Clinical characteristics of neuroleptic-induced parkinsonism S. Hassin-Baer1,*, P. Sirota2, A. D. Korczyn1,3, T. A. Treves1,**, B. Epstein2, H. Shabtai1, T. Martin2, Y. Litvinjuk2, and N. Giladi1
1 Movement Disorders Unit, Department of Neurology, Tel-Aviv Medical Center,
2 Department 6A, Abarbanel Mental Health Center, Bat-Yam,
3 Sieratzki Chair of Neurology, Tel-Aviv University, Ramat Aviv, and
Sackler School of Medicine, Tel-Aviv University, Tel-Aviv, Israel
Received May 8, 2001; accepted June 10, 2001
Summary. In order to characterize the clinical spectrum of neuroleptic- induced parkinsonism (NIP), we studied a population of consecutive psychiat- ric in-patients treated with neuroleptics for at least two weeks, who were diagnosed by their psychiatrist as having parkinsonism. Parkinsonism was confirmed by a movement disorders specialist who performed neurological assessment including the motor examination and the activities of daily living (ADL) sections of the Unified Parkinson’s Disease Rating Scale (UPDRS), and the Hoehn and Yahr (H&Y) staging.
Seventy-five patients (54 males), aged 46 Ϯ 13 years (range 21 to 73 years)
were included in the analysis. The mean duration of neuroleptic therapy was15 Ϯ 12 years, while 61% were treated for more than 10 years. Most of thepatients (n ϭ 66, 88%) were scored as H&Y stage 2.5 or less. Rest tremor waspresent in 44% of the patients, and usually persisted in action. Forty-onepatients (61%) had symmetrical involvement. Parkinsonian signs were signifi-cantly more common and pronounced in the upper in comparison with thelower limbs (p ϭ 0.0001). Gait disturbances were mild and freezing of gait wasvery rare (n ϭ 2). Neither age nor duration of therapy or their interactionaffected the total motor score or any of the motor sub-scores. In conclusion,NIP differs from PD for more bilateral involvement with relative symmetry,and by affecting upper limbs more often than the lower ones. NIP tends to beassociated with the triad of bradykinesia, tremor and rigidity while PD tends
Present addresses:* Department of Neurology, Sheba Medical Center, Tel-Hashomer, Israel** Department of Neurology, Rabin Medical Center, Campus Beilinson, Petach
to involve gait and posture more often. NIP develops unrelated to duration ofneuroleptic treatment or age of the patient, suggesting an individual predispo-sition to blockage of the dopaminergic receptors. Keywords: Drug induced parkinsonism, neuroleptic induced parkinsonism, antipsychotics, extrapyramidal side effects, symmetry. Introduction
Patients treated with neuroleptic agents, that is dopamine receptor blockingagents (DRBA) frequently exhibit extrapyramidal adverse events. Amongthese are dystonia, akathisia, dyskinesia and parkinsonism (Korczyn andGoldberg, 1976; Diederich and Goetz, 1998). Ever since the introduction ofDRBA for the treatment of psychosis forty years ago, neuroleptic-inducedparkinsonism (NIP) became a common movement disorder. Epidemiologicalstudies provide a wide range of NIP prevalence in different studies from5% to 90% (Ayd, 1961; Kennedy et al., 1971; Korczyn and Goldberg, 1976;Stephen and Williamson, 1984). Distinct diagnostic criteria and patient popu-lations, as well as exposure to different types and doses of neuroleptics mayexplain these differences. The clinical features of NIP develop within 1 to 3months after introduction of DRBA or dose increment (Stephen andWilliamson, 1984). After discontinuation, recovery occurs in 60–70% of thepatients within 7 weeks, although complete recovery may take 6 monthsor more (Klawans et al., 1973). Some patients do not recover and continueto exhibit parkinsonian features and a few deteriorate following drug with-drawal (Melamed et al., 1991). Another group of patients recovers tem-porarily until a syndrome identical to Parkinson’s disease (PD) reappearsmonths to years later (Kennedy et al., 1971; Wilson and Primrose, 1986). These observations cannot be fully explained by the accepted pathogenetichypothesis, which is based on dopamine receptor blockade. Positron emissiontomography (PET) studies showed reduced F18-fluoro-dopa uptake in somepatients with NIP, implying presynaptic dopaminergic nerve terminal dys-function as a contributory factor (Burn and Brooks, 1993). Dopaminergicpresynaptic dysfunction can be the result of primary degenerative process i.e. PD (Rajput et al., 1982) or the result of toxic effects of neuroleptics on theseterminals.
