Is static hyperinflation a limiting factor during exercise in adolescents with cystic fibrosis?
Is Static Hyperinflation a Limiting Factor During Exercise
M.S. Werkman, MSc, PT,1 H.J. Hulzebos, PhD, MSc, PT,1* H.G.M. Arets, MD, PhD,2
PhD, PT, PCS,1 P.J.M. Helders, PhD, MSc, PT, PCS,1 and T. Takken, PhD, MSc
Summary. Increased work of breathing is considered to be a limiting factor in patients with cysticfibrosis (CF) performing aerobic exercise. We hypothesized that adolescents with CF and withstatic hyperinflation are more prone to a ventilatorily limited exercise capacity than non-statichyperinflated adolescents with CF.
Exercise data of 119 adolescents with CF [range 12–18 years], stratified for static hyperinflation,
defined as ratio of residual volume to total lung capacity (RV/TLC) > 30%, were obtained during aprogressive bicycle ergometer test with gas analysis and analyzed for ventilatory limitation.
Static hyperinflation showed a significant, though weak association (F 0.38; P < 0.001) with a
ventilatorily limited exercise capacity (breathing reserve index at maximal effort >0.70;FEV1 < 80% predicted and reduced exercise capacity, defined as VO2peak < 85% predicted). Analysis of association for increasing degrees of hyperinflation showed an increase to F 0.49(P < 0.001) for RV/TLC > 50%. In adolescents with static hyperinflation, peak work rate (Wpeak;3.1 Æ 0.7 W/kg (75.1 Æ 17.3% of predicted), peak oxygen uptake (VO2peak/kg (ml/min/kg);39.2 Æ 9.2 ml/min/kg (91.0 Æ 20.3% of predicted), peak heart rate (HRpeak; 176 Æ 19 beats/min)were significantly (P < 0.05) decreased when compared with non-static hyperinflated adolescents(Wpeak 3.5 Æ 0.5 W/kg (81.4 Æ 10.0% of predicted)); VO2peak/kg (ml/min/kg); 43.1 Æ 7.5 ml/min/kg(98.0 Æ 15.1% of predicted); and HRpeak 185 Æ 14 beats/min). Additionally, no difference was foundin the degree of association of FEV1 (%) and RV/TLC (%) with VO2peak/kgpred and Wpeak/kgPred, butwe found the RV/TLC (%) to be a slightly stronger predictor of VO2peak/kgpred and Wpeak/kgPred thanFEV1 (%).
These results indicate that the presence of static hyperinflation in adolescents with CF by
nnitself does not strongly influence ventilatory constraints during exercise and that statichyperinflation is only a slightly stronger predictor of Wpeak/kgPred and VO2peak/kgPred than airflowobstruction (FEV1 (%)). Pediatr Pulmonol. ß 2010 Wiley-Liss, Inc.
Key words: work of breathing; ventilatory limitation; cardiopulmonary exercise testing.
Funding source: Committee on Physiotherapy Research of the Royal Dutch Society for
Physiotherapy (Wetenschappelijk College Fysiotherapie, KoninklijkNederlands Genootschap voor Fysiotherapie (KNGF)).
inspiratory capacity (IC) during exercise,12 children withCF develop a rapid breathing pattern during exercise
Limitation of exercise capacity in adolescents with
with a concomitant increase in the work of breathing
cystic fibrosis (CF) has a multi-factorial cause. Reduced
(WOB)13–15 and oxygen cost.13 A decreased inspiratory
lung function and muscle mass are known to be mostimportant factors leading to a limited exercise capacity.1,2
1Child Development & Exercise Center, Cystic Fibrosis Center, University
A decreased muscle mass reduces skeletal muscle
Medical Center Utrecht, Utrecht, the Netherlands.
function, including respiratory muscle strength, in adultswith CF.3 Moreover, in children with CF a decreased
2Department of Pediatric Respiratory Medicine, Cystic Fibrosis Center,
skeletal muscle strength4,5 and endurance6 have been
University Medical Center Utrecht, Utrecht, the Netherlands.
reported, even when corrected for a decreased lean body
*Correspondence to: H.J. Hulzebos, PhD, MSc, PT, Child Development &
mass or lung function.4–6 This points to a possible
Exercise Center, University Medical Center Utrecht, PO Box 85090, 3508
intrinsic abnormality in muscle oxygen uptake in patients
AB Utrecht, the Netherlands. E-mail: h.hulzebos@umcutrecht.nl
with CF, however, currently there is no firm evidenceavailable.7–11
Received 18 December 2009; Revised 9 June 2010; Accepted 26 June 2010.
