are means ± S.D. Pak J Physiol 2006; 2(2)
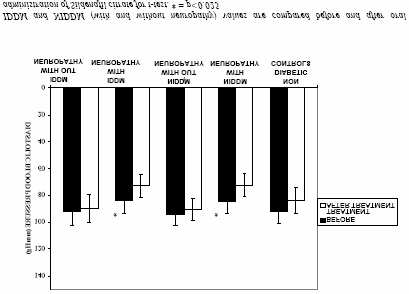
types of treated diabetic patients without neuropathy showed a non-significant difference in levels systolic and diastolic blood pressures and heart rate when compared with the untreated patients and their age matched control subjects.
An interesting feature in these experiments
was about 7% decrease in the values of systolic and diastolic blood pressure and about 6% decrease in the values of heart rate after the oral administration of 50 mg of sildenafil in non-diabetic controls. In addition, no difference was observed when the IDDM and NIDDM values were compared with each other either before or after the oral administration of sildenafil in all groups (data not shown).
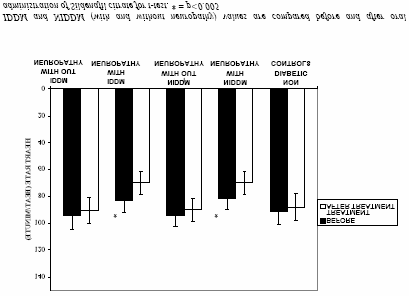
Figure-4: Changes in systolic blood pressure (mmHg) before and after oral administration of sildenafil citrate (50 mg dose) in response to erotic film and fantasy in insulin dependent (IDDM) and non insulin dependent (NIDDM) diabetic males (with and without neuropathy) and in age matched non diabetic control subjects. Values are means ± S.D. Figure-6: Changes in heart rate (beat/minute) before and after oral administration of sildenafil citrate (50 mg dose) in response to erotic film and fantasy in insulin dependent (IDDM) and non insulin dependent (NIDDM) diabetic males (with and without neuropathy) and in age matched non diabetic control subjects. Values are means ± S.D. DISCUSSION Figure-5: Changes in diastolic blood pressure (mmHg)
Laboratory assessment of erectile response to erotic
before and after oral administration of sildenafil citrate
stimuli has been used for many years to assess sexual
(50 mg dose) in response to erotic film and fantasy in
preferences as the out come of modification of
insulin dependent (IDDM) and non insulin dependent
deviant sexual behavior21, but only one published
(NIDDM) diabetic males (with and without neuropathy)
study23 has used this procedure in the investigation of
and in age matched non diabetic control subjects.
erectile dysfunction. In the recent years, there has
Values are means ± S.D.
been increasing recognition that many cases of
In contrast, an inverse relationship was
erectile dysfunctions are due, at least in part, to
found when systolic and diastolic blood pressures and
physical factors. This has led to a renewed interest in
heart rate values were measured in the same group of
the physiological mechanism of normal erection and
search for methods of investigating erectile function
neuropathic treated patients showed a significant
that may have diagnostic value. Evidence indicates
decrease (p<0.025) in the values of systolic and
that erection may involve the activation of several
diastolic blood pressure (Figures-4 and 5) and
comparatively a more significant decrease (P< 0.005)
parasympathatically mediated arterial vasodilatation,
in values of heart rate (Figure-6). However, both
there may also be active reduction of venous
Pak J Physiol 2006; 2(2)
drainage25 and the active closure of intra cavernosal
after the oral administration of 50 mg of sildenafil
arterio-venous shunts 26. None of the established
(Viagra) in both IDDM and NIDDM diabetic
methods of investigating penile dysfunction is wholly
neuropathic patients. However this difference was
satisfactory. The most widely used techniques for
found to be non-significant in both types of diabetic
laboratory studies are either concerned with
patients without neuropathy before and after oral
physiological state of non-erect penis e.g.
administration of sildenafil and when compared with
measurement of penile blood pressure27-28 or involve
invasive procedures such as xe non washout25,
arteriography and artificial erection29-30 and the usual
determinant of the quality of an erection. Based on
non-invasive method of investigating the erect penis
published evidence it is suggested that a penile
is to measure erections during sleep. However, this
rigidity of >70% is adequate for sexual intercourse33.