Several groups have described the clinical features of NIP. In most of the
studies the presence of various signs or symptoms were reported, withoutrating their severity or mentioning their exact topographical distribution(Kennedy et al., 1971; Korczyn and Goldberg, 1976; Stephen and Williamson,1984; Diederich and Goetz, 1998). The frequency of axial involvement (e.g. falls and gait disturbances) was rarely addressed and comparison to PD wasnot formally attempted.
The goal of the present study was to examine the clinical features of NIP
with the eyes and tools of movement disorders specialists, to find associatedfactors and to compare NIP to PD, in an attempt to improve our understand-ing of the relationship between these two disorders.
Clinical characteristics of neuroleptic-induced parkinsonism
The source population was composed of patients hospitalized in psychiatric departmentsat Abarbanel Mental Health Center in Bat-Yam, Israel, from December 1997 or July 1998were receiving neuroleptic therapy for at least 2 weeks and were suspected of havingparkinsonism by their treating psychiatrist. The study was approved by the hospitalHelsinki committee. All patients agreed to take part in the study and signed an informedconsent. The patients were examined by a movement disorders specialist, to confirm thepresence of parkinsonism. Patients were included if they fulfilled the DSM-IV (1994)criteria for NIP, while parkinsonism was considered if at least 2 out of the 4 cardinal signs(tremor, bradykinesia, rigidity and postural instability) were present. All patients whofulfilled the inclusion criteria were taken off anticholinergic treatment for at least 24 hoursand in most cases 48 hours before the motor assessment was performed according to theUnified Parkinson’s Disease Rating Scale (UPDRS) (Lang and Fahn, 1989). The pres-ence of other extrapyramidal features was not analysed.
Demographic information, medical history, family history of psychiatric or neurologi-
cal disorders, and careful history regarding pharmacotherapy were obtained from thepatient, treating psychiatrist and hospital records.
For the sake of statistical analysis UPDRS subscales were calculated for items from
the ADL section and from the motor examination. The subscores definitions are listedbelow:
– TADLS Total ADL score ϭ the sum of all items of the ADL section (items 5–
– TMS Total motor score ϭ the sum of all motor examination items (items 18–
– GTS Global tremor score ϭ the sum of the tremor item by history and tremor at
rest items by examination (items 16 and 20 for the face and four limbs).
– GBS Global bradykinesia score ϭ the sum of dexterity items (3 in each upper limb
and 1 in each lower limb) and the general bradykinesia item of the motor examina-tion (items 23, 24, 25, 26 and 31).
– GRS Global rigidity score ϭ the sum of 5 items of rigidity from the motor exami-
– PIGD score Postural instability gait difficulty score ϭ the sum of items from history
regarding falling, freezing and walking with items of gait and postural instabilityfrom the motor examination (items 13, 14, 15, 29 and 30).
– GS Gait score ϭ the sum of the item from history concerning walking and freezing
and the gait item from examination (items 14, 15, 29).
– UBS Upper body score ϭ the sum of all motor items from the upper limbs (the
mean of right and left upper limbs rest tremor, the mean of right and left upperlimbs rigidity and the mean of 3 items of dexterity in the right and left upper limbs)(items 20, 22, 23, 24 and 25).
– LBS Lower body score ϭ the sum of all motor items from the lower limbs
(the mean of right and left lower limbs rest tremor, the mean of right and leftlower limbs rigidity and the mean of right and left leg agility) (items 20, 22 and26).
– RS Right score ϭ the sum of all motor items from the right upper and right lower
limbs (tremor at rest, rigidity, 3 items of dexterity for right upper limb and one itemfor the lower) (items 20, 22, 23, 24, 25 and 26 of right side).
– LS Left score ϭ the sum of all motor items from the left upper and left lower limbs
(rest tremor, rigidity, 3 items of dexterity for left upper limb and one item for thelower limb) (items 20, 22, 23, 24, 25 and 26 of left side).
