While in hospital he was observed to be physically
concentrations were 46-4 (2-6) and 22-6 (3-0) for the blue-
aggressive. He was first treated with sulpiride and diazepam,
green and special-blue groups, respectively (p<0-0001).
which led to excessive sedation interspersed with aggressive
24 h 19 of the blue-green group terminated phototherapy,
outbursts. He was transferred to a continuing care ward
whereas 10 of the special-blue group still needed light
where he continued to manifest persecutory delusions and
threatening behaviour. He was started on risperidone 0-5 mg
The success of blue-green phototherapy is mainly due to
once daily and showed much improvement, becoming
the combined effects of the increase from blue to green of
cheerful and cooperative, and joining in occupational
the quantum yield of lumirubin, responsible for the quickest
therapy for the first time. He was maintained on risperidone
pigment clearance in human beings; a corresponding
and after 3 months was sufficiently improved to be referred
decrease of ZE-BR quantum yield; and filtering effects of the
to the local authority for transfer to a community setting.
skin, which attenuates more blue than green light. Our
A 71-year-old man (case 3) with LBD for 6 years
results represent the first significant improvement of
developed marked visual and auditory hallucinations which
phototherapy efficiency following the development and
his wife found distressing and difficult to deal with. He
introduction of the special-blue lamp by Sisson in 1970, and
began attending a day hospital and was started on
is based on more than 10 years of interdisciplinary studies
risperidone 0-5 mg twice a day. His hallucinations resolved
between our groups.1,5 The phototherapy exposure time has
and his cognitive functioning improved. There was no
now been reduced to 1 day in the majority of preterm
determination in his rigid-akinetic syndrome apart from
infants, ensuring less stress to the infant and less interference
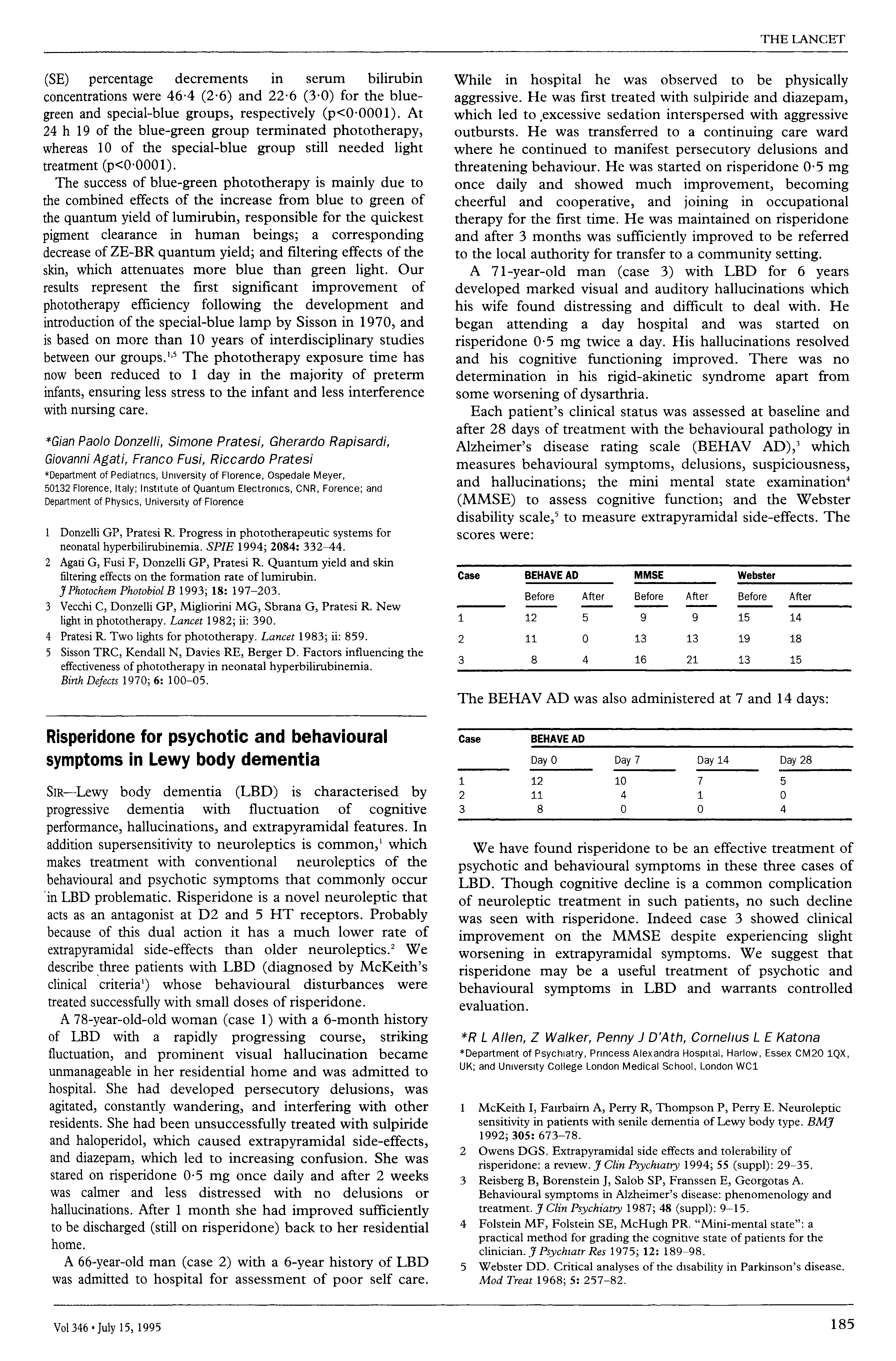
Each patient’s clinical status was assessed at baseline and
after 28 days of treatment with the behavioural pathology in
*Gian Paolo Donzelli, Simone Pratesi, Gherardo Rapisardi,
Alzheimer’s disease rating scale (BEHAV AD),3 which
Giovanni Agati, Franco Fusi, Riccardo Pratesi