does necessitate over night observation of the
Because sildenafil is believed to exert its beneficial
effects by inhibiting the phosphodiesterase type-V
In a study laboratory based procedure for
enzyme and, therefore, increasing the intracellular
monitoring penile diameter and dorsal penile arterial
levels of cGMP in the corporal smooth muscle, it
pulse during presentation of erotic stimuli has been
would not be expected to produce an erectile
described in the normal subjects10. The results
response when used in the absence of a drive on the
indicate the aspects of the erectile response, which
nitric oxide-cGMP pathway. This drive can be
may be vulnerable to different pathological
provided by physiological mechanisms that can be
processes31. The etiology of erectile impotence
initiated by visual or other forms of sexual
associated with diabetes mellitus has been reported to
stimulations. As such, sildenafil may be expected to
be neuropathic abnormality in the male genital organ
enhance relaxation of the corpus cavernosal smooth
and/or vascular change in the corpora cavernosa.
muscle, which in turn increases blood flow into the
However, the diagnostic assessment and the
cavernosal spaces, thus leading to increased
treatment of the neuropathic factor has been
intracavernosal pressure, a key factor in producing an
impended by the lack of an objective laboratory test.
Sildenafil citrate relaxes vascular smooth
Our results suggest that oral administration
muscle, resulting in modest reductions in blood
of sildenafil improves the quality of erection in both
pressure that are insufficient to stimulate a reflex
IDDM and NIDDM neuropathic group of patients.
increase in heart rate. These blood pressure
We thus conclude that sildenafil citrate is an effective
reductions are similar for healthy men and men with
first-line therapy for erectile dysfunction in diabetic
coronary artery disease (CAD) or who use
men with impotence of neuropathic etiology. These
antihypertensive drugs. Sildenafil does not affect the
results further explains, how to manage sexual
force of cardiac contraction, and cardiac performance
disorders as part of diabetic care, and suggests rules
is unaffected. Sildenafil is mildly vasodilating in the
for sildenafil’s prescription in diabetic neuropathic
coronary circulation and does not increase the risk of
ventricular arrhythmia. During exercise and recovery,
In contrast to above mentioned findings we
sildenafil does not cause clinically significant
found a decrease in the values of systolic and
alterations in hemodynamic parameters in men with
diastolic blood pressures (P<0.025) and heart rate
CAD, and it has no negative effects on coronary
(P<0.005) in both types of diabetic neuropathic
oxygen consumption, ischemia, or exercise
patients after the sildenafil treatment, where as this
difference was found to be non significant in both
types of non neuropathic diabetics when compared
designed to compare the efficacy of sildenafil citrate
with their respective control subjects. A decrease in
on erectile and cardiovascular responses to erotic
pressure responses and heart rate after the sildenafil
stimulations in IDDM and NIDDM diabetics (with
treatment in IDDM and NIDDM diabetic neuropathic
and without neuropathy) and in age matched non-
patients is probably due to a decrease in peripheral
diabetic controls. The stimuli utilized were fantasy
resistance due to overall greater severity of
and film. Both of these stimuli produced striking
neuropathy in these individuals with sympathetic and
differences between those in whom neuropathic and
parasympathetic damage rather than from the effect
induced erectile factors were likely to under lie their
of parasympathetic damage in particular. In this
context, Jackson36 observed in one couple tested, that
Our results indicated that during the period
administration of beta-adrenergic receptor antagonist
of erotic stimulation to film and fantasy penile mid
prior to intercourse reduced the pressure response in
shaft circumference, penile length, and penile pulse
both sexes. This can be taken as an alternative
amplitude exhibited a significant increase (P<0.0005)
interpretation of our results. Our data indicate that
Pak J Physiol 2006; 2(2)
change in penile pulse amplitude is not produced
Rundles RW. Diabetic neuropathy, Medicine 1945; 24:
passively by change in systemic blood pressure, or by
Kolodny RC. Sexual dysfunction in diabetic female.