The associations between the different extrapyramidal features [e.g. tremor (GTS), rigid-ity (GRS), bradykinesia (GBS) or postural instability and gait disturbances (PIGD)] wereassessed using Pearson correlation test. The comparisons between upper to lower andright to left body scores were done using pairedt test. However for the comparison of
asymmetry, we used only the absolute differences between sides in the first case. Thescores obtained in the right and left sides were also reported on a scatter plot and linearregression lines were used to reflect asymmetry: in case of perfect symmetry the line isexpected to have a slope of 45 degrees and regression coefficient of 1. The number ofsymmetrical cases, defined by |RS-LS| Յ 1 was determined. The association betweenclinical features (expressed by subscores) and age, duration of therapy, or their interac-tion was evaluated using multiple linear regression analysis. Statistical significance wasdefined for p Ͻ 0.05.
Out of 90 patients who were referred for evaluation by the treating psychia-trist, 75 patients (54 male and 21 females, male to female ratio (2.6 : 1) metinclusion criteria and were included in the analysis. The male predominancefound in our study population was comparable to the patient population in thehospital at the time of the study. Ten patients did not meet inclusion criteriaof parkinsonism, 2 did not stop therapy with anticholinergics and 3 refused tobe examined. The mean age of the study population was 46.0 years (standarddeviation (SD) ϭ 13.3, median age ϭ 43.0, range 21–73 years). Sixty-onepatients (81%) had been diagnosed with schizophrenia, 6 (8%) with aschizoaffective disorder and 2 (3%) with affective disorders (the remainderhad other diagnoses). Thirty-four patients (45%) were treated with haloperi-dol and the others with other DRBA’s, of whom 10 (13%) were treated withatypical neuroleptics (risperidone, clozapine or olanzapine) and 3 patientswere on a combination of two neuroleptics each. The mean duration ofexposure to neuroleptic therapy was 15.4 years (SD ϭ 11.8, range: 2 weeks–43years) and 61% of the patients were treated for longer than 10 years (Fig. 1). Sixty-six patients (87%) were treated with an anticholinergic agent, whichwas withheld at least 24 hours prior to evaluation. Only one of the patientsreported family history of parkinsonism unrelated to neuroleptic treat-ment, while 25 patients (33.3%) had a positive family history of psychiatricdisorders.
20 Number of Patients Duration of Treatment (years) Fig. 1. Duration of neuroleptic treatment among 75 patients with neuroleptic-induced parkinsonism. The mean duration of neuroleptic therapy was 15.4 years (SD ϭ 11.8,
range: 2 weeks–43 years) and 61% of the patients were treated for more than 10 years
Clinical characteristics of neuroleptic-induced parkinsonism
Most patients had only minimal disability or none at all, but drooling, tremorand speech difficulties were the most common symptoms (data not shown). Falling or prominent gait difficulties were rare (n ϭ 10 and n ϭ 9, respectively)and only two patients reported freezing of gait. The motor examination section of the UPDRS
Most patients had mild parkinsonism according to the motor examination, asreflected by the mean motor subscores (Table 1).
Sixty-six patients (88%) had a H&Y stage Յ2.5, of whom 45 were in stage 2. Unilateral cases, either with (stage 1.5, n ϭ 2) or without (stage 1, n ϭ 3) axialinvolvement were very rare (4% and 3%, respectively). Only eight patients(11%) were in stage 3, 1 patient in stage 4 and none in stage 5. The mean H&Ystage of the study population was 2.2 Ϯ 0.5.
Rest tremor was present in 44% of the patients (n ϭ 33), being more commonin the upper limbs than in the lower limbs (41% versus 20%, respectively). Only 2 patients had tremor limited to the lower limbs. In most patients (n ϭ53, 71%) tremor was strictly symmetrical and in others there was only a smalldifference between the right and left sides in severity. Tremor involving thefacial structures was present in 15 patients (20%). Action tremor of the upperlimbs was present in 44% of the patients (n ϭ 33), strongly correlating with
Table 1. The motor performance as scored in subscales of the UPDRS and the ADL
score of the UPDRS in 75 patients with NIP
8 for UPDRS items included in each subscales see text. UPDRS Unified Parkinson’s
Disease Rating Scale, ADL Activities of Daily Living, NIP Neuroleptic-induced parkin-sonism, SD standard deviation. * For the total ADL score, median ϭ 4
rest tremor in these limbs (Spearman correlation coefficient ϭ 0.5, p ϭ0.0001). Thirteen patients (17%) had action tremor of the upper limbs withoutrest tremor.