Due to continuous airflow obstruction, as reflected by a
decreased forced expiratory volume in 1 sec (FEV1), and
dynamic hyperinflation, as reflected by a decreasing
muscle function (strength and endurance) that has been
(800 mg), using a pneumotach system and a volume-
observed in patients with CF will lead to a faster
constant plethysmograph (Master Lab system, E. Jaeger,
inspiratory muscle fatigue during exercise, which con-
tributes to the reduced exercise capacity.16,17
Lung function measurements included total lung
It seems that there is an interrelationship between lung
capacity (TLC), residual volume (RV), and forced expira-
function, muscle mass, energy expenditure (respiratory),
tory volume in 1 sec (FEV1). The results were compared
muscle function, and exercise capacity in patients with
with predicted values for healthy subjects matched for age,
The objective of the current study was to investigate
whether static hyperinflation makes adolescents with CF
more prone to a ventilatory limitation during exercise. We
Exercise capacity was assessed using a progressive
hypothesized that adolescents with static hyperinflation
CPET. CPET, after brochodilation with salbutamol,
are more prone to a ventilatorily limited exercise capacity
performed on an electronically braked cycle ergometer
than non-static hyperinflated adolescents with CF. Fur-
(Jaeger physis; Carefusion, Houten, the Netherlands). The
thermore, we questioned if the amount of static hyper-
seat height was adjusted to the participant’s comfort and
inflation (RV/TLC (%)) is a stronger predictor of exercise
leg length. Participants rested until all measured variables
capacity than the degree of airflow obstruction FEV1
were stable. Cycling started at a workload of 0 W; the
workload was incremented with 15 W/min until thepatient stopped due to volitional exhaustion. The work-
load which could be overcome for the last 30 sec prior to
exhaustion was considered to be the Wpeak. Determinationif a participants’ effort was maximal was based on
Adolescents with CF (n ¼ 119) of the Cystic Fibrosis
subjective and objective criteria. Subjective criteria are
Center of the University Children’s Hospital and Medical
described as ‘‘unsteady biking,’’ ‘‘sweating,’’ ‘‘facial
Center Utrecht, the Netherlands, were measured for body
flushing,’’ and ‘‘clear unwillingness to continue despite
weight, height, lung function, and exercise capacity as part
encouragement.’’ Objective criteria were: [1] peak heart
of routine assessment measures at the annual medical
check-up. All measurements were part of usual care,
exchange ratio (RER) > 1.00. Based on previous liter-
according to the policy of the medical ethical committee
ature, we defined that a participant had to meet the
of the University Medical Center Utrecht, ethical approval
subjective criteria and at least one out of two objective
and informed consent were not obliged. Data of the initial
criteria for the test to be considered of maximal effort and
test of each participant (between 1998 and 2006) were
character.22 Participants breathed through a mask that was
selected for this study. Participants were stratified into
connected to a calibrated metabolic cart (Oxycon pro,
static hyperinflated and non-static hyperinflated. Conform
Carefusion). Expired gas was passed through a flow meter,
previous literature about children with asthma, we defined
oxygen analyzer, and a carbon dioxide analyzer. The flow
a ratio of residual volume to total lung capacity (RV/TLC),
meter and gas analyzer were connected to a computer,
after using a bronchodilator, higher than 30% as moderate
which calculated breath-by-breath minute ventilation
to severe hyperinflation.19 Analysis for increasing degrees
of static hyperinflation was performed by including only
patients with a certain level of static hyperinflation in the
2), and RER from conventional equations. Relative
analysis (RV/TLC >30%, >35%, >40%, >45%, and
2peak by total body mass. HR was monitored
continuously by a three-lead electrocardiogram (Hewlett-
The definition used for determination of a ventilatory
Packard, Amstelveen, the Netherlands).
limitation during cardiopulmonary exercise test (CPET)was previously used by Sexauer et al.20 including: [1]
breathing reserve index at maximal effort >0.70 (calcu-lated as peak minute ventilation (VE
maximal voluntary ventilation (MVV) were MVV is
children and adolescents were obtained from previously
studied Dutch children and adolescents.23,24
and [3] a reduced exercise capacity, defined asVO
Data were expressed as mean Æ SD. Data were
analyzed using SPSS 15.0 for Windows and tested for
Spirometry and body plethysmography were performed
normality with the Kolmogorov–Smirnov test. An alpha
before and after bronchodilation with salbutamol
value of 0.05 was considered as statistically significant.