measures behavioural symptoms, delusions, suspiciousness,
*Department of Pediatrics, University of Florence, Ospedale Meyer,
and hallucinations; the mini mental state examination4
50132 Florence, Italy; Institute of Quantum Electronics, CNR, Forence; andDepartment of Physics, University of Florence
(MMSE) to assess cognitive function; and the Webster
disability sealer to measure extrapyramidal side-effects. The
1 Donzelli GP, Pratesi R. Progress in phototherapeutic systems for
neonatal hyperbilirubinemia. SPIE 1994; 2084: 332-44.
2 Agati G, Fusi F, Donzelli GP, Pratesi R. Quantum yield and skin
filtering effects on the formation rate of lumirubin. J Photochem Photobiol B 1993; 18: 197-203.
3 Vecchi C, Donzelli GP, Migliorini MG, Sbrana G, Pratesi R. New
light in phototherapy. Lancet 1982; ii: 390.
4 Pratesi R. Two lights for phototherapy. Lancet 1983; ii: 859. 5 Sisson TRC, Kendall N, Davies RE, Berger D. Factors influencing the
effectiveness of phototherapy in neonatal hyperbilirubinemia. Birth Defects 1970; 6: 100-05.
Risperidone for psychotic and behaviouralsymptoms in Lewy body dementia
SIR-Lewy body dementia (LBD) is characterised byprogressive dementia with fluctuation
performance, hallucinations, and extrapyramidal features. In
addition supersensitivity to neuroleptics is common,’ which
We have found risperidone to be an effective treatment of
psychotic and behavioural symptoms in these three cases of
behavioural and psychotic symptoms that commonly occur
LBD. Though cognitive decline is a common complication
in LBD problematic. Risperidone is a novel neuroleptic that
of neuroleptic treatment in such patients, no such decline
acts as an antagonist at D2 and 5 HT receptors. Probably
was seen with risperidone. Indeed case 3 showed clinical
because of this dual action it has a much lower rate of
improvement on the MMSE despite experiencing slight
extrapyramidal side-effects than older neuroleptics.2 We
worsening in extrapyramidal symptoms. We suggest that
describe three patients with LBD (diagnosed by McKeith’s
risperidone may be a useful treatment of psychotic and
clinical criteria’) whose behavioural disturbances were
behavioural symptoms in LBD and warrants controlled
treated successfully with small doses of risperidone.