All patients exhibited rigidity, most common in the neck (93%), followed bythe upper limbs (84%) and least in the lower limbs (57%).
Gait impairment was observed in 31 patients (41%) mostly in the form of mildslowing (27 patients). Only 4 patients had clear parkinsonian gait with someshuffling and one of them could not walk unassisted. Only two patients re-ported freezing of gait, which was not seen during our exam.
Significant postural instability was observed in 9 patients (12%), while 17patients (23%) exhibited minimal impairment in the pull test.
The parkinsonian signs were symmetrical in 61% of the patients (n ϭ 46). Theright and left scores had a linear correlation with a slope of 0.95 (p ϭ 0.0001)(Fig. 2). This indicates an almost perfect symmetrical clinical picture. Upper versus lower body involvement
UBS (2.7 Ϯ 1.9, mean Ϯ SD) was significantly higher than LBS (2.1 Ϯ 1.7,mean Ϯ SD; p ϭ 0.0001; Table 1). Fig. 2. Linear regression curve of right score (RS) versus left score (LS)
Clinical characteristics of neuroleptic-induced parkinsonism
Table 2. Correlation between the motor subscales used for
* The numbers in the cells are Pearson correlation
coefficients and their corresponding p values. The correlationwas performed only for subscales which do not include com-mon items. GTS Global tremor score, GRS Global rigidityscore, GBS Global bradykinesia score, PIGD score Posturalinstability gait difficulty score, GS Gait score
Intercorrelation between parkinsonian features
All parkinsonian features correlated well with each other except betweentremor and rigidity, while correlation between tremor PIGD was borderline(Table 2). Association with age and treatment duration
Using multiple linear regression analysis we found no association between thetotal motor score and the patients’ age or duration of therapy. Neither wereany of the motor subscores (GTS, GRS, GBS, PIGD or GS) associated witheither the patient’s age or duration of neuroleptic therapy. Discussion
We describe the clinical features of 75 psychiatric in-patients with NIP.
Only 1% of our patients reported a first-degree or second-degree relative
affected with parkinsonism unrelated to neuroleptic treatment, a finding thatdoes not support an association between NIP and PD.
The severity of parkinsonian features in NIP is variable (Ayd, 1961;
Kennedy et al., 1971; Korczyn and Goldberg, 1976; Stephen and Williamson,1984; Hardie and Lees, 1988). Most patients with NIP in the study by Korczynand Goldberg were asymptomatic (Korczyn and Goldberg, 1976). InKennedy’s series (Kennedy et al., 1971), where all chronic schizophrenicpatients from two hospitals who have been treated with trifluoperazine wereassessed, extrapyramidal symptoms did have clinical significance: 14% haddressing difficulties, 27% postural abnormalities and 49% gait disturbances. These disabilities were not significantly associated with the parkinsoniansigns, but rather to other extrapyramidal motor abnormalities, like akathisia
or dyskinesia (Kennedy et al., 1971). On the contrary, in the series by Stephenand his colleagues, of symptomatic elderly patients with drug-induced parkin-sonism, many patients had severe parkinsonism, very similar to PD. Thesepatients were referred to hospitalization due to severe motor impairment. Theauthors concluded that the similarity between NIP and PD in their seriesmight be due to the fact that neuroleptics unmask latent PD, which is commonin the elderly population (Stephen and Williamson, 1984). In contrast, most ofour NIP patients had no functional disability although some were bothered bysymptoms such as speech difficulty, drooling or tremor. The methodology ofthe study may account for the preponderance of mild cases, since our patientswere selected by their psychiatrists due to signs of parkinsonism regardless ofany complaints. Although most of the patients (87%) were treated by anticho-linergics, these drugs were withdrawn 24–48 hours before evaluation; there-fore the symptomatic benefit of the anticholinergic drugs could play a minorrole by decreasing the severity of the parkinsonian signs. Except for accentua-tion of parkinsonism, anticholinergic withdrawal precipitated motor and be-havioral disorders such as restlessness and akathisia, discussion of which isbeyond the scope of this article.