BM, body mass; BMI, body mass index; RV/TLC, ratio residual volume/total lung capacity; FEV1, forced expiration volume in 1 sec; HR, heart rate;RER, respiratory exchange ratio (VCO2/VO2); VO2peak, peak oxygen uptake; Wpeak, peak work rate; VEpeak, minute ventilation at maximal effort. Values are presented as means Æ SD. 1Significant difference between gender groups (P < 0.05): non-parametric tested with Mann–Whitney U-test. 2Significant difference between gender groups (P < 0.001). 3Significant difference between gender groups (P < 0.01). 4Significant difference between gender groups (P < 0.05).
Possible differences between groups in the CF population
inflated and non-static hyperinflated adolescents with CF
were analyzed using one-way ANOVA when normally
are shown in Table 2. VO2peak/kg, Wpeak/kg, VEpeak, and
distributed and with the Mann–Whitney U-test when not
HRpeak were all significantly lower in static hyperinflated
normally distributed. Dichotomy variables were tested for
patients compared to the non-hyperinflated patients
association using the phi coefficient (F), and tested for
(P < 0.05). Corrected for age and gender, the differences
significance using chi-square test. Prognostic value of
in VO2peak/kgPred (98.0 Æ 15.1% in non-static hyper-
FEV1 and RV/TLC for exercise capacity was analyzed
inflated and 91.0 Æ 20.3% in static hyperinflated patients;
using standard multiple regression analysis.
P < 0.05), and in Wpeak/kgPred (75.1 Æ 17.3 (%) in statichyperinflated and 81.4 Æ 10.0 (%) in non-static hyper-
inflated patients; P < 0.05) remained (Table 2).
After determination of maximal effort and screening
TABLE 2— Exercise Capacity in Static Hyperinflated andNon-Static Hyperinflated Patients With CF
for completeness of data set, in total 119 adolescents,50 females and 69 males were included.
Mean age was 13.8 years Æ 1.7 (range 12–18 years),
and anthropometric values did not differ according to
gender (Table 1). All measurements were obtained after
Overall, 54 (40.3%) patients were non-static hyper-
HRpeak, peak heart rate; RERpeak, respiratory exchange ratio at peak
inflated (20,; 34<; RV/TLC (%) 23.4 Æ 3.4; FEV
peak, peak minute ventilation; VO2peak/kg, peak oxygen
(%pred) 97.0 Æ 13.6), whereas 65 (48.5%) patients were
uptake per kilogram body mass; Wpeak/kg, peak work rate per kilogrambody mass.
identified as static hyperinflated (30,; 35<; RV/TLC (%)
Values are presented as means Æ SD.
P < 0.05 non-parametric tested with Mann–Whitney U-test.
parameters and ventilatory parameters in static hyper-
TABLE 3— Correlation Between Static Hyperinflation and
Ventilatory Limitation for Different Degrees ofHyperinflation
As presented in Figure 1, baseline FEV1 (%pred) after
bronchodilator, showed a fair degree of association with
VO2peak/kgPred and Wpeak/kgPred (r ¼ 0.44 and r ¼ 0.46,
respectively (both P < 0.001), where RV/TLC, after
bronchodilator, showed more variable degrees of associ-
ation (r ¼ À0.43 and r ¼ À0.47, respectively (both
P < 0.001) after bronchodilator). There was a strong
association between FEV1 (%pred) and RV/TLC after
RV/TLC, residual volume/total lung capacity.
bronchodilator (r ¼ À0.84; P < 0.001).
Values are Phi correlation coefficients with P-value.