A 78-year-old-old woman (case 1) with a 6-month history
of LBD with a rapidly progressing course, striking
*R L Allen, Z Walker, Penny J D’Ath, Cornelius L E Katona
fluctuation, and prominent visual hallucination became
*Department of Psychiatry, Princess Alexandra Hospital, Harlow, Essex CM20 1QX,
unmanageable in her residential home and
UK; and University College London Medical School, London WC1
hospital. She had developed persecutory delusions, was
agitated, constantly wandering, and interfering with other
McKeith I, Fairbairn A, Perry R, Thompson P, Perry E. Neuroleptic
residents. She had been unsuccessfully treated with sulpiride
sensitivity in patients with senile dementia of Lewy body type. BMJ
2 Owens DGS. Extrapyramidal side effects and
diazepam, which led to increasing confusion. She was
stared on risperidone 0-5 mg once daily and after 2 weeks
3 Reisberg B, Borenstein J, Salob SP, Franssen E, Georgotas A.
was calmer and less distressed with no delusions or
Behavioural symptoms in Alzheimer’s disease: phenomenology and
hallucinations. After 1 month she had improved sufficiently
treatment. J Clin Psychiatry 1987; 48 (suppl): 9-15.
McHugh PR. "Mini-mental state": a
practical method for grading the cognitive state of patients for the
A 66-year-old man (case 2) with a 6-year history of LBD
Webster DD. Critical analyses of the disability in Parkinson’s disease.
was admitted to hospital for assessment of poor self care.
M E R I D I A N P S Y C H O L O G I C A L A S S O C I A T E S 4401 North Central Avenue Indianapolis IN 46205 (317) 923-2333 FAX (317) 923-2333 mcgreene@yahoo.com Dennis Mac Greene, Ph.D., HSPP Indiana License #: 20041237 National Register of Health Service Providers in Psychology #44394 Mailing Address: 1992 Ph.D. Clinical Psychology, Rutgers University, Brunswick, NJ 1989-
Le développement de la recherche chez les cliniciens : d'abord questionner la pratique clinique Extrait du Espace d'échanges du site IDRES sur la systémique Le développement de la recherche chez les cliniciens : d'abord questionner la pratique clinique - SAVOIR THÉORIQUE - Échanges à partir d'articles , bibliothèque, dictionnaire et concepts de la systémique - Article d
 While in hospital he was observed to be physically
concentrations were 46-4 (2-6) and 22-6 (3-0) for the blue-
aggressive. He was first treated with sulpiride and diazepam,
green and special-blue groups, respectively (p<0-0001).
which led to excessive sedation interspersed with aggressive
24 h 19 of the blue-green group terminated phototherapy,
outbursts. He was transferred to a continuing care ward
whereas 10 of the special-blue group still needed light
where he continued to manifest persecutory delusions and
threatening behaviour. He was started on risperidone 0-5 mg
The success of blue-green phototherapy is mainly due to
once daily and showed much improvement, becoming
the combined effects of the increase from blue to green of
cheerful and cooperative, and joining in occupational
the quantum yield of lumirubin, responsible for the quickest
therapy for the first time. He was maintained on risperidone
pigment clearance in human beings; a corresponding
and after 3 months was sufficiently improved to be referred
decrease of ZE-BR quantum yield; and filtering effects of the
to the local authority for transfer to a community setting.
While in hospital he was observed to be physically
concentrations were 46-4 (2-6) and 22-6 (3-0) for the blue-
aggressive. He was first treated with sulpiride and diazepam,
green and special-blue groups, respectively (p<0-0001).
which led to excessive sedation interspersed with aggressive
24 h 19 of the blue-green group terminated phototherapy,
outbursts. He was transferred to a continuing care ward
whereas 10 of the special-blue group still needed light
where he continued to manifest persecutory delusions and
threatening behaviour. He was started on risperidone 0-5 mg
The success of blue-green phototherapy is mainly due to
once daily and showed much improvement, becoming
the combined effects of the increase from blue to green of
cheerful and cooperative, and joining in occupational
the quantum yield of lumirubin, responsible for the quickest
therapy for the first time. He was maintained on risperidone
pigment clearance in human beings; a corresponding
and after 3 months was sufficiently improved to be referred
decrease of ZE-BR quantum yield; and filtering effects of the
to the local authority for transfer to a community setting.