The quantification of parkinsonian features in NIP patients using the
UPDRS allowed us to discriminate between upper and lower limb involve-ment, and depict the relative segmental distribution of symptoms (e.g. rightversus left or upper versus lower body involvement). Korczyn and Goldberg(1976) rated parkinsonian features of hypokinesia, rigidity, tremor, facialmask, gait disturbance, drooling and micrographia, using an arbitrary severityscale of 0–3, but the authors did not describe the relative distribution of signsin different body parts. Hardie and Lees assessed 26 patients with NIP aged 21to 71 using the Webster rating scale: they found no specific features for NIP. The findings were commonly asymmetric and tremor was of greater or equalseverity to other cardinal signs in 53% of the patients (Hardie and Lees, 1988). Kennedy and his colleagues (Kennedy et al., 1971) reported that tremor wasvery common, occurring in 88% of the patients (when doubtful and mild caseswere excluded it was 48%), and rigidity was found in 68% of the patients(38% withsignificant manifestations). In Ayd’s series tremor occurrence was60%, usually beginning in the upper limb (Ayd, 1961). These figures aresimilar to ours, where tremor prevalence was 44%.
Is NIP part of the spectrum of PD? In order to answer this question we
attempted to compare our data with similar data concerning PD patients. Inthe PD database at Columbia Presbyterian Medical Center (CPMC) in 1992the prevalence of tremor in PD was 77% (from a total of 1,347 PD patients),while in patients with drug-induced parkinsonism it was 52% (from a total ofonly 27 patients included in the analysis). Motor blocks (freezing phenom-enon) occurred in 31% (out of 1,227) of PD patients and in 8% (out of 24) ofdrug-induced parkinsonism patients. Segmental distribution cannot be com-pared since it was not reported for PD patients. However, the CPMC databasewas composed of early as well as advanced cases with a preferential referralbias of more advanced cases (Fahn, 1997). For this reason we looked at thedata reported from the Deprenyl and Tocopherol Antioxidative Therapy of
Clinical characteristics of neuroleptic-induced parkinsonism
Parkinsonism (DATATOP) study of recently diagnosed, unmedicated pa-tients. In our own present series the parkinsonism in NIP is different from thatreported from the DATATOP study, where the baseline data from earlydopa-naive PD patients is given. Most NIP patients were at H&Y stages of 2–3 and only 7% (n ϭ 5) were unilateral. In most of our cases, this implies abilateral disease with or without some postural involvement and not an ad-vanced disease. This is different from the DATATOP study where one of theinclusion criteria was H&Y stage under 2.5 and 50% of the patients had aunilateral disease – a typical feature of early PD (Jankovic et al., 1990).
The prevalence of rest tremor is lower in NIP than in PD as reflected in the
DATATOP study, where more than 70% of the patients had rest tremor(Jankovic et al., 1990). In NIP the rest tremor is usually associated with anaction component in the same limb. Many patients have an action tremoralone, an uncommon finding in PD. Upper limbs were involved significantlymore often than the lower limbs. In the DATATOP study 7.1% of the pa-tients had freezing of gait (Giladi et al., 2001), while we found 3% (n ϭ 2) inthe NIP patients. Prominent gait and postural abnormalities among patientswith NIP are uncommon as well. These differences could be partially attrib-uted to the fact that most patients had mild parkinsonism, which did notprogress to affect gait and postural reflexes in spite of long-term exposure toneuroleptics. We found no association between the severity of the parkinso-nian syndrome or any of the motor subscores to the age of the patients or theduration of therapy. The same was shown by Korczyn and Goldberg (1976). Several other authors, however, found that increasing age rather than theduration or the dosage of neuroleptic therapy was associated with increasedparkinsonian severity (Ayd, 1961; Kennedy et al., 1971; Hardie and Lees,1988).
The present study contributes little to the understanding of the basic
question of the pathogenesis of NIP. Our results do not provide furtherevidence in favor of the pathogenetic theory of neuroleptic toxicity tonigrostriatal dopaminergic system, or the unmasking of age-related dopamin-ergic system degeneration in most cases of NIP. Dopamine receptor blockadeis probably the main mechanism of NIP. Individual susceptibility to blockadeof the D dopamine receptors as well as to interactions with other neuro-
chemical circuits may be responsible for the variable severity of NIP. Thissusceptibility may be related to receptor affinity to DRBA’s, or perhapsefficiency of compensatory mechanisms that can bypass the dopaminergicblockage. Dose or potency effect of the neuroleptic agent was not assessed inour study due to the changes in medications in these hospitalized patientsmaking it one of the study’s limitations (Ayd, 1961).