Multiple linear regression showed that, compared to
FEV1 (%pred), RV/TLC (%) was a somewhat strongerpredictor for Wpeak/kgPred (FEV1 (%pred) B 0.161 and b
Ventilatory Versus Non-Ventilatory Limitation
0.227 (P ¼ 0.135); RV/TLC (%) B À0.371 and b À0.273(P ¼ 0.073)) and VO
Twenty (29.4%; 7,; 13<) out of the 65 patients with
static hyperinflation were ventilatorily limited during
exercise while only 1 (1<) of the 54 patients without statichyperinflation was ventilatorily limited during exercise.
Phi coefficient (F) between ventilatory limitation andstatic hyperinflation was 0.38 (P < 0.001; see Table 3).
We hypothesized that adolescents with CF with static
Furthermore, for increasing degrees of hyperinflation, Phi
hyperinflation are more prone for a ventilatorily limited
coefficient increased to 0.52 (P < 0.001) in the RV/TLC
aerobic exercise capacity compared with non-static
hyperinflated adolescents. We found a significant, but
Fig. 1. Associations between lung function parameters and exercise capacity.
weak association (F 0.38; P < 0.001) between static
cise.15 Moreover, the greater fatigability of the inspiratory
hyperinflation (RV/TLC > 30%) and ventilatory limita-
muscles could hypothetically induce a reflex vasocon-
tion at peak exercise. This indicates that the presence of
striction in the peripheral locomotor muscles and thereby
static hyperinflation in adolescents with CF by itself does
compromises blood flow to the exercising limbs.17
not strongly influence ventilatory constraints during
Furthermore, the increase in WOB in patients with CF
exercise, which is in line with previous research.20
as a possible factor in ventilatorily limited exercise
Sexauer et al.20 found an odds ratio of 0.96 (P ¼ 0.76)
capacity could theoretically be elicited by the develop-
for the RV/TLC ratio at rest as a weak non-significant
ment of dynamic hyperinflation during exercise, instead of
predictor for ventilatory limitation in adults with CF.
the presence of static hyperinflation at rest.
Confirmative results were found in a study among adult
Beside the FEV1 and possible dynamic hyperinflation,
COPD patients, were the change in IC during exercise,
other factors, such as nutritional status, muscle mass,
reflecting dynamic hyperinflation, has been shown to be
respiratory and peripheral muscle strength, and habitual
superior to static hyperinflation (resting IC) in estimating
daily physical activity are also important predictors of
Moreover, after analysis of the association between the
After all we suggest that, in future research, beside
degrees of static hyperinflation and a ventilatorily limited
standard anthropometric and lung function measures,
exercise capacity, the correlation coefficient slightly
dynamic hyperinflation and flow–volume curves during
increased from 0.38 to 0.49 for RV/TLC >30% and
exercise should be measured to facilitate a better under-
standing of the role of increased WOB as possible limiting
Additionally, we found no difference in the degree of
factor in the exercise capacity of patients with CF.
association of baseline FEV1 (%pred) and RV/TLC (%),after bronchodilator, with VO2peak/kgPred and Wpeak/
kgPred, however, RV/TLC (%) was a slightly strongerpredictor of VO
This study was funded by an unconditional research
grant (DO-IT) from the Committee on Physiotherapy
A point of discussion in the present study is the cut-off
Research of the Royal Dutch Society for Physiotherapy
point in breathing reserve used to determine ventilatory
(Wetenschappelijk College Fysiotherapie, Koninklijk
limitation. Prioux et al. suggested a ventilatory reserve at
Nederlands Genootschap voor Fysiotherapie (KNGF)).
peak exercise of 20% (MVV-VE/MVV Â 100%), with a
All measurements used in data analysis are part of
corresponding breathing reserve 0.8, in 11-year-old
standard routine care at the Cystic Fibrosis Center of the
children, which increased to 30% (corresponding breath-
University Children’s Hospital and Medical Center
ing reserve 0.7) at the age of 16 years. The mean age of our
patients is 14 years, which could have influenced theprevalence of ventilatory limitation as we have used
breathing reserve >0.7 as cut-off point.26 Furthermore,due to the narrow age range of our population, the present
1. Shah AR, Gozal D, Keens TG. Determinants of aerobic and
results could not be extrapolated to patients that are
anaerobic exercise performance in cystic fibrosis. Am J RespirCrit Care Med 1998;157:1145–1150.