the gross alteration in physical properties of penis
consequent upon erection. The increase in penile
10. Ellenberg M. Development of urinary bladder
pulse amplitude during arousal is therefore likely to
dysfunction in diabetes mellitus. Ann Intern Med 1980;
reflect local vascular events, markedly affected by
11. Jackson G. Sexual dysfunctions and diabetes. Int J Clin
sildenafil treatment. These results are in conformity
with the previous findings37. However, a strict
12. Benet AE, Melman A. The epidemiology of erectile
relationship between penile blood flow and penile
dysfunction. Urol Clin North Am 1995; 21: 699-709.
pulse amplitude cannot yet be assumed until we have
13. Jackson G. Erectile dysfunction and vascular risk: Let’s
14. Crnily CM, Schade RR, Van DH, Gavaler JS. Chronic
Our results in general suggest that parallel
advanced liver disease and impotence cause and effect?
development of circumference, length and penile
pulse amplitude increase is associated with more
15. English KM, Mandour O, Steeds RP, Diver MJ, Jones
TH, Channer KS. Men with coronary disease have low
rapid erection, whilst if penile amplitude increase
levels of androgens than men with normal coronary
does not occur at all, erections tends to be smaller in
angiograms. Europ Heart J 2000; 21:890-4.
16. Ignarro LJ, Lippton H, Edwards JC. Mechanism of
In conclusion, these results suggest that sildenafil
vascular smooth muscle relaxation by organic nitrates, nitrites nitroprusside and nitric oxide evidence for the
citrate is an effective and well-tolerated treatment for
involvement of S- nitrosothiols as active intermediates.
erectile dysfunction in patients with diabetic
neuropathy. It does not cause major decreases in
17. Thompson IM. Erectile dysfunction and cardiovascular
blood pressure. It is associated with small additive
18. Solomon H, Wierzbicki AS, Lumb PJ, Lambert HM,
decreases rather than large synergistic decreases.
Jackson G. Cardiovascular risk factors determine
However, experimental studies to date do not suggest
erectile and arterial function responses to Sildenafil.
that sildenafil citrate causes a coronary artery steal
phenomenon38. Because there is a small but finite risk
19. Goldstein I, Lue TF, Padma- Nathan H, Rosen RC,
Steers WD, Wicker PA. Oral sildenafil in the treatment
of having a cardiac event with sexual activity with
of erectile dysfunction. J Urol 2002; 167:1197-1204.
20. Fujiswa M, Sawada K. Clinical efficacy and safety of
recommended to ask the diabetic neuropathic patients
sildenafil citrate in elderly patients with erectile
about their cardiac status before the administration of
dysfunction. Arch Androl 2004; 4:255-60.
21. Bancroft J, Bell C. Simultaneous recording of penile
sildenafil, since it may produce systemic vasodilatory
diameter and penile arterial pulse during laboratory
properties and can potentially lowers the blood
based erotic stimulation in normal subjects. J Psychom
22. Rosen RC, Riley A, Wagner G, Osterloh IH,
REFERENCES
Kirkpatrick J, Mishra A. The International Index of Erectile Function (IIEF): a multidimensional scale for
Rosen RC, Jackson G, Kostis JB. Erectile dysfunction
assessment of erectile dysfunction. Urology 1997;
and cardiac disease: recommendations of the Second
Princeton Conference. Curr Urol Rep 2006; 6: 490-6.
23. Kockott G, Fiel W, And Ferster R, Besinger V.
Jackson G, Montorsi P, Cheitlin MD. Cardiovascular
Psychological aspect of male inadequacy: results of an
safety of sildenafil citrate (Viagra): an updated
experimental study. Arch Sex Behav 1980; 9:477-94.
24. Braunstein GD. Impotence in diabetic men. Mt Sinai J
Andersen BL, Broffitt. Is there a reliable and valid self-
report measure of sexual behavior? Arch Sex Behav
25. Wagner G. Vascular mechanisms involved in erection
and erectile disorders. Clinics In Endocrinol Metab
Guvel S, Pourbagher MA, Torun D, Egilmez T,
pourbagher A, Ozkardes H. Calcification of the
26. Sommer F, Klotz T, Engelmann U. Improved
epididymis and tunica albuginea of the corpus
spontaneous erectile function in man with mild to
cavernosa in patients on maintenance hemodialysis. J
moderate arteriogenic erectile dysfunction treated with
a nightly dose of Sildenafil for one year: a randomized
Jannini EA, Screponi E, Carosa E, Pepe M, Lo Giudice
trail. Asian J Androl 2007; 9(1):134-41.