In conclusion, our study showed that NIP differs from PD in terms of some
clinical symptoms. NIP is more symmetrical and tends to be associated withthe triad of bradykinesia, rigidity and tremor, while PD tends to involve gaitand posture more commonly. In contrast to PD, which worsens with time, NIPseems to be unassociated with duration of neuroleptic treatment. In spite ofthe presence of parkinsonian symptoms the functional disability and aware-ness in NIP is mild and partial. Future studies should look more carefully at
S. Hassin-Baer et al.: Clinical characteristics of NIP
the metabolic changes of brain function secondary to dopaminergic blockageby DRBA’s and specifically at possible compensatory mechanisms. References
American Psychiatric Association (1994) Diagnostic and statistical manual of mental
disorders. American Psychiatric Press, Washington DC
Ayd F (1961) A survey of drug-induced extrapyramidal reactions. JAMA (175): 102–108Burn DJ, Brooks DJ (1963) Nigral dysfunction in drug induced parkinsonism: an F-dopa
Diederich NJ, Goetz CG (1998) Drug-induced movement disorders. Neurol Clin 16(1):
Fahn S (1997) From the PD database at Columbia Presbyterian Medical Center, 1992. A
comprehensive review in movement disorders for the clinical practitioner. ColumbiaUniversity, pp 278–279
Giladi N, McDermott M, Fahn S, Prodborski S and the Parkinson study group (2001)
Freezing of gait in Parkinson’s disease. Neurology 56(12): 1712–1721
Hardie RJ, Lees AJ (1988) Neuroleptic-induced Parkinson’s syndrome: clinical features
and results of treatment with levodopa. J Neurol Neurosurg Psychiatry 51(6): 850–854
Jankovic J, McDermott M, Carter J, et al (1990) Variable expression of Parkinson’s
disease: a base-line analysis of the DATATOP cohort. The Parkinson Study Group. Neurology 40(10): 1529–1534
Kennedy PF, Hershon HI, Mcguire RJ (1971) Extrapyramidal disorders after prolonged
phenothiazine therapy. Br J Psychiatry 118(546): 509–518
Klawans HL, Bergen D, Bruyn GW (1973) Prolonged drug-induced Parkinsonism.
Korczyn AD, GJ Goldberg (1976) Extrapyramidal effects of neuroleptics. J Neurol
Lang AE, Fahn S (1989) Assessment of Parkinson’s disease. Quantification of neurologi-
cal deficit. T Munsat Stoneham, Mass, Butterworths, pp 285–309
Melamed E, Achiron A, Schapira A, Davidovicz S (1991) Persistent and progressive
parkinsonism after discontinuation of chronic neuroleptic therapy: an additionaltardive syndrome? Clin Neuropharmacol 14(3): 273–278
Rajput AH, Rozdilsky B, Hornykiewicz O, Shannak K, Lee T, Seeman P (1982) Revers-
ible drug-induced parkinsonism. Clinicopathologic study of two cases. Arch Neurol39(10): 644–646
Stephen PJ, Williamson J (1984) Drug-induced parkinsonism in the elderly. Lancet
Wilson JA, Primrose WR (1986) Drug induced parkinsonism. Br Med J (Clin Res Ed)
Authors’ address: Dr. N. Giladi, Movement Disorders Unit, Tel-Aviv Medical Cen-
ter, 6 Weizmann St., Tel-Aviv 64239, Israel, e-mail: ngiladi@tasmc.health.gov.il
Cholinergic blockade does not alter the nasalcongestive response to irritant provocation*Dennis Shusterman1, Mary-Alice Murphy2, Paula Walsh1, John R. Balmes1Division of Occupational and Environmental Medicine, University of California, San Francisco, U.S.A. Department of Pediatrics, University of California, San Francisco, U.S.A. Objective: To understand the mechanism underlying the nasal
THROMBOREDUCTIN 0.5 mg PACKAGE INSERT SCHEDULING STATUS PROPRIETARY NAME AND DOSAGE FORM COMPOSITION Each capsule contains 0.57 mg anagrelide hydrochloride equivalent to 0.5 mg anagrelide basemagnesium stearate, titanium dioxide E171, indigo carmine E 132 and gelatin. PHARMACOLOGICAL CLASSIFICATION A 8.5 Medicines acting on blood and haemopoietic system – platelet reducing agent
 Clinical characteristics of neuroleptic-induced parkinsonism
Clinical characteristics of neuroleptic-induced parkinsonism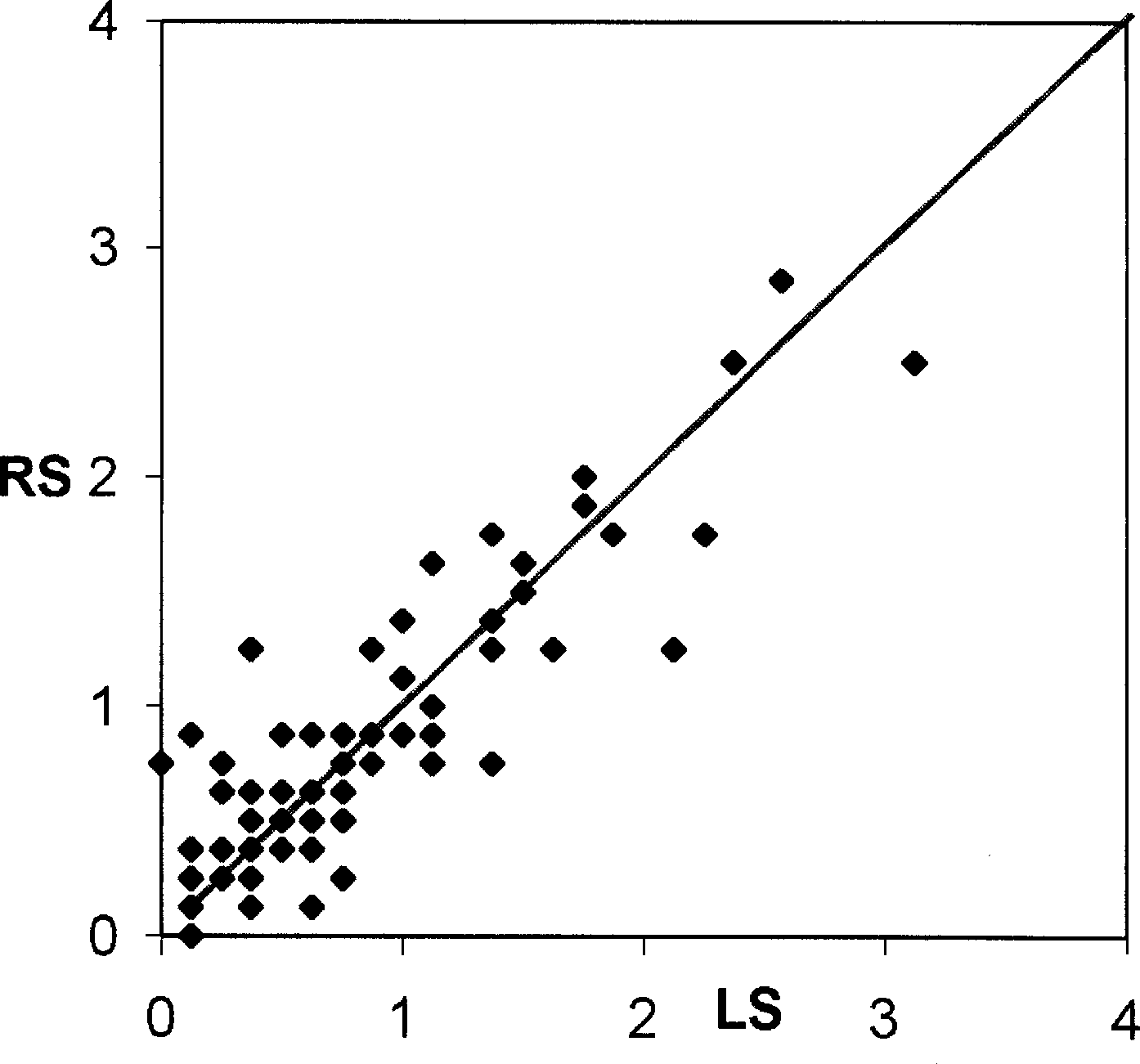 rest tremor in these limbs (Spearman correlation coefficient ϭ 0.5, p ϭ0.0001). Thirteen patients (17%) had action tremor of the upper limbs withoutrest tremor.
rest tremor in these limbs (Spearman correlation coefficient ϭ 0.5, p ϭ0.0001). Thirteen patients (17%) had action tremor of the upper limbs withoutrest tremor.