2. Klijn PHC, van der Net J, Kimpen JL, Helders PJM, van der Ent
Based on the results we conclude that the presence
CK. Longitudinal determinants of peak aerobic performance in
children with cystic fibrosis. Chest 2003;124:2215–2219.
TLC > 30%) in adolescents with CF by itself does not
3. Ionescu AA, Chatham K, Davies CA, Nixon LS, Enright S, Shale
strongly influence ventilatory constraints during exercise
DJ. Inspiratory muscle function and body composition in cysticfibrosis. Am J Respir Crit Care Med 1998;158:1271 –1276.
and that static hyperinflation, as reflected by RV/TLC (%),
4. de Meer K, Gulmans VAM, van der Laag J. Peripheral muscle
is only a slightly stronger predictor of Wpeak/kgPred and
weakness and exercise capacity in children with cystic fibrosis.
VO2peak/kgPred than the FEV1 (%pred), which is only
Am J Respir Crit Care Med 1999;159:748–754.
reflecting the degree of airflow obstruction. The decreased
5. Hussey J, Gormley J, Leen G, Greally P. Peripheral muscle
exercise capacity in static hyperinflated adolescents could
strength in young males with cystic fibrosis. J Cystic Fibrosis2002;1:116–121.
be explained by faster termination of peak exercise due to
6. Sahlberg ME, Svantesson U, Magnusson Thomas EML, Strand-
preliminary inspiratory muscle fatigue. The preliminary
vik B. Muscular strength and function in patients with cystic
inspiratory muscle fatigue could be induced by the
fibrosis. Chest 2005;127:1587–1592.
development of dynamic hyperinflation.14,15,24 which
7. Moser C, Tirakitsoontorn P, Nussbaum E, Newcomb R, Cooper
increases work12–15 and oxygen cost of breathing13 and
DM. Muscle size and cardiorespiratory response to exercise incystic fibrosis. Am J Respir Crit Care Med 2000;162:1823–1827.
causing intrapulmonary gas trapping and ventilation/
8. de Meer K, Jeneson JAL, Gulmans VAM, van der Laag J, Berger
perfusion mismatching,27 which make a patient with CF
R. Efficiency of oxidative work performance of skeletal muscle in
more susceptible to ventilatory limitation during exer-
patients with cystic fibrosis. Thorax 1995;50:980–983.
9. Hjeltnes N, Stanghelle JK, Skyberg D. Pulmonary function and
20. Sexauer WP, Cheng H-K, Fiel SB. Utility of the breathing reserve
oxygen uptake during exercise in 16 year old boys with cystic
index at the anaerobic threshold in determining ventilatory-
fibrosis. Acta Paediatr Scand 1984;73:548–553.
limited exercise in adult cystic fibrosis patients. Chest 2003;124:
10. Hebestreit H, Hebestreit A, Trusen A, Hughson RL. Oxygen
uptake kinetics are slowed in cystic fibrosis. Med Sci Sports Exerc
21. Zapletal A, Samanek M, Paul T. Lung function in children and
adolescents: methods, reference values. In: Zapletal A, editor.
11. Rosenthal M, Narang I, Edwards L, Bush A. Non-invasive
Progress in respiration research, Vol. 22. Basel: Karger; 1987.
assessment of exercise performance in children with cystic
fibrosis (CF) and non-cystic fibrosis bronchiectasis: is there a
22. de Groot JF, Takken T, de Graaff S, Gooskens RHJM, Helders
CF specific muscle defect? Pediatr Pulmonol 2009;44:222–
PJM, Vanhees L. Treadmill testing of children who have
spina bifida and are ambulatory Does peak oxygen uptake reflect
12. Loring SH, Garcia-Jaques M, Malhotra A. Pulmonary character-
maximum oxygen uptake? Phys Ther 2009;89:679–687.
istics in COPD and mechanisms of increased work of breathing.
23. Gulmans VA, de Meer K, Binkhorst RA, Helders PJ, Saris WH.
Reference values for maximum work capacity in relation to body
13. Gibson GJ. Pulmonary hyperinflation a clinical overview. Eur
composition in healthy Dutch children. Eur Respir J 1997;10:94–97.
24. Saris WHM, Noordeloos AM, Rignalda BEM, van’t Hof MA,
14. Keochkerian D, Chlif M, Delanaud S, Gauthier R, Maingourd Y,
Binkhorst RA. Reference values for aerobic power of healthy 4 to
Ahmaidi S. Timing and driving components of the breathing
18 year old Dutch children. In: Binkhorst RA, Kemper HGC,
strategy in children with cystic fibrosis during exercise. Pediatr
Saris WHM, editors. Children and exercise. XI. International
Series on Sport Sciences, Vol. 15. Champaign, IL: Human
15. Keochkerian D, Chlif M, Delanaud S, Gauthier R, Maingourd Y,
Ahmaidi S. Breathing pattern adopted by children with cystic
25. O’Donnell DE, Revill SM, Webb KA. Dynamic hyperinflation
fibrosis with mild to moderate pulmonary impairment during
and exercise intolerance in chronic obstructive pulmonary
exercise. Respiration 2008;75:170–177.
disease. Am J Respir Crit Care Med 2001;164:770–777.
16. Enright S, Chatham K, Ionescu AA, Unnithan VB, Shale DJ.
26. Prioux J, Matecki S, Amsallem F, Denjean A, Ramonatxo M,
Inspiratory muscle training improves lung function and exercise
et le. ‘‘Groype EFR pe´diatriques’’ de la socie´te de physiologie.
capacity in adults with cystic fibrosis. Chest 2004;126:405–
La response ventilatoire a` l’exercise maximal chez l’enfant sain.
17. Dempsey JA, Romer L, Rodmann J, Miller J, Smith C. Con-
27. Hart N, Polkey MI, Cle´ment A, Boule´ M, Moxham J, Lofaso F,
sequences of exercise-induced respiratory muscle work. Respir
Fauroux B, Changes in pulmonary mechanics with increasing
Physiol Neurobiol 2006;151:242–250.
disease severity in children and young adults with cystic fibrosis.
18. Scho¨ni MH, Casaulta-Aebischer C. Nutrition and lung function in
Am J Respir Crit Care Med 2002;166:61–66.
cystic fibrosis patients: review. Clin Nutr 2000;19:79–85.
28. Lands L, Desmond KJ, Demizio D, Pavilanis A, Coates AL. The
19. Eid N, Yandell B, Howell L, Eddy M, Sheikh S. Can peak
effects of nutritional status and hyperinflation on respiratory
expiratory flow predict airflow obstruction in children with
muscle strength in children and young adults. Am Rev of Respir
asthma? Pediatrics 2000;105:354–358.
For a CME/CEU version of this article please go to http://www.namcp.org/cmeonline.htm, and then click the activity title. Multiple sclerosis (MS) is a common cause of disability in young adults. Althoughnot curable, effective immunomodulators, which alter the development of disabil-ity, are available and should be initiated early in the disease process. Optimizingcare of patients with MS requi
Presence of a Na1-stimulated P-type ATPase in the plasmamembrane of the alkaliphilic halotolerant cyanobacteriumAphanothece halophyticaKanjana Wiangnon1, Wuttinun Raksajit1 & Aran Incharoensakdi1,21Department of Biochemistry, Faculty of Science, Chulalongkorn University, Bangkok, Thailand; and 2Center for Environmental Stress Tolerance inPlants, Faculty of Science, Chulalongkorn University
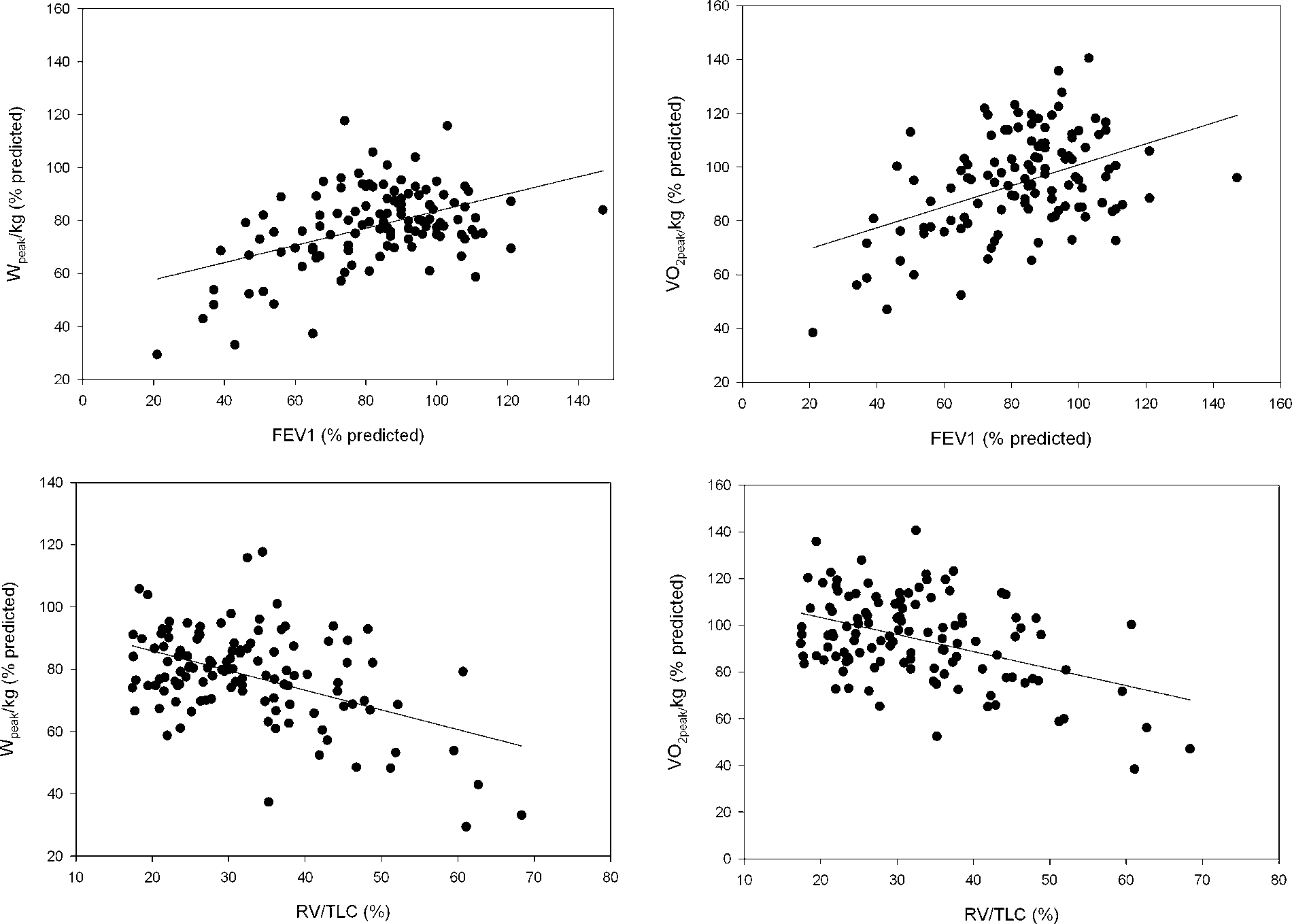 TABLE 3— Correlation Between Static Hyperinflation and
Ventilatory Limitation for Different Degrees ofHyperinflation
As presented in Figure 1, baseline FEV1 (%pred) after
bronchodilator, showed a fair degree of association with
VO2peak/kgPred and Wpeak/kgPred (r ¼ 0.44 and r ¼ 0.46,
respectively (both P < 0.001), where RV/TLC, after
bronchodilator, showed more variable degrees of associ-
ation (r ¼ À0.43 and r ¼ À0.47, respectively (both
P < 0.001) after bronchodilator). There was a strong
association between FEV1 (%pred) and RV/TLC after
RV/TLC, residual volume/total lung capacity.
TABLE 3— Correlation Between Static Hyperinflation and
Ventilatory Limitation for Different Degrees ofHyperinflation
As presented in Figure 1, baseline FEV1 (%pred) after
bronchodilator, showed a fair degree of association with
VO2peak/kgPred and Wpeak/kgPred (r ¼ 0.44 and r ¼ 0.46,
respectively (both P < 0.001), where RV/TLC, after
bronchodilator, showed more variable degrees of associ-
ation (r ¼ À0.43 and r ¼ À0.47, respectively (both
P < 0.001) after bronchodilator). There was a strong
association between FEV1 (%pred) and RV/TLC after
RV/TLC, residual volume/total lung capacity.