F, Trimarchi F, Benvenga S. Lack of sexual activity
27. Fletcher EC, Martin RJ. Sexual dysfunction and erectile
from erectile dysfunction is associated with a reversible
impotence in chronic obstructive pulmonary disease.
reduction in serum testosterone. Int J Andrology 1999;
28. Anderson KM, Wilson PWF, Odell PM, Kannel WB.
Bramann HU, Aleff G. Autonomic neuropathy in
An updated coronary risk profile: a statement for health
diabetes mellitus and advanced age. Med Asp Hum Sex
professionals. Circulation 1998; 83:356-62.
29. Miccoli R, Giampietro D, Tognarelli M, Navalesi R.
Carosa E, Benvenga S, Trimarchi F, Lenzi A, Pepe M,
Prevalence and type of sexual dysfunction in diabetic
Simonelli C, Jannini EA. Lack of sexual activity for
males: a standard clinical approach. J Med 1987; 18:
erectile dysfunction causes a reversible
for LH bioavailability. Int J Impot Res 2002; 14:93-9.
Pak J Physiol 2006; 2(2)
30. Lugnier C, Komas N. Modulation of vascular cyclic
35. Zhang H, Fillipi S, Morelli A, Vignozzi L, Forti G,
nucleotide phosphodiesterase by cyclic GMP: role in
Maggi M. Testosterone restores diabetes induced
vasodilatation. Euro Heart J 1993; 14 (suppl-1):141-8.
erectile dysfunction and sildenafil responsiveness in
31. Faerman I, Vilar O, Rivarola MA. Impotence in
two distinct animal models of chemical diabetes. J Sex
diabetes: studies of androgenic function in diabetic
impotent males. Diabetes 1972; 21:23-32.
36. Jackson G. Should erectile dysfunctions be treated as
32. Huang ST, Hsieh ML. different hemodynamic
secondary prevention for coronary disease. Int J Cli
responses by Color Doppler ultrasonography studies
between Sildenafil non-responders and responders.
37. Webb DJ, Allen MJ, Muirhead GJ. Sildenafil citrate
and blood pressure lowering drugs: results of drug
33. Ogrinc FG, Linet OI. Evaluation for real-time Rigiscan
interaction studies with an organic nitrate and a calcium
monitoring in pharmacological erection. J Urol 1995;
38. Robert A, Kloner. Cardiovascular risk and Sildenafil.
34. Abosaif SR, Lue TF. Hemodynamics of penile erection.
______________________________________________________________________________ Address For Correspondence: Dr. Syed Tabrez Ali, Associate Professor, Department of Physiology, Faculty of Medicine and Medical Sciences, Umm-al-Qura University, P.O. Box 7607, Makkah, Saudi Arabia E-mail: shazali_2004@hotmail.com
• -35 to +80°C (-31 to +176°F) measurement range• USB interface for set-up and data download• Status indication via red, green and orange LEDs• Supplied with replaceable internal lithium This standalone data logger measures and stores up to 16,382 temperature readings over a -35 to +80°C (-31 to +176°F) range. The user can easily set up the logging rate and start-time, an
Wenn man zunehmend in die primäre Sozialisation eingreift, ihrer “Selbstregulierung” imRahmen alltäglicher lebender Systeme misstraut, sie faktisch zur Erziehungssituation umbaut,dann kommt es schnell zu einer Überlastung (Süddeutsche Zeitung 13.12.2008 WERNER BARTENS) Jetzt mal ganz ruhig - Das Zappelphilipp-Syndrom bleibt umstritten - zu oft vermuten überforderte Eltern und Ärzte
 Pak J Physiol 2006; 2(2)
Pak J Physiol 2006; 2(2) 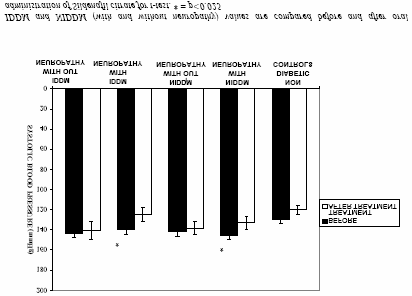
 Pak J Physiol 2006; 2(2)
Pak J Physiol 2006; 2